The application of molecular genetic tests using paraffin‑embedded biopsy specimens in the diagnosis of bone and joint tuberculosis



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
The application of molecular genetic tests using paraffin‑embedded biopsy specimens in the diagnosis of bone and joint tuberculosis
A total of 2% of tuberculosis cases involve bone and joint tuberculosis, which is the third most common extrapulmonary localization of the disease.1,2 In Poland, 32 new cases of bone and joint tuberculosis were reported in 2019, including 14 patients with spinal tuberculosis, which constitutes 13% of extrapulmonary tuberculosis cases.3 In clinical practice, pediatricians encounter bone and joint tuberculosis less frequently. Tuberculosis has become a disease somewhat less significant, often not even considered in the diagnostic workup.4 Diagnostic assessment is based on microbiological tests and detection of typical granulomas in pathological examination. To confirm the etiology of lesions, molecular testing for the presence of the Mycobacterium tuberculosis complex with the use of fresh specimen or paraffin‑embedded specimen blocks is recommended.5 The rapid Xpert MTB/RIF assay allows clinicians to detect the genetic material of the bacilli within 2 hours.4
A 16‑year‑old, BCG‑vaccinated male patient without confirmed exposure to tuberculosis reported lumbar pain since November 2019. No lung parenchyma lesions were seen on the chest X‑ray or computed tomography, and abdominal ultrasound did not reveal any abnormalities. A contrast‑enhanced magnetic resonance imaging (MRI) of the chest was performed, which showed bone marrow edema and increased contrast uptake in vertebral end plates (Th11 and Th12 vertebrae) as well as end plate erosions similar to Schmorl nodes (Figure 1A and 1B). After a week since the initial assessment, rapid worsening of health status was observed, with fever and markedly elevated inflammatory markers (C‑reactive protein, 168 mg/l [reference range, 0–10 mg/l], procalcitonin, 17 ng/ml [reference range, 0.05–0.1 ng/ml]). In blood cultures, only coagulase‑negative staphylococci were detected. Clindamycin treatment was started as standard therapy used to prevent and treat infections. The main advantages of clindamycin are its high bioavailability and good distribution to the bone. Neurological and ophthalmological consultations did not reveal any abnormalities. The tuberculosis skin test (TST) and the interferon‑gamma release assay (IGRA; T‑SPOT.TB) were negative. After 2 months, another MRI scan was performed and progression of lesions at Th11 and Th12 vertebrae was observed (Figure 1C and 1D). Following an orthopedic consultation, further antibiotic therapy was recommended along with a Jewett spinal brace to be used for 3 to 4 months. The patient underwent a biopsy of vertebral bodies and soft tissue. Histological analysis revealed a non‑neoplastic inflammatory process and presence of eosinophils; M. tuberculosis was not detected in microbiological tests. Spinal MRI performed 5 months after the initial assessment revealed inflammatory infiltration and intervertebral disc abscess at Th11 and Th12 vertebrae as well as fluid collection within the soft tissue at Th10 through Th12 vertebrae (Figure 1E and 1F).
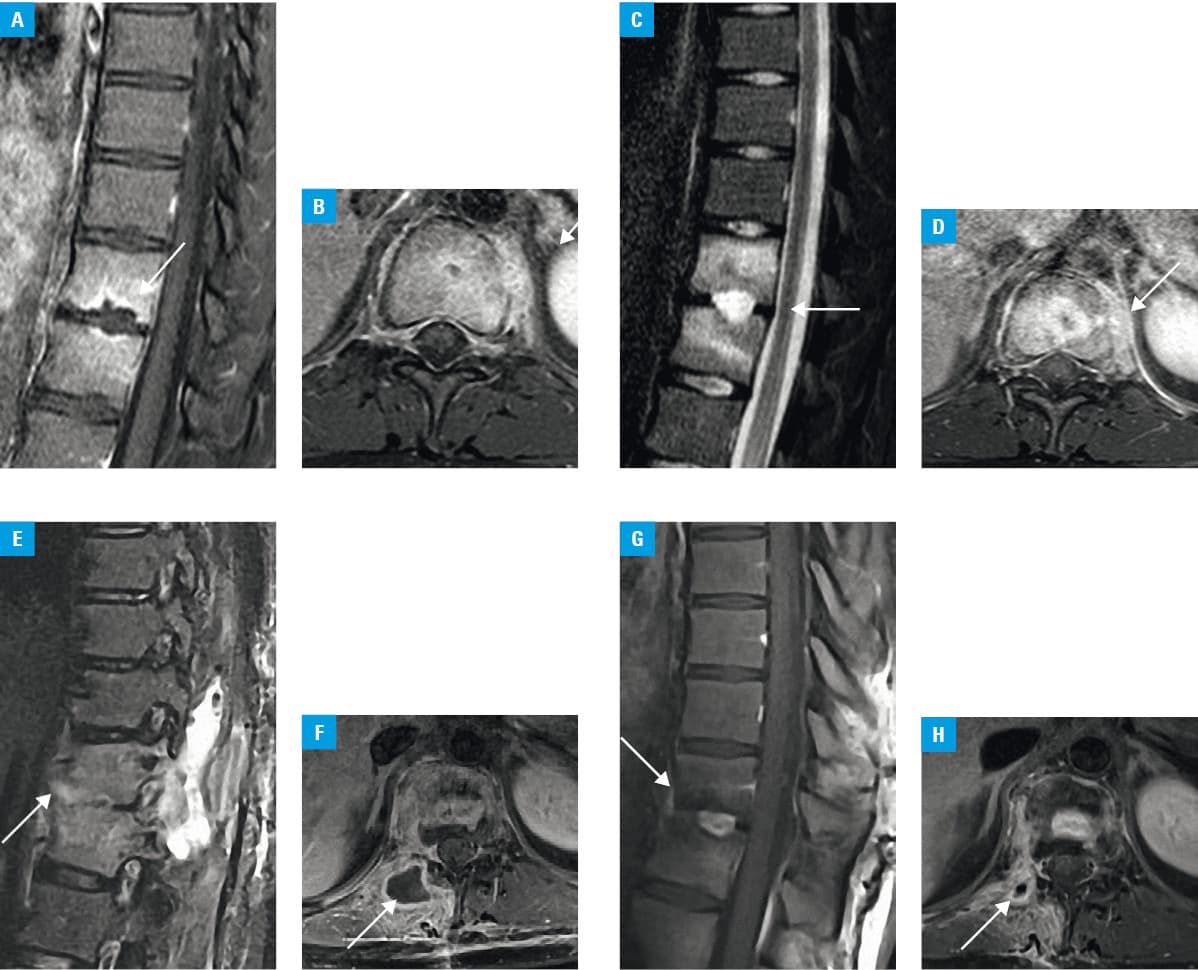
The TST and IGRA (QFT) tests were performed again, with negative results. The rapid Xpert MTB/RIF molecular assay was performed, with the use of a paraffin‑embedded block containing a specimen collected 3 months earlier during the vertebral body biopsy. The findings demonstrated the presence of genetic material of the M. tuberculosis complex. The patient was diagnosed with bone and joint tuberculosis involving Th11 and Th12 vertebrae and a suspicion of cold abscess. After 4 weeks of antituberculous treatment, readmission to the hospital was scheduled to perform a follow‑up MRI and to qualify the patient for surgical fluid collection removal from the paraspinal soft tissue (Figure 1G and 1H). A considerable regression of the inflammatory lesions was observed, suggesting proper tuberculosis diagnosis and reasonable antituberculous treatment that was prolonged to 12 months. The surgery was abandoned.
In the case described, tuberculosis was diagnosed after 8 months following the pain onset and initial assessment. The diagnosis was hampered by lesion localization as well as negative microbiological, TST, and IGRA tests. The specific infection was found owing to ineffective antibiotic therapy, progression of MRI‑detected lesions as well as histological analysis and genetic findings based on paraffin‑embedded biopsy specimen examinations. Tuberculosis was confirmed by histological examination and molecular tests using a paraffin‑embedded biopsy specimen.
- Teo HEL, Peh WCG. Skeletal tuberculosis in children. Pediatr Radiol. 2004; 34: 853‑860. | Crossref
- Broderick C, Hopkins S, Mack DJF, et al. Delays in the diagnosis and treatment of bone and joint tuberculosis in the United Kingdom. Bone Joint J. 2008; 100‑B: 119‑124. | Crossref
- Korzeniewska‑Koseła M. Tuberculosis and lung diseases in Poland in 2019. National Tuberculosis and Lung Diseases Research Institute, Warsaw; 2020.
- Korzeniewska‑Koseła M, Gątarek J, Bestry I, et al. Tuberculosis diagnosed by thoracic surgeons. Pol Arch Intern Med. 2021; 131: 615‑616. | Crossref
- Jambhekar NA, Kulkarni SP, Madur BP, et al. Application of the polymerase chain reaction on formalin‑fixed, paraffin‑embedded tissue in the recognition of tuberculous osteomyelitis. J Bone Joint Surg Br. 2006; 88: 1097‑101. | Crossref
ARTICLE INFORMATION