Serum concentrations of phenylalanine and tyrosine isomers in patients with acute coronary syndrome



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Serum concentrations of phenylalanine and tyrosine isomers in patients with acute coronary syndrome
Introduction
Oxidative stress plays a pivotal role in the pathogenesis of several cardiovascular diseases, including atherogenesis, ischemic‑reperfusion injury, and cardiac remodeling.1 Under oxidative stress conditions, excess hydroxyl radicals can oxidize the benzyl ring of phenylalanine, producing abnormal tyrosine isomers (meta-tyrosine, ortho-tyrosine, and para-tyrosine).2 The accumulation of m-tyrosine has been reported to adversely affect cells, suggesting a direct role of this isomer in oxidative stress damage.3 As a result, increase in m-tyrosine levels is commonly used as a biomarker of oxidative stress.3
Normal physiological enzymatic processes also produce p-tyrosine from phenylalanine, predominantly in the kidney due to activation of the enzyme phenylalanine‑4‑hydroxylase (PAH).2 Recent evidence suggests that oxidative stress induced by immune activation and inflammation may destroy the enzyme cofactor tetrahydrobiopterin (BH4) and impair the activity of PAH. As a result, the conversion of phenylalanine to tyrosine by PAH may be diminished.4 However, no single study has investigated tyrosine isomers in patients with acute coronary syndrome (ACS). Therefore, the present study was designed to compare these parameters in blood samples of ACS patients and healthy controls. The aim of this study was to examine the association of phenylalanine and tyrosine isomers (m-, o-, and p-tyrosine) with oxidative stress following myocardial injury.
Patients and methods
Patients
A cohort of 44 patients (11 men, 33 women) admitted to the Department of Interventional Cardiology of the Heart Institute of Pécs University Clinical Center (Pécs, Hungary) were part of this case‑control study of ACS patients. The diagnosis of ACS was defined according to the ST segment deviation: ST‑segment elevation myocardial infarction (STEMI) and non‑STEMI (NSTEMI). Patients aged 30 years and older with confirmed diagnosis of STEMI or NSTEMI were included. The exclusion criteria comprised the lack of serum samples of adequate volume or an uncertain diagnosis of ACS. None of the ACS patients had inflammatory disease or cancer that could impact the tyrosine isomer concentration.
Clinical and angiographic evaluation
General medical history was collected and physical examinations, standard laboratory tests, and 12‑lead electrocardiography were performed in all patients upon admission. The type of ACS was assigned based on the American Heart Association and American College of Cardiology guidelines.5 The extent of coronary artery disease (CAD) was ascertained by coronary angiography and was categorized according to the number of coronary arteries with obstructive CAD (defined as angiographic stenosis of ≥50%) into 0-, 1-, 2- or 3‑vessel disease.
Control group
Control serum samples were obtained by collecting blood from 26 healthy volunteers who were healthcare workers at the same Heart Institute mentioned above, with a gender distribution of 11 men and 15 women. A biobank similar to that of ACS patients was created by selecting volunteers aged 25 to 72 years. None of the volunteers had cardiovascular disease, risk factors for CAD, or used immunosuppressive drugs.
Ethics
This study was approved by the Regional and Institutional Research Ethics Committee (4511/2016) of the University of Pécs and was conducted in accordance with the ethical guidelines of the 2003 Declaration of Helsinki. All participants gave their informed consent.
Blood collection and laboratory analysis
Blood samples were drawn from the aortic root and the radial artery for ACS patients, while for the control group, they were drawn by venipuncture. Serum was obtained through centrifugation (3000 rpm, 10 min) and was stored at −80 °C until further examination. Afterwards, 125 μl of trichloroacetic acid (Reanal Private Ltd, Budapest, Hungary) was added to 500 μl of serum and the samples were incubated on ice for 30 minutes. The precipitate was subsequently separated by centrifugation. The supernatant was filtered by a syringe filter (0.2 μm; Millipore, Billerica, Massachusetts, Unites States) before analysis. Phenylalanine and tyrosine concentration measurements are described in Supplementary material, the Laboratory analysis section and Figure S1.
Statistical analysis
SPSS software, version 22.0 (IBM Corporation, Armonk, New York, United States) was used for statistical analysis. Continuous variables were expressed as mean (SD) or median and interquartile range. Categorical variables were expressed as percentages or frequencies. Normal distribution was assessed with the Shapiro–Wilk test. Comparisons between the ACS patients and healthy controls were performed using the χ2 test for categorical variables, the t test for normally distributed continuous variables, and the Mann–Whitney test for skewed continuous variables. To assess the correlation between the amino acid parameters and baseline characteristics of patients with ACS, we used Spearman rank correlation. P values of less than 0.05 were considered statistically significant.
Results
A comparison of baseline characteristics and amino acid parameters for ACS patients showed no significant differences between the STEMI and NSTEMI subgroups; therefore, ACS patients were treated as a single group. Similar results have been published previously.6 Gender distribution did not differ significantly between ACS patients and healthy controls (men / women, 11/33 vs 11/15, respectively; P = 0.13), but the mean age was higher in the ACS group (mean [SD], 68.1 [9.4] years vs 47.5 [12.7] years, respectively; P = 0.02). Demographic and clinical data of the study population are summarized in Supplementary material, Table S1.
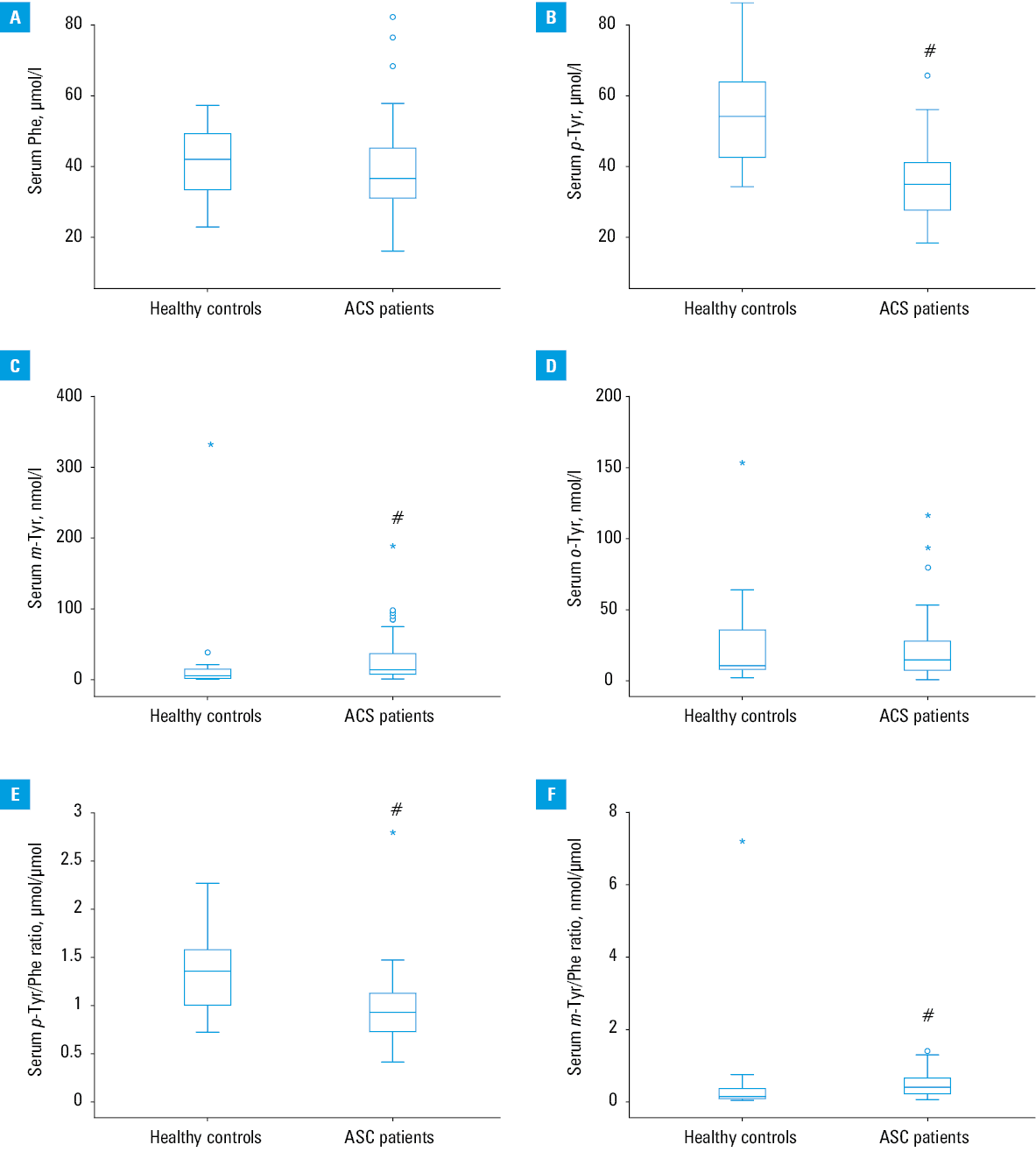
Our data showed that while serum phenylalanine concentrations did not differ between ACS patients and controls (Figure 1A), serum p-tyrosine levels were lower in the ACS group than in controls (median, 34.9 vs 54.1 μmol/l; P < 0.001) (Figure 1B). Serum m-tyrosine concentrations were higher in ACS patients than in controls (median, 14.6 vs 6.1 nmol/l; P < 0.001) (Figure 1C), whereas serum o-tyrosine concentrations did not differ between the two groups (Figure 1D). Moreover, the serum p-tyrosine / phenylalanine ratio was lower in ACS patients compared with controls (median, 0.9 vs 1.4 μmol/μmol; P <0.001) (Figure 1E). In contrast, the serum m-tyrosine / phenylalanine ratio was higher in ACS patients compared with controls (median, 0.3 vs 0.1 nmol/μmol; P <0.001) (Figure 1F).
When comparing serum p-tyrosine / phenylalanine ratios from our recalculated data on different illnesses, we found that this ratio was significantly lower in all patients compared with controls (Supplementary material, Figure S2).
In both ACS patients and controls, no gender differences were found for phenylalanine or p-, m-, or o-tyrosine. None of these amino acid parameters were correlated for age in either group. Moreover, creatinine levels and estimated glomerular filtration rates were not significantly correlated with either phenylalanine or p-, m-, or o-tyrosine in ACS patients. Serum m-tyrosine levels did show a positive correlation with p-tyrosine / phenylalanine ratios in different vessel segments (Supplementary material, Figure S3).
Discussion
In the present study, we found that the serum p-tyrosine concentration and the p-tyrosine / phenylalanine ratio were both lower in ACS patients compared with controls. Similar results were described in patients with diseases associated with inflammation and immune activation, such as sepsis, diabetes, and renal failure as well as in burn patients.7-10
The current data are in line with the results obtained from our previous studies that we recalculated (the data presented in Supplementary material, Figure S2 are based partly on literature data).4,7,8,10 These results further support the idea that diminished conversion of phenylalanine to tyrosine by PAH may be due to increased production of reactive oxygen species, which can cause a decrease in the enzyme cofactor BH4 that takes part in the enzymatic reaction.4,7-9 Therefore, the observed decrease in the serum p-tyrosine concentration and the p-tyrosine / phenylalanine ratio could be attributed to reduced enzymatic production of cofactor BH4.
Another important finding was that the serum m-tyrosine concentration and the m-tyrosine / phenylalanine ratio were both higher in ACS patients compared with controls. Similar results were detected in patients with diseases in which oxidative stress is thought to play a pivotal pathological role, such as sepsis, lens cataracts, as well as in burn patients and those after trauma and acute ischemic stroke.2,8,11,12 These results indicate that increased serum concentration of m-tyrosine and the m-tyrosine / phenylalanine ratio in ACS patients may reflect oxidative stress induced by inflammation.2,7,11,12
Conclusions
The results of this study showed that increased serum m-tyrosine levels can reflect oxidative stress induced by inflammation after myocardial injury, similarly to the observed decrease in p-tyrosine levels.
- Vichova T, Motovska Z. Oxidative stress: predictive marker for coronary artery disease. Exp Clin Cardiol. 2013; 18: e88‑e91.
- Ipson BR, Fisher AL. Roles of the tyrosine isomers meta-tyrosine and ortho-tyrosine in oxidative stress. Ageing Res Rev. 2016; 27: 93‑107. | Crossref
- Ipson BR, Green R, Wilson JS, et al. Tyrosine aminotransferase is involved in the oxidative stress response by metabolizing meta-tyrosine in Caenorhabditis elegans. J Biol Chem. 2019; 294: 9536‑9554. | Crossref
- Murr C, Grammer TB, Meinitzer A, et al. Immune activation and inflammation in patients with cardiovascular disease are associated with higher phenylalanine to tyrosine ratios: the ludwigshafen risk and cardiovascular health study. J Amino Acids. 2014; 2014: 783730. | Crossref
- Amsterdam EA, Wenger NK, Brindis RG, et al. 2014 AHA/ACC Guideline for the management of patients with non‑ST‑elevation acute coronary syndromes. J Am Coll Cardiol. 2014; 64: e139‑e228. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION