Performance of plastic stents used for benign and malignant biliary strictures: experience of a single high‑volume endoscopy unit
Key words: biliary stenting, complications, endoscopic retrograde cholangiopancreato- graphy, plastic stent



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Performance of plastic stents used for benign and malignant biliary strictures: experience of a single high‑volume endoscopy unit
Introduction: Endoscopic plastic biliary stenting has been used for more than 30 years as a temporary or definitive treatment of benign and malignant neoplasms. These stents are commonly available, inexpensive, and easy to implant.
Objectives: We aimed to evaluate the duration of plastic stent patency, to assess complications associated with stent use, and to determine the optimal timing of stent replacement depending on the indication for biliary stenting.
Patients and methods: This was a retrospective cohort study with a 5‑year follow‑up including patients who underwent plastic biliary stent implantation between 2012 and 2013 in a tertiary referral gastroenterological center. The performance of stents was assessed on the basis of medical records, direct contact with patients or their family members, and information derived from the national death registry.
Results: We assessed 830 biliary stenting procedures performed in 346 patients. The indications for biliary stenting included choledocholithiasis in 120 patients (34.7%), benign stricture in 70 patients (20.2%), and malignant stricture in 156 patients (45.1%). The mean duration of stent patency for these conditions was 110, 106, and 55 days, respectively (P <0.001). Stents implanted for malignant perihilar strictures had a shorter duration of patency than those used for distal strictures (40 days vs 76 days, P = 0.002).
Conclusions: The patency of plastic stents depends on the underlying disease. In patients with benign biliary disease, stent replacement is recommended after about 3.5 months. In patients with cancer, the timing of stent replacement should be guided by survival prognosis and location of stricture.
What's new?
Endoscopic biliary stenting has been used for over 30 years as a definitive or temporary treatment of benign and malignant conditions. Plastic stents are still commonly applied today despite technological advances and the development of self‑expandable metal stents. Data on the optimal timing of stent replacement are equivocal. In this study on a large population of patients, we showed that stents should be replaced after about 3.5 months in the case of benign biliary disease. In patients with malignancy, the timing of stent replacement should depend on the location of the biliary stricture and survival prognosis, because systemic infection resulting from stent dysfunction may be life threatening. Our findings have important implications for future clinical decision making, because, so far, all patients with neoplastic biliary disease were treated as a uniform population.
Introduction
The implementation of biliary stenting during endoscopic retrograde cholangiopancreatography (ERCP) has been a significant advancement in the treatment of biliary strictures. Endoscopic stenting is performed both in benign1 and malignant biliary diseases. Stenting has effectively replaced palliative surgery in patients with cancer, improving their quality of life and prolonging life expectancy.2,3 Plastic biliary stents were introduced into clinical practice in the 1980s. Despite their gradual replacement by self‑expandable metal stents (SEMS), they are still used today, mostly because of significantly lower costs and the ease of implantation. Currently available biliary stents show large differences in shape (straight, double pigtail, or single pigtail), diameter (5–12 French [F]; 1 F = 0.33 mm), length (5–18 cm), and wall composition (polytetrafluoroethylene, polyethylene, or polyurethane).4,5
The lifespan of stents is limited as they become occluded by biliary sludge, biofilm formation, or tumor growth.6 Numerous factors influence the duration of stent patency, including the inner diameter of the stent7 or the location of biliary stricture. Moreover, endoscopic stenting carries certain risks related either to the implantation and presence of stents in the biliary ducts or to ERCP alone. The stenting of distal biliary strictures is associated with higher technical and clinical success rates than stenting of hilar biliary strictures.8 Despite various methods employed to prevent stent occlusion, such as stent impregnation with antimicrobial agents, coating with silver, or the use of special polymers, a significant increase in the duration of stent patency has not been achieved so far.9,10
The main objective of our study was to evaluate the performance of plastic stents in patients with benign and malignant biliary strictures to determine suggested time intervals for stent replacement to avoid the development of acute cholangitis that may quickly progress to sepsis, especially in patients on immunosuppressive treatment, with multimorbidity, and at advanced age.
Patients and methods
We retrospectively assessed 830 consecutive biliary stenting procedures with plastic stents performed in 346 patients hospitalized in the Department of Gastroenterology and Hepatology of the Medical University of Silesia in Katowice, Poland, between January 1, 2012 and December 31, 2013. The follow‑up lasted 5 years. Data on indications for stenting, laboratory results, short‑term outcomes, and complications were obtained from medical records, while information on long‑term outcomes was collected via direct phone calls to patients or their authorized representatives and, if necessary, from the national death registry.
Endoscopic biliary stenting during ERCP was performed by 5 experienced endoscopists (more than 2000 procedures each). Patients received 100 mg of diclofenac rectally and an adequate fluid supply prior to ERCP, unless contraindicated. They were divided into 3 groups depending on the diagnosis: choledocholithiasis (n = 120), benign biliary stricture (n = 70), and malignant biliary stricture (n = 156). Malignancy was diagnosed on the basis of histopathologic results (material collected during ERCP, endoscopic ultrasound, or percutaneous biopsy). The study also included 12 patients in whom imaging tests and the course of the disease clearly supported the diagnosis. Stenting efficacy was evaluated on the basis of the clinical picture and laboratory parameters. The lack of efficacy was defined as persisting cholangitis and / or no decline in bilirubin or alkaline phosphatase levels. The duration of stent patency was defined as the time from stent insertion to the first symptoms of stent dysfunction as specified below. In patients who died without apparent signs of stent dysfunction (as determined on the basis of hospitalization records or information provided by family members), the duration of stent patency was defined as the time from stent insertion to the date of death.
As there are no standardized criteria for diagnosing stent dysfunction, the diagnosis was based on the criteria proposed by Schmidt et al,11 including biliary dilatation on ultrasound (as compared with the bile duct size after stenting); bilirubin concentration of at least 2 mg/dl or higher with an increase of 1 mg/dl or higher as compared with the concentration after successful stenting; at least a double increase above the upper limit of normal or an increase by at least 30 IU/l in alkaline phosphatase or γ-glutamyl transferase levels; and signs of cholangitis (fever or leukocyte count >10 000/mm3 or C‑reactive protein >20 mg/dl).
Distal migration of straight stents was recognized if the lower end of the stent rested on the opposite wall of the duodenum or if its upper end was located below the stricture or stone. A pigtail stent was considered distally dislocated when its upper end was found in the main biliary duct or below the stricture level or stone. Proximal migration of both straight and pigtail stents was diagnosed in the case of an invisible protrusion of the stent from the ampulla of Vater with the presence of stent in the biliary tree on fluoroscopy. Complete migration was defined as the absence of a stent in the bile ducts on fluoroscopy.
Malignant strictures were divided into those located in the proximal biliary ducts (hilar cholangiocarcinoma and gallbladder cancer) and distal biliary ducts (ampullary carcinoma, pancreatic cancer, and distal cholangiocarcinoma). As biliary strictures caused by metastases often involve several portions of the intrahepatic biliary tree, they were not included in this division.
Short biliary strictures, the strictures of moderate length, and long strictures were defined as the narrowing of the biliary duct over a distance of less than or equal to 10 mm, 11–30 mm, and more than 30 mm, respectively. Patients included in the study did not use ursodeoxycholic acid or antibiotics to exclude their effect on bile lithogenicity owing to divergent results reported in the literature.10 Patients were treated with antibiotics before ERCP in accordance with the European Society of Gastrointestinal Endoscopy (ESGE) recommendations (eg, in the case of immunocompromised patients or if incomplete biliary drainage was expected).8
Ethical approval
The need for ethical approval was waived by the Ethics Committee of the Medical University of Silesia (decision no., KNW/0022/KB/326/18/19). The study was conducted in accordance with the Declaration of Helsinki. The patient’s consent was not required.
Statistical analysis
Data were presented as median with interquartile range (IQR) or the number (percentage) of procedures / patients. The Mann–Whitney test was used for a comparison of quantitative variables between 2 groups, while the Kruskal–Wallis test was applied for a comparison of more than 2 groups. The χ2 test was used for comparison of qualitative variables. A P value of less than 0.05 was considered significant. Statistical calculations were made using Statistica 12.0 (StatSoft, Kraków, Poland).
Results
Demographic data of patients and indications for stenting are listed in Table 1. Duration of stent patency depending on stent type and diameter, indications for stenting, the length of stricture, and the number of stones are shown in Table 2. Stents used for perihilar strictures (n = 126) remained patent for a median (IQR) of 40 (20–89) days, while those inserted for distal strictures (n = 89), for a median (IQR) of 76 (34–129) days (P = 0.002).
Parameter | Value | |
Abbreviations: ERCP, endoscopic retrograde cholangiopancreatography; F, French; IQR, interquartile range | ||
General data | ||
Number of patients | 346 | |
Age, y, median (IQR) | 67.3 (58.3–75.9) | |
Sex, n (%) | Female | 167 (48) |
Male | 179 (52) | |
Number of ERCPs | 830 | |
Indication for biliary stenting, n (%) | ||
Choledocholithiasis | Patients | 120 (34.7) |
Procedures | 210 (25.3) | |
Benign strictures | Patients | 70 (20.2) |
Procedures | 255 (30.7) | |
Malignant strictures | Patients | 156 (45.1) |
Procedures | 365 (44) | |
Procedural data | ||
Number of ERCPs per patient, n (%) | 1 | 303 (36.5) |
2 | 187 (22.5) | |
3 and 4 | 179 (21.6) | |
≥5 | 161 (19.4) | |
Number of implanted stents, n (%) | 1 | 720 (86.7) |
2 | 110 (13.3) | |
Type of stent, n (%) | Double pigtail | 346 (41.7) |
Straight | 451 (54.3) | |
Both types | 33 (4) | |
Type and diameter of stent, n (%) | One 7F double pigtail stent | 303 (36.5) |
Two 7F double pigtail stents | 38 (4.6) | |
One 8.5F–10F straight stent | 417 (50.2) | |
Other combination | 72 (8.7) | |
Clinical outcome, n (%) | Primary loss of function | 49 (5.9) |
Secondary loss of function | 430 (51.8) | |
Sustained function | 323 (38.9) | |
Unknown | 28 (3.4) | |
Variable | n/N | Duration of stent patency, d, median (IQR) | P value |
Abbreviations: n, number of procedures; N, total number of procedures; others, see Table 1 | |||
Indication for stenting | |||
Choledocholithiasis | 78/430 | 110 (42–218) | <0.001 |
Benign stricture | 125/430 | 106 (54–252) | |
Malignant stricture | 227/430 | 55 (26–108) | |
Type of stent | |||
Double pigtail | 159/430 | 71 (38–150) | 0.1 |
Straight | 253/430 | 79 (30–156) | |
Both types | 18/430 | 79.5 (39–147) | |
Stent diameter | |||
7F | 134/430 | 85 (38–162) | 0.18 |
Double 7F | 25/430 | 48 (33–69) | |
8.5–10F | 232/430 | 81 (30–156) | |
≥15F | 39/430 | 76 (39–171) | |
Number of ERCPs | |||
1 | 127/430 | 89 (26–155) | 0.92 |
2 | 96/430 | 82.5 (31.5–170.5) | |
3–4 | 101/430 | 69 (38–157) | |
≥5 | 106/430 | 72.5 (39–138) | |
Type of malignancy | |||
Ampullary cancer | 36/227 | 79 (23.5–109) | <0.001 |
Pancreatic cancer | 53/227 | 76 (36–132) | |
Gallbladder cancer | 19/227 | 35 (20–82) | |
Cholangiocarcinoma | 107/227 | 47 (23–91) | |
Liver metastases | 12/227 | 172 (75.5–303) | |
Site of malignant biliary stricture | |||
Distal | 89/215 | 76 (34–129) | 0.002 |
Proximal | 126/215 | 40 (23–89) | |
Length of stricture | |||
≤10 mm | 56/341 | 122.5 (68–283) | <0.001 |
11–30 mm | 185/341 | 67 (31–137) | |
>30 mm | 80/341 | 57.5 (28–105) | |
Number of stones in the common bile duct | |||
1 | 35/125 | 101 (52–184) | 0.65 |
2 | 13/125 | 121 (59–260) | |
≥3 | 77/125 | 108 (40–217) | |
A relationship between time (months) and the proportion of patients with stent patency depending on the underlying disease is shown in Figure 1. The frequency of stent migration depending on tumor site, the number and length of inserted stents, and the location of the stent’s proximal end are presented in Table 3.
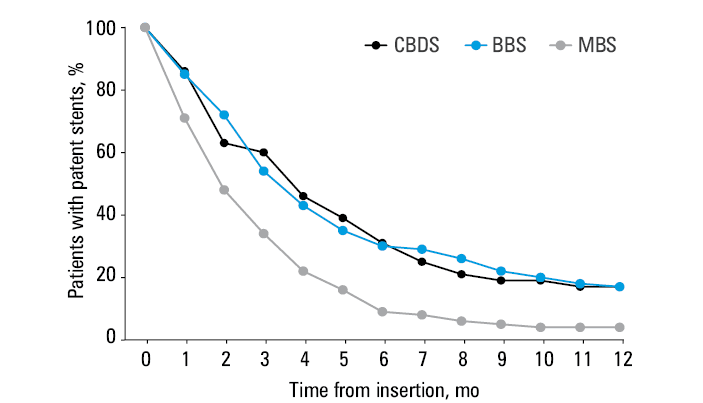
Abbreviations: BBS, benign biliary stricture; CBDS, common bile duct stones; MBS, malignant biliary stricture
Stent migration | Total number of procedures | Procedures with stent migration, n (%) | χ2 value | P value | |||
a Double pigtail only
b Straight only | |||||||
Indication for stenting | |||||||
Choledocholithiasis | 210 | 32 (15.2) | 17.88 | 0.001 | |||
Benign stricture | 255 | 22 (8.6) | |||||
Malignant stricture | 365 | 18 (4.9) | |||||
Site of malignant biliary stricture | |||||||
Distal | 158 | 6 (3.7) | 1.42 | 0.23 | |||
Proximal | 185 | 12 (6.5) | |||||
Type of stent | |||||||
Double pigtail | 346 | 43 (12.4) | 10.98 | 0.04 | |||
Straight | 451 | 26 (5.8) | |||||
Both types | 33 | 3 (9.1) | |||||
Number and length of stents | |||||||
Single | 720 | 66 (9.2) | 1.66 | 0.2 | |||
Multiple | 110 | 6 (5.5) | |||||
Straight ≤7 cm | 85 | 8 (9.4) | 2.95 | 0.09 | |||
Straight >7 cm | 326 | 15 (4.6) | |||||
Double pigtail ≤9 cm | 138 | 24 (17.4) | 2.72 | 0.1 | |||
Double pigtail >9 cm | 158 | 17 (10.8) | |||||
Location of the proximal end of the stent | |||||||
Double pigtail | Right hepatic duct | 123 | 13 (10.6) | 3.88 | 0.14 | ||
Left hepatic duct | 198 | 29 (14.6) | |||||
Bilateral | 32 | 1 (3.1) | |||||
Straight | Main bile duct | 257 | 11 (4.3) | 3.65 | 0.3 | ||
Right hepatic duct | 165 | 10 (6.1) | |||||
Left hepatic duct | 47 | 5 (10.6) | |||||
Bilateral | 9 | 1 (11.1) | |||||
Spontaneous stent discharge in relation to its type / length and clinical indication for stenting | |||||||
Double pigtail | 346 | 37 (10.7) | 33.63 | <0.001 | |||
Straight | 451 | 6 (1.3) | |||||
Choledocholithiasisa | 166 | 24 (14.5) | 4.73 | 0.03 | |||
Benign and malignant stricturesa | 180 | 13 (7.2) | |||||
Choledocholithiasisb | 44 | 0 | 0.66 | 0.42 | |||
Benign and malignant stricturesb | 407 | 6 (1.5) | |||||
Straight ≤7 cm | 85 | 3 (3.5) | 3.19 | 0.07 | |||
Straight >7 cm | 326 | 1 (0.3) | |||||
Double pigtail ≤9 cm | 138 | 21 (15.2) | 2.85 | 0.09 | |||
Double pigtail >9 cm | 158 | 14 (8.9) | |||||
Complications associated with stenting are listed in Tables 4 and 5. Of the 72 episodes of stent migration, proximal migration occurred in 9 cases only when using the straight stent. Two patients were referred for surgery because the stents could not be removed by endoscopy (straight stents with a diameter of 10F and a length of 12 cm or 9 cm). Distal migration was observed for 45 double pigtail stents and for 18 straight stents. We noted 5 cases of bowel perforation, all of which were caused by straight stents with a diameter of 10F and a length of 9 cm or 12 cm. Two cases of bile duct perforation occurred with a double pigtail stent (diameter of 7F and length of 9 cm). Stent fracture was noted in 4 cases, including 2 with double pigtail stents (diameter of 7F and length of 12 cm or 15 cm) and 2 with straight stents (each with a diameter of 10F and a length of 9 cm).
Complication | Proceduresa, n (%) |
a Total number of procedures, N = 830
b Nonremovable stents were broken at the same time. | |
Overall | 77 (9.3) |
Stent migration | 72 (8.7) |
Stent fracture | 4 (0.5) |
Nonremovable stentb | 2 (0.2) |
Proximal insertion | 1 (0.1) |
Complication | Proceduresa, n (%) |
a Total number of procedures, N = 830
Abbreviations: PEP, postendoscopic retrograde cholangiopancreatography pancreatitis | |
Overall | 43 (5.1) |
PEP | 12 (1.4) |
Bleeding | 4 (0.5) |
Liver or pancreatic abscesses | 15 (1.8) |
Cholecystitis | 5 (0.6) |
Duodenal perforation | 5 (0.6) |
Biliary perforation | 2 (0.24) |
Discussion
In 2018, the ESGE released updated guidelines regarding indications for biliary stenting and stent selection.8,12 For malignant lesions, SEMS were recommended owing to their longer duration of patency, smaller number of required reinterventions, and longer patient survival.13-15 However, plastic stents are still used in clinical practice in patients with short life expectancy (<6 months), no histopathological confirmation of the disease, or contraindications to the use of fully covered SEMS (eg, hilar stricture, scheduled endoscopic ultrasound–guided biopsy, or incidence of cholecystitis after using fully covered SEMS).
Our study indicates that the timing of stent replacement should be strictly guided by an indication for stenting and the type of suspected or diagnosed cancer. In perihilar tumors, an endoscopic reintervention can be scheduled after approximately 35 days for gallbladder cancer and 47 days for cholangiocarcinoma. For tumors located in the distal part of the biliary tract (pancreatic cancer, ampullary carcinoma, distal cholangiocarcinoma), this period should be almost twice as long.
In benign strictures (postinflammatory, iatrogenic, secondary to liver transplant or chronic pancreatitis), the ESGE recommends using as many plastic stents or fully covered SEMS as possible. In patients with plastic stents, replacement is recommended every 3 to 4 months for about 1 year.8 In our study, the duration of plastic stent patency was significantly longer in benign compared with malignant strictures, which can be explained by cancer progression associated with the increasing narrowing and the size of stricture or alterations in bile consistency. The duration of stent patency in our study correlated with the length of stricture.
Short‑term stenting is recommended if biliary stones cannot be removed at first attempt.16 Di Giorgio et al17 suggested stent replacement after approximately 3 months in these cases, which is in line with our results (mean patency duration, 110 days). Nevertheless, we did not find a relationship between the diameter or number of stones and stent patency duration. With temporary stenting, not only can the normal bile outflow be preserved, but also the size of stones may be decreased by about 50% within 2 to 6 months.18
Several small studies suggested that stents with a diameter of less than 10F are characterized by a shorter duration of patency compared with larger stents, although the duration was not significantly improved with stents over 10F.5 In our study, no clear relationship was found between stent diameter and patency duration.
The stent migration rate of 8.7% found in our study is in line with literature data.19 Stent migration was less common in patients with malignancy than in those with benign lesions. A similar relationship was also reported by other authors.20 This finding can probably be explained by the fact that malignant strictures are longer and firmer than benign ones, thus better stabilizing the stent. Both partial and complete migrations were significantly more common with double pigtail stents, which may be related both to the small inner diameter and the curved lower end of the stent being more susceptible to peristaltic waves of the duodenum compared with straight stents. We also noted a tendency for an easier migration of shorter stents (both straight and double pigtail), but the difference was not significant. Moreover, the location of the proximal end in the biliary tree and the number of stents had no significant effect on the stent migration rate.
Endoscopic retrograde cholangiopancreatography is associated with a high rate of complications, the most common being acute pancreatitis, cholangitis, cholecystitis, bleeding, and duodenal perforation.20 In our study, the rate of post‑ERCP acute pancreatitis was 1.4%, which is lower than in other publications (3.5%–9.7%).21 Importantly, in accordance with the ESGE guidelines, our patients were routinely administered intravenous hydration and rectal diclofenac (100 mg) during the procedure.20,22 In addition, post‑ERCP acute pancreatitis is more frequent in patients younger than 55 years, while our patients were generally much older and most stenting procedures were reinterventions after previous sphincterotomy. Furthermore, the procedures were performed by experienced endoscopists who avoided unnecessary cannulations of the papilla of Vater and the pancreatic duct, thus reducing the risk of acute pancreatitis.23-26 We also assessed ERCP‑associated bleeding requiring an endoscopic intervention with transfusion of packed red blood cells. The bleeding rate in our study was 0.5%, which is closer to the lower margin of the range reported by other centers (0.3%–9.6%).20 The prevalence of other complications was also similar to that described in the available literature. In a large meta‑analysis, Cirocchi et al27 reported that perforation during ERCP occurred in 0.6% of cases,27 while cholecystitis was observed in 0.5% to 5.4% of cases.28 Duodenal perforation occurs mostly with straight stents,29 which is in line with our findings.
Our study shows the clinical advantages of biliary stenting with plastic stents based on the assessment of a large cohort in the real‑life setting. However, the study is not without limitations. First, it was a retrospective analysis presenting the experience of a single gastroenterological unit. Second, the number of patients with a simultaneous insertion of numerous biliary stents was small. Finally, we did not assess anthropometric parameters, comorbidities, or physical activity of the included patients, while these factors have a potential impact on reducing biliary cholesterol saturation and facilitating biliary tract peristalsis.
In summary, in patients with benign biliary strictures, stent replacement should be recommended at an interval of about 3.5 months to avoid cholangitis caused by stent dysfunction. Stent patency duration is affected by the length and location of the stricture. Therefore, in patients with malignant biliary strictures with short life expectancy, the timing of stent replacement should be guided by the site of biliary stricture and life expectancy. There was no significant relationship between the diameter, type, and number of inserted stents and the duration of their patency. The rate of stent migration depends on the characteristics of stricture and the type of stent. Our findings have important implications for clinical practice and decision making on stent replacement in patients with benign versus those with malignant biliary strictures.
- Costamagna G, Tringali A, Perri V, et al. Endotherapy of postcholecystectomy biliary strictures with multiple plastic stents: long‑term results in a large cohort of patients. Gastrointest Endosc. 2020; 91: 81‑89. | Crossref
- Artifon EL, Sakai P, Cunha JE, et al. Surgery or endoscopy for palliation of biliary obstruction due to metastatic pancreatic cancer. Am J Gastroenterol. 2006; 101: 2031‑2037. | Crossref
- Ballinger AB, McHugh M, Catnach SM, Lark ML. Symptom relief and quality of life after stenting for malignant bile duct obstruction. Gut. 1994; 35: 467‑470. | Crossref
- Ferreira LE, Baron TH. Endoscopic stenting for palliation of malignant biliary obstruction. Expert Rev Med Devices. 2010; 7: 681‑691. | Crossref
- Mangiavillano B, Pagano N, Baron TH, et al. Biliary and pancreatic stenting: devices and insertion techniques in therapeutic endoscopic retrograde cholangiopancreatography and endoscopic ultrasonography. World J Gastrointest Endosc. 2016; 8: 143‑156. | Crossref
ARTICLE INFORMATION