CAd26.COV2‑S vaccination can reveal inherited thrombophilia: a case of massive cerebral venous sinus thrombosis in a young man with normal platelet count



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
CAd26.COV2‑S vaccination can reveal inherited thrombophilia: a case of massive cerebral venous sinus thrombosis in a young man with normal platelet count
Cerebral venous sinus thrombosis (CVST) is a cerebrovascular disorder that generally occurs in younger patients (<50 years old) and is responsible for 0.5% to 1% of all strokes.1
A previously healthy, nonsmoking, 25‑year‑old White man with no personal or family history of thrombosis received an Ad26.COV2‑S COVID‑19 vaccine (Janssen / Johnson & Johnson). A few hours post vaccination the patient developed a fever and started to vomit. The next day he reported a headache of increasing severity, and 7 days after vaccination he was admitted to the hospital.
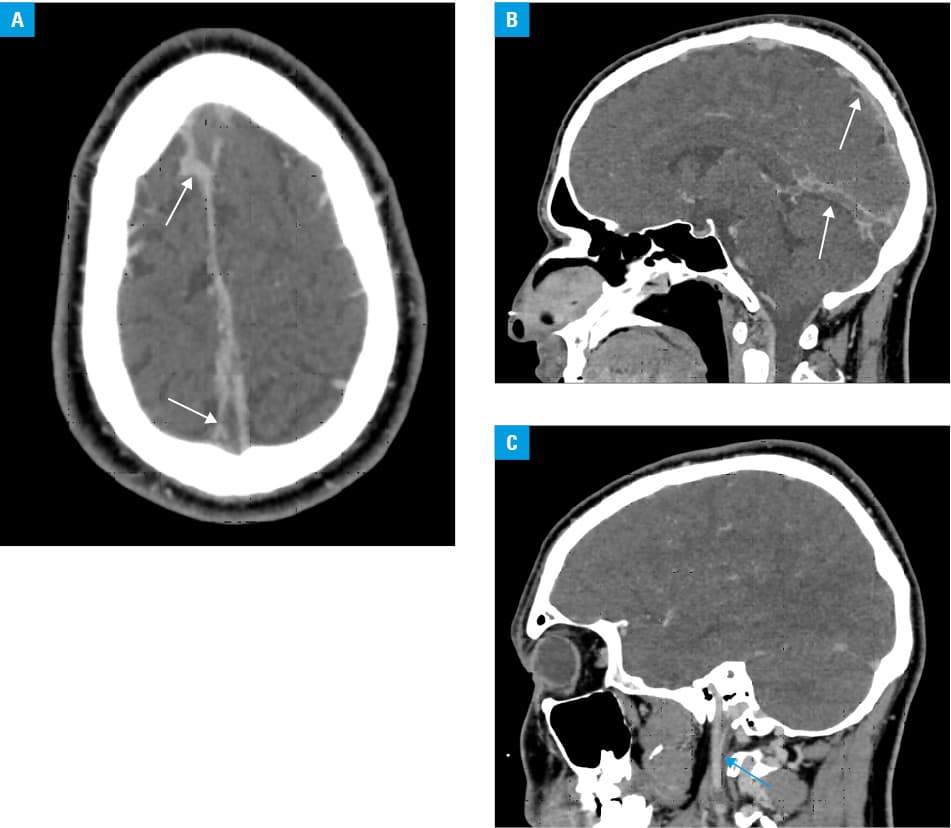
On examination he was apyrexial and overweight, with a body mass index of 27.17 kg/m2. No abnormalities were identified in the neurological examination. Laboratory blood tests showed increased levels of C‑reactive protein (83.7 mg/l; reference range <5 mg/l) and D‑dimer (3049.25 ng/ml; reference range <550 ng/ml); white blood cell and platelet counts were within the reference range (7.3 G/l and 227 G/l, respectively). The reverse transctiptase–polymerase chain reaction test for SARS‑CoV‑2 was negative. Computed tomography angiography of the head showed extensive intracranial thrombotic lesions (Figure 1A–1C). The patient was heterogeneous for factor V Leiden mutation. A heparin‑platelet factor 4 (PF4) enzyme‑linked immunosorbent assay specific for immunoglobulin (Ig) G antibodies was negative. An assay for protein C showed a level of 148% and the level of coagulation factor VIII was 208%. Moreover, the free protein S level was 83%, no mutation of prothrombin 20210A was found, and the level of antithrombin was 102.9%. Negative results were obtained for the determination of antibodies to beta‑2 glycoprotein as well as IgG and IgM anticardiolipin antibodies. The tests did not show the presence of the lupus anticoagulant. In addition, analysis of the cerebrospinal fluid revealed an elevated cell count (83/3 per ml), 87% of which were mononuclear, and the protein concentration was 0.83 g/l. No virus was detected in the cerebrospinal fluid. A sterile bacteriological culture was obtained and aseptic meningitis was finally diagnosed. Ceftriaxone at a dose of 2 g daily and enoxaparin at a dose of 80 mg twice daily were administered and the patient continued enoxaparin after discharge. In addition to the heterozygous factor V Leiden mutation, the patient had risk factors for CSVT which included an increased level of factor VIII, aseptic meningitis, and possible dehydration due to vomiting.
See et al2 reported 12 cases of CVST after Ad26.COV2.S vaccination. All patients were White women; of these, 7 had at least a single CVST risk factor. Time from Ad26.COV2.S vaccination to symptom onset ranged from 6 to 15 days. All 11 patients tested for the antibodies against PF4 had positive results.2 In contrast to the previously reported cases, our patient had not been diagnosed with thrombocytopenia. Hypotheses on the mechanisms underlying thrombotic thrombocytopenia after COVID‑19 vaccination include the role of antibodies against PF4, direct interaction between the adenoviral vector and platelets, cross‑reactivity of antibodies against the SARS‑CoV‑2 spike protein with PF4, cross‑reactivity of antiadenovirus antibodies and PF4, interactions between the spike protein and platelets, platelet expression of the spike protein and the subsequent immune response, and platelet expression of other adenoviral proteins and associated responses.3 Vaccination for COVID‑19, especially using adenovirus‑based vaccines, may predispose to various thrombotic manifestations in young individuals with previously unknown inherited thrombophilia and such patients should be screened for thrombophilia.4
- Saposnik G, Barinagarrementeria F, Brown RD Jr, et al. Diagnosis and management of cerebral venous thrombosis: a statement for healthcare professionals from the American Heart Association / American Stroke Association. Stroke. 2011; 42: 1158‑1192. | Crossref
- See I, Su JR, Lale A, et al. US case reports of cerebral venous sinus thrombosis with thrombocytopenia after Ad26.COV2.S vaccination, March 2 to April 21, 2021. JAMA. 2021; 325: 2448‑2456. | Crossref
- Rzymski P, Perek B, Flisiak R. Thrombotic thrombocytopenia after COVID‑19 vaccination: in search of the underlying mechanism. Vaccines. 2021; 9: 559. | Crossref
- Szarowska A, Zaczyński A, Szymański P, et al. Initiation of the COVID‑19 vaccination program in Poland: vaccination of the patient “zero” and first experience from the Central Clinical Hospital of the Ministry of Internal Affairs and Administration. Pol Arch Intern Med. 2021; 131: 101‑102. | Crossref
ARTICLE INFORMATION