Preliminary observations on ANGPT1 and ANGPT2 polymorphisms in systemic sclerosis: ANGPT2 rs2442598 and rs3739390 are associated with disease susceptibility and diffuse disease subtype
Key words: ANGPT2, polymorphism, rs2442598, susceptibility, systemic sclerosis



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Preliminary observations on ANGPT1 and ANGPT2 polymorphisms in systemic sclerosis: ANGPT2 rs2442598 and rs3739390 are associated with disease susceptibility and diffuse disease subtype
Introduction: Angiopoietin‑1 (Ang‑1) and -2 (Ang‑2) concentrations were found to be associated with systemic sclerosis (SSc).
Objectives: We explored whether single nucleotide polymorphisms of Ang‑1 (ANGPT1) and Ang‑2 (ANGPT2) genes can predict SSc susceptibility in Polish Caucasian patients.
Patients and methods: Genotyping by reverse transcriptase–polymerase chain reaction and Sanger sequencing was performed in 48 patients with SSc and 38 controls.
Results: Individuals with the CC genotype of ANGPT2 rs2442598 were 3.29‑fold more likely to develop SSc (odds ratio [OR], 3.288; 95% CI, 1.212–8.915; P = 0.02) compared with those carrying the CT variant. Subgroup analysis revealed that the G allele, CG, and CG+GG genotypes of ANGPT2 rs3739390 were associated with a 9‑fold higher risk to develop a diffuse form of the disease compared with the C allele or CC genotype (OR, 9.00; 95% CI, 2.102–38.519; P = 0.002 and OR, 9.00; 95% CI, 1.112–72.824; P = 0.03, respectively) and patients carrying the CG variant presented with higher serum Ang‑2 levels than those carrying the CC variant (P = 0.001). On the contrary, the likelihood of a diffuse disease subtype was 8.77‑fold lower for the TT+AT than for the AA genotype of ANGPT1 rs2507800 (OR, 0.114; 95% CI, 0.014–0.932; P= 0.04). The C allele of ANGPT2 rs3739390 was associated with a 4.83‑fold lower risk of digital ulcers (OR, 4.833; 95% CI, 1.089–21.437; P= 0.03).
Conclusions: We concluded for the first time in the literature that the ANGPT2 rs2442598 polymorphism might represent a susceptibility locus for SSc, whereas the ANGPT2 rs3739390 and ANGPT1 rs2507800 variants may affect the disease profile.
What's new?
This study documents for the first time that: 1) the ANGPT2 rs2442598 polymorphism has a potentially strong association with a higher risk of systemic sclerosis (SSc) in a population of Caucasian ancestry, and the CC variant may be a candidate genetic marker of SSc susceptibility; 2) ANGPT2 rs3739390 genetic variants affect serum levels angiopoietin‑2 and are associated with certain clinical variables, including diffuse disease subtype (dcSSc) and risk of digital ulcers; 3) ANGPT1 rs2507800 single nucleotide polymorphisms may significantly decrease the likelihood to develop dcSSc. Hence, ANGPT2 and ANGPT1 may be considered as either disease‑susceptibility or disease‑modifying gene variants in SSc with a possible, but yet unclear, pathogenic role. This preliminary study could provide reference information to drive subsequent studies on a larger cohort to elucidate the genetic function of ANGPT1 / ANGPT2 polymorphisms in SSc; in particular, their potential role in early screening to predict the risk and course of the disease.
Introduction
Systemic sclerosis (SSc) is a rare multiorgan rheumatic disease with a prevalence in Europe and the North America varying between 7.2–33.9 and 13.5–44.3 per 100 000.1 The current most accepted hypothesis points to the central role of endothelial injury as the primary pathogenic event, followed by immune activation and progressive fibrotic remodeling in the skin and internal organs. Consequently, there is a vascular damage with capillary loss that cannot be counterbalanced by vascular repair. The aberrant angiogenic process perpetuates SSc‑related microangiopathy and contributes to the severity of vascular complications, including digital ulcers (DUs) and pulmonary arterial hypertension.2-6
Angiopoietins, along with vascular endothelial growth factor (VEGF), have been recognized as regulators of abnormal vascular remodeling in SSc.3,7,8 Angiopoietin‑1 (Ang‑1) and angiopoietin‑2 (Ang‑2) are endothelial‑specific growth factors that cooperate with VEGF in new blood vessel formation, vascular homeostasis, and remodeling. They interact with specific tyrosine kinase receptors (Tie‑2) and exert context‑dependent effects in an opposing manner. Ang‑1 is critical for endothelial survival and promotes the maturation of newly formed blood vessels, quiescence and integrity of adult vasculature. Ang‑2 acts as a vessel‑destabilizing factor that enhances angiogenesis in the presence of VEGF but promotes vessel regression if VEGF is insufficient.9,10 Imbalanced Ang‑1/Ang‑2 levels have been reported to associate with a greater severity of the disease, more advanced capillary damage, and microvascular complications such as DUs.7,11-15 Therefore, in the context of the genetic background of the disease, the Ang‑1 and Ang‑2 genes (ANGPT1 and ANGPT2) appear as excellent gene candidates for SSc.
However, to date, there are no reports on genetic polymorphisms of ANGPT1 and ANGPT2 in relation to the risk and clinical course of SSc.
In this preliminary, single‑center, case‑control study, we aimed to determine the predictive capacity of ANGPT1 and ANGPT2 single nucleotide polymorphisms (SNPs) as candidate biomarkers for SSc susceptibility and disease pattern in the Caucasian population of eastern Poland. We selected 3 candidate SNPs: rs2507800 (ANGPT1), rs2442598, and rs3739390 (ANGPT2) based on documented data suggesting their role in other vascular or autoimmune disorders.16-22 Subgroup analysis was performed to validate the possibility that certain SNPs are distinctively associated with specific phenotypes and clinical aspects of the disease. We also explored the effects of the investigated polymorphisms on Ang‑1 and Ang‑2 serum levels.
Patients and methods
A total of 86 individuals were recruited to the study, including a series of 48 consecutive SSc cases and 38 healthy controls (HCs) selected to achieve a similar age and sex distribution in both groups. Patients with SSc were recruited between December 2018 and December 2019 from the Department of Dermatology, and were classified according to the American College of Rheumatology / European Alliance of Associations for Rheumatology (ACR/EULAR) 2013 criteria for SSc.23 Patients with overlap syndromes were excluded. All patients were on a stable treatment regimen for at least 6 months. Demographic features and basic clinical characteristics, including disease subtype (limited vs diffuse form), DUs, interstitial lung disease (ILD), and antinuclear antibodies (ANAs), were collected based on a retrospective analysis of the medical records. HCs were recruited from among outpatient volunteers.
All procedures performed in this study were in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its 2000 revision. The study protocol was approved by the local Bioethics Review Board for clinical research at the Medical University of Lublin. All participants gave their informed consent.
Based on literature search (PubMed and Reference SNP (rs) Report of The National Centre for Biotechnology Information; NCBI SNP database; https://www.ncbi.nlm.nih.gov/snp), a single ANGPT1 SNP (rs2507800 [1414 A>T], chromosome position 107250441) and 2 ANGPT2 SNPs (rs3739390 [161378 C>G] chromosome position 6562969 and rs2442598 [135709 T>C,G] chromosome position 6537300) were selected. Blood samples for genotyping were collected in ethylenediamine tetraacetic acid tubes and stored at –20 °C. Total genomic DNA was extracted with a commercial kit (QIAamp DNA Blood Mini Kit, Qiagen, Germany) following the manufacturer’s protocol. The extracted DNA concentration and purity (A260/230 and A260/280 ratios) were assessed by NanoDrop UV/Vis spectrophotometer (Thermo Fisher Scientific, Waltham, Massachusetts, United States).
The specific SNP alleles of ANGPT1 were determined with a TaqMan SNP Genotyping Assay (Taq Man Probe C_1252396_10 rs2507800 Gene ANGPT1 Location Chr.8:108262669 SNP) on the ABI 7500 Fast Real‑Time Polymerase Chain Reaction (PCR) System (Applied Biosystems, Foster City, California, United States) according to the manufacturer’s instructions. Genotyping of ANGPT2 was performed by automated DNA Sanger sequencing with the BigDye Terminator v3.1 Cycle Sequencing Kit in an ABI 7500 Fast Real‑Time PCR System (Applied Biosystems). The sequencing PCR products were purified using an exterminator kit (A&A Biotechnology, Gdańsk, Poland), and then analyzed using an ABI 3130 Genetic Analyzer (Applied Biosystems) with a dedicated Applied Biosystems software (Supplementary material, Figure S1). Additional data on the sequences and length of the ANGPT2 rs3739390 and rs2442598 SNPs probes are presented in Supplementary material, Table S1.
Serum levels of Ang‑1 and Ang‑2 were quantified using the Human Angiopoietin‑1 and Angiopoietin‑2 Quantikine ELISA Kits (R&D Systems Inc, Minneapolis, Minnesota, United States) according to the manufacturer’s instructions.
Statistical analysis
Statistical analysis was performed using Statistica software, version 13.3 (StatSoft, Kraków, Poland). Data expressed on a qualitative scale were presented as the number and percentage of the sample. The Hardy–Weinberg equilibrium (HWE) was determined by the χ2 test. The χ2 test, χ2 test with Yates correction or the Fisher exact probability test were used to compare the prevalence of sex between the study and control groups as well as the disease type and clinical symptoms depending on the genotype or allele. The odds ratios (ORs) and 95% CIs for associations between the allelic or genotype frequencies and the risk of SSc as well as clinical characteristics of the disease were estimated by logistic regression models. Genotype distribution between study patients and controls was determined by logistic regression using additive, dominant, and recessive models. Data expressed on a quantitative scale were presented as a mean with SD or as a median with interquartile range, as appropriate. Depending on the number of compared groups and the result of the Shapiro–Wilk test (assessment of compliance with the normal distribution), the following tests were used: the 1‑way analysis of variance, the t test, and the Mann–Whitney test. The results were considered statistically significant when P was less than 0.05.
Results
All participants enrolled in the study were of Caucasian ethnicity. The mean (SD) age of SSc patients was 54.69 (12.29) years and of HCs, 52.26 (9.16) years (P = 0.38). Women constituted 97.95% (n = 47) and 100% of the SSc and control groups, respectively (P = 0.91). All study patients fulfilled the ACR/EULAR 2013 classification criteria for SSc.23 Of these, 40 patients had limited cutaneous systemic sclerosis (lcSSc), and 8 had diffuse cutaneous systemic sclerosis (dcSSc) based on the criteria proposed by LeRoy et al.24 The median time of disease duration (ie, the interval between the disease onset and blood collection) was 6 years, and 24.49% of SSc patients had active disease at the time of blood sampling. All SSc patients were ANA–positive; among them, 51.02% were positive for ACA and 44.89%, for Scl‑70. A history of DUs was present in 25% of patients.
The results of Ang‑1 and Ang‑2 serum levels were obtained for 44 patients with SSc. Serum levels of Ang‑1 were significantly lower, with a median value of 15081.15 (8005.13–24075.65) pg/ml, whereas serum levels of Ang‑2 were significantly higher (a median value of 2684.98 [2139.91–3725.70] pg/ml) among SSc patients compared with HCs (31090.75 [22799.90–36192.75] pg/ml; P <0.001 and 1503.31 [1379.96–1868.09] pg/ml; P <0.001, respectively). Baseline demographic data and clinical variables of both groups as well as a comparison of Ang‑1 and Ang‑2 serum levels are summarized in Table 1.
Variable | SSc patients (n = 48) | Healthy controls (n = 38) | P value | |||
Data are presented as number (percentage) unless otherwise indicated.
a Compared with the t test
b Compared with the χ2 test with Yates continuity correction
c Compared with the Mann–Whitney test
Abbreviations: ANAs, antinuclear antibodies; Ang‑1, angiopoietin 1; Ang‑2, angiopoietin 2; CYC, cyclophosphamide; DCO(SB), pulmonary diffusing capacity for carbon monoxide‑single‑breath; HRCT, high‑resolution computed tomography; IQR, interquartile range; mRSS, modified Rodnan Skin Score; N/A, not applicable; SSc, systemic sclerosis; TLC, total lung capacity | ||||||
Age, y, mean (SD); range | 54.69 (12.29); 20–74 | 52.26 (9.16); 35–80 | 0.38a | |||
Sex | Female | 47 (97.92) | 38 (100) | 0.91b | ||
Male | 1 (2.08) | 0 | ||||
Disease subtype | Limited | 40 (83.33) | – | – | ||
Diffuse | 8 (16.66) | – | ||||
SSc duration, y; median (IQR); range | 6.0 (4.0–9.5); 1–28 | – | – | |||
mRSS, median (IQR); range | 8.0 (6.0–12.0); 3–22 | – | – | |||
Digital ulcers | 12 (25) | – | – | |||
ANAs | ANA‑positive | 48 (100) | – | – | ||
Anti‑Scl‑70 | 22 (45.83) | – | ||||
ACA | 25 (52.08) | – | ||||
Anti‑polymerase III | 1 (2.08) | – | ||||
Interstitial lung disease on HRCT | 35 (71.42) | – | – | |||
DCO(SB), mean (SD); range | 76.52 (19.76); 30–110 | – | – | |||
DCO(SB) | >80% | 21 (42.86) | – | |||
<80% | 19 (38.77) | – | ||||
N/A | 9 (18.37) | – | ||||
TLC, mean (SD); range | 108.44 (23.74); 62–158 | – | – | |||
TLC | >80% | 36 (73.47) | – | – | ||
<80% | 6 (12.24) | – | ||||
N/A | 7 (14.28) | – | ||||
Active disease | 12 (24.49) | – | – | |||
Treatment | Prenisolone, 5–10 mg every day | 47 (100) | – | – | ||
Pentoxifylline, 400 mg twice a day | 47 (100) | – | ||||
Sulodexide, 250 mg twice a day | 47 (100) | – | ||||
Sildenafil, 25 mg twice a day | 21 (44.6) | – | ||||
CYC pulse, intravenously every 4 weeks | 15 (32) | – | ||||
Serum Ang‑1, pg/ml, median (IQR) | 15081.15 (8005.13–24075.65) | 31090.75 (22799.90– 36192.75) | <0.001c | |||
Serum Ang‑2, pg/ml, median (IQR) | 2684.98 (2139.91–3725.70) | 1503.31 (1379.96–1868.09) | <0.001c | |||
SNP genotyping was successful in all enrolled individuals. The HWE test showed that in both groups, the genotype distribution of the investigated polymorphisms was in the HWE, except for ANGPT2 rs2442598 (P <0.001), as presented in Supplementary material, Table S2.
There were no statistically significant differences in the allelic frequency of the investigated SNPs between the SSc and control groups, except for alleles C and T over the rs2442598 site of the ANGPT2 gene (P = 0.03). The rs2442598 C allele frequency was significantly higher in the SSc patients, and it was associated with a 2.28‑fold higher risk for SSc (OR, 2.277; 95% CI, 1.013–5.117; P = 0.04) compared with the T allele. The detailed allelic frequencies of the investigated SNPs in both groups are compared in Table 2.
Gene | SNP | Reference allele | Alternative allele/-s | Risk allele | P valuea | OR (95% CI) | ||||
SSc patients | Healthy controls | SSc patients | Healthy controls | |||||||
Data are presented as number (percentage). Odds ratios with their 95% CIs were estimated by logistic regression models.
a P value for allelic frequencies (maximum likelihood χ2 test)
b Significant at P = 0.04
Abbreviations: ANGPT1, angiopoietin‑1 gene; ANGPT2, angiopoietin‑2 gene; OR, odds ratio; SNPs, single nucleotide polymorphisms; others, see Table 1 | ||||||||||
ANGPT1 | rs2507800 | T | A | A | 0.2 | 1.554 (0.788–3.063) | ||||
50 (61) | 51 (71) | 32 (39) | 21 (29) | |||||||
ANGPT2 | rs3739390 | C | G | C | 0.25 | 0.598 (0.246–1.451) | ||||
74 (88) | 62 (82) | 10 (12) | 14 (18) | |||||||
ANGPT2 | rs2442598 | T | C | G | C | 0.03 | 2.277 (1.013–5.117)b | |||
13 (15) | 19 (25) | 67 (80) | 43 (57) | 4 (5) | 14 (18) | G | 0.646 (0.328–1.269) | |||
Next, we analyzed the effect of the investigated genotypes on the susceptibility to developing SSc using 3 different genetic models (additive, dominant, and recessive), except for ANGPT2 rs2442598, in which only the additive model was used due to 2 alternative alleles found for this SNP. The AA and AT genotypes of the ANGPT1 gene were analyzed as a single group in the dominant model because the frequency of AA homozygotes was very low in both groups—12% (5 cases) in SSc patients and 8% (3 cases) in HCs. Similarly, for ANGPT2 rs3739390, the frequency of the CG genotype was very low (12% [5 cases] and 16% [6 cases] in the study and control groups, respectively), and GG homozygotes were identified exclusively in the control group. Thus, both genotypes were additionally analyzed in a cluster.
There were significant differences in genotype distribution of ANGPT2 rs2442598 between the SSc cases and controls. According to the additive model for rs2442598, the CC genotype was found significantly more often in the SSc group compared with HCs. Individuals carrying the risk CC genotype were 3.29‑fold more likely to develop SSc (OR, 3.288; 95% CI, 1.212–8.915; P = 0.02) compared with carriers of the CT genotype, indicating a potential strong association between the CC genotype of the ANGPT2 rs2442598 SNP and SSc susceptibility.
With respect to other analyzed SNPs, the genotype frequencies were comparable between the SSc and control groups, and consequently, no significant association was found in terms of the general likelihood to develop SSc in the study group. Of note, the GG genotype of the ANGPT2 rs3739390 SNP was identified exclusively in the control group; however, due to the relatively small sample size, any conclusive association with susceptibility to the disease could not be determined. The results are summarized in Table 3. The representative allelic discrimination plot for ANGPT1 rs2507800 is presented in Supplementary material, Figure S2.
Gene | SNP | Genetic model | ||||
Genotype | SSc patients | Healthy controls | OR (95% CI) | P value | ||
Data are presented as number (percentage). Odds ratios with their 95% CIs were estimated by logistic regression models.
a The GG genotype of the rs3739390 polymorphism in the ANGPT2 gene was identified exclusively in the healthy control group.
| ||||||
ANGPT1 | rs2507800 | Additive model | ||||
TT | 14 (34) | 18 (50) | 1.00 (reference) | – | ||
AT | 22 (54) | 15 (42) | 1.885 (0.710–5.004) | 0.19 | ||
AA | 5 (12) | 3 (8) | 1.463 (0.643–3.332) | 0.35 | ||
Dominant model [TT/AT+AA] | ||||||
TT | 14 (34) | 18 (50) | 1.00 (reference) | – | ||
AT+AA | 27 (66) | 18 (50) | 1.928 (0.758–4.904) | 0.16 | ||
Recessive model [AA/AT+TT] | ||||||
AA | 5 (12) | 3 (8) | 1.00 (reference) | – | ||
AT+TT | 36 (88) | 33 (92) | 0.654 (0.141–3.029) | 0.58 | ||
ANGPT2 | rs3739390 | Additive model | ||||
CC | 37 (88) | 31 (81) | 1.00 (reference) | – | ||
CG | 5 (12) | 6 (16) | 0.698 (0.190–2.560) | 0.58 | ||
GG | 0 (0) | 1 (3) | N/Aa | N/Aa | ||
Dominant model [CC/CG+GG] | ||||||
CC | 37 (88) | 31 (81) | 1.00 (reference) | – | ||
CG+GG | 5 (12) | 7 (18) | 0.598 (0.169–2.115) | 0.42 | ||
Recessive model [GG/CC+CG] | ||||||
GG | 0 (0) | 1 (3) | 1.00 (reference) | N/Aa | ||
CC+CG | 42 (100) | 37 (97) | N/Aa | |||
rs2442598 | Additive model | |||||
CT | 13 (31) | 19 (50) | 1.00 (reference) | – | ||
CC | 27 (64) | 12 (32) | 3.288 (1.212–8.915) | 0.02 | ||
GG | 2 (5) | 7 (18) | 0.646 (0.265–1.571) | 0.32 | ||
The allelic frequency and genotype distribution of respective SNPs of ANGPT1 and ANGPT2 genes were then analyzed for their association with selected clinical variables of SSc patients, including disease subtype (lcSSc vs dcSSc), ANAs (ACA vs anti‑Scl‑70), and ILD on high‑resolution computed tomography. Particular attention was paid to the history of DUs, which constitutes a common clinical feature related to microvascular involvement in SSc.
There were significant differences in the allelic frequency and genotype distribution of the rs3739390 polymorphism according to the disease subset. Patients carrying the rs3739390 G allele as well as the CG and CG+GG genotypes of the ANGPT2 gene were 9‑fold more likely to develop dcSSc than lcSSc compared with individuals with the C allele or CC genotype (OR, 9.00; 95% CI, 2.102–38.519; P = 0.002 and OR, 9.00; 95% CI, 1.112–72.824; P = 0.03, respectively). In contrast, according to the recessive model, the likelihood to develop dcSSc was 8.771‑fold lower in individuals with the TT+AT genotype of the rs2507800 SNP (ANGPT1) compared with the AA homozygotes (OR, 0.114; 95% CI, 0.014–0.932; P = 0.04) (Table 4).
Data are presented as number (percentage). Odds ratios and their 95% CIs were estimated by logistic regression models.
Between OR and 95% CIs, the information is added which category (group) is an outcome for the analysis according to either the dominant or recessive model
a P value for allelic frequencies (the maximum likelihood χ2 test)
| |||||||||||||||
SNPs | Clinical variable | Allelic frequency | Genotype frequency | ||||||||||||
Additive model | Dominant model | Recessive model | |||||||||||||
ANGPT1 | Disease subtype | T | A | P valuea | OR (95% CI) | TT | AT | AA | OR [TT/AT] (95% CI) | OR [TT/AA] (95% CI) | AA+AT | OR [TT/AA+AT] (95% CI) | TT+AT | OR [AA/TT+AT] (95% CI) | |
rs2507800 | lcSSc | 40 (65) | 22 (35) | 0.13 | 1.00 (ref.) | 11 (35) | 18 (58) | 2 (7) | 1.00 (ref.) | 1.00 (ref.) | 20 (64.5) | 1.00 (ref.) | 29 (93.5) | 1.00 (ref.) | |
dcSSc | 7 (44) | 9 (56) | 2.337 (0.751–7.268) | 2 (25) | 3 (37.5) | 3 (37.5) | 0.916 (0.122–6.880) | 2.872 (0.81–10.176) | 6 (75) | 1.650 (0.267–10.192) | 5 (62.5) | 0.114 (0.014–0.932) | |||
P = 0.04 | |||||||||||||||
ANGPT2 | Disease subtype | C | G | P valuea | OR (95% CI) | CC | CG | GG | OR [CC/CG] (95% CI) | CG+GG | OR [CC/CG+GG] (95% CI) | CC+CG | OR [GG/CC+CG] (95% CI) | ||
rs3739390 | lcSSc | 60 (94) | 4 (6) | 0.003 | 1.00 (ref.) | 30 (94) | 2 (6) | 0b | 1.00 (ref.) | 2 (6) | 1.00 (ref.) | 32 (100) | N/A | ||
dcSSc | 10 (62) | 6 (38) | 9.00 (2.102–38.519) | 5 (63) | 3 (38) | 0b | 9.00 (1.112–72.824) | 3 (38) | 9.00 (1.112–72.824) | 8 (100) | N/A | ||||
P = 0.03 | |||||||||||||||
P = 0.003 | P = 0.03 | ||||||||||||||
ANGPT2 | DU status | C | G | P valuea | OR (95% CI) | CC | CG | GG | OR [CC/CG] (95% CI) | CG+GG | OR [CC/CG+GG] (95% CI) | CC+CG | OR [GG/CC+CG] (95% CI) | ||
rs3739390 | DUs (–) | 58 (91) | 6 (9) | 0.04 | 1.00 (ref.) | 29 (91) | 3 (9) | 0 (0) | 1.00 (ref.) | 3 (9) | 1.00 (ref.) | 32 (100) | N/A | ||
DUs (+) | 8 (67) | 4 (33) | 4.833 (1.089–21.437) | 4 (67) | 2 (33) | 0 (0) | 4.833 (0.566–41.255) | 2 (33) | 4.833 (0.566–41.255) | 6 (100) | N/A | ||||
P = 0.03 | |||||||||||||||
For the rs3739390 SNP of ANGPT2, the C allele was significantly more frequent among SSc patients without DUs than in cases with this complication (P = 0.04) and it was associated with a 4.83‑fold lower risk of developing DUs in this group (OR, 4.833; 95% CI, 1.089–21.437; P = 0.03) compared with the G allele.
None of the other analyzed features of the disease, including ILD and ANAs, were associated with the investigated SNPs. The associations between the studied SNPs and SSc characteristics are presented in detail in Supplementary material, Tables S3 and S4.
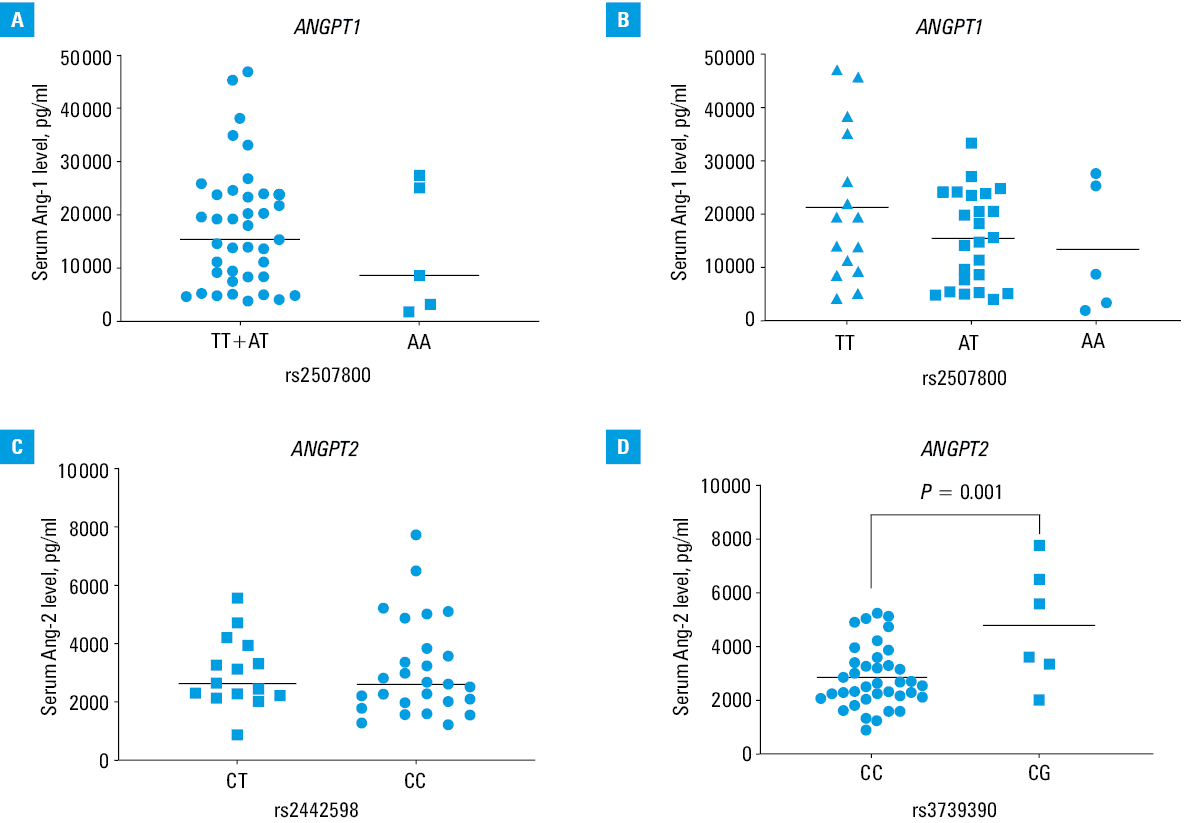
No significant differences in serum Ang‑1 levels were found among SSc patients carrying the TT, AT, and AA genotypes of rs2527800, although those with either the TT (mean [SD], 21219.59 [14279.25] pg/ml) or TT+AT (median [IQR], 15467.80 [8422.09–24054.20] pg/ml) variant tended to have higher levels of Ang‑1 than the AA homozygotes (mean [SD], 13 323.14 [12260.88] pg/ml; P = 0.22 and median [IQR], 8673.00 [3258.85–25280.20] pg/ml; P = 0.46, respectively) (Figure 1A and 1B). Patients carrying either the CT or CC genotype of ANGPT2 rs2442598 had comparable serum concentrations of Ang‑2 (P = 0.73) (Figure 1C). With respect to ANGPT2 rs3739390, SSc patients with the CC genotype presented significantly lower serum Ang‑2 concentrations (mean [SD], 2839.38 [1141.44] pg/ml) compared with those carrying the CG variant (mean [SD], 4798.35 [2179.60] pg/ml; P = 0.001) (Figure 1D).
Discussion
To the best of our knowledge, this study is the first to highlight the association of either ANGPT1 or ANGPT2 polymorphism with SSc.
The ANGPT1 and ANGPT2 genes are localized on human chromosomes 8q22.3→q23 and 8p23.1, respectively.25 ANGPT1 encodes Ang‑1 and is expressed predominantly by perivascular cells such as pericytes, vascular smooth muscle cells, and fibroblasts. The ANGPT2 gene encodes Ang‑2, and endothelial cells have been identified as its primary source. The ANGPT2 gene is highly polymorphic, and SNPs may alter its expression, while polymorphism in ANGPT1 seems to be less common.26
The prognostic value of ANGPT1 and ANGPT2 polymorphisms has been reported in various human pathologies. They have been suggested as susceptibility genes for acute respiratory distress syndrome, trauma‑associated acute lung injury, obstetric diseases, stroke, cancers, neovascular age‑related macular degeneration, polypoidal choroidal vasculopathy, premature retinopathy,16-20,27,28 psoriasis,21 and recently, for autoimmune connective tissue diseases.22,29-31
Specifically, our findings suggest that the ANGPT2 rs2442598 (135709 T>C) polymorphism has a potential strong association with a higher overall risk of SSc in the analyzed population of White ancestry. Carriers of the allelic variant C of rs2442598 had a 2.28‑fold higher likelihood to develop SSc compared with those with the wild‑type allele (T), and consequently, the presence of the rs2442598 CC genotype was associated with a higher disease susceptibility compared with carrying the CT variant. Thus, with respect to disease‑related variability of the ANGPT2 rs2442598 SNPs, our findings may suggest that allele C seems to be a risk allele for SSc and the CC genotype may be a unique candidate genetic marker of SSc susceptibility.
In contrast, in psoriasis vulgaris the CT+TT genotype of rs2442598 has been reported to increase the risk of the disease in the Han population of northern China,21 and Dai et al22 found that the TT genotype of the rs2442598 SNP was related to a higher risk for rheumatoid arthritis in patients of Chinese origin compared with those carrying the AA genotype. It also has been reported that the ANGPT2 rs2442598 polymorphisms are strongly associated with acute lung injury in patients after major trauma16 but not with systemic lupus erythematosus (SLE).29 The reported divergence may relate not only to the heterogeneity among different diseases but also different ethnicities (Chinese vs European ancestry) and sample size.
Although a significant association between the ANGPT2 rs3739390 SNP and susceptibility to SSc has been shown in our White patients, it is worth noting that the rs3739390 GG homozygotes were identified exclusively in HCs. However, due to a relatively small sample size, any conclusive association with disease development could not be determined. In comparison, in a recent study by Wang et al,29 the frequency of the G allele as well as the GC and GG+GC genotypes of rs3739390 were lower in the Chinese population of SLE patients as compared with healthy individuals, and negatively correlated with SLE susceptibility.
In addition, our results showed that the ANGPT2 gene polymorphisms are also associated with certain clinical variables among the SSc patients of White ethnicity.
First, we identified a difference in the distribution of the ANGPT2 rs3739390 (161 378 C>G) genetic variants between diffuse and limited disease subtypes, although it was not associated with overall disease susceptibility. Namely, the individuals carrying the ANGPT2 rs3739390 G allele or CG genotype had a 9‑fold higher risk of developing dcSSc compared with carriers of either the wild‑type C allele or CC homozygotes. On the contrary, in our analysis according to the recessive model, the ANGPT1 rs2507800 TT+AT genotype seemed to significantly decrease risk of dcSSc compared with AA homozygotes. This finding fits well to the antagonistic model of Ang‑1 and Ang‑2 functions and might support a concept of their opposite effect in SSc as well.7,9-11,15 No comparable genetic studies are available for SSc. With respect to SLE patients, recent data from Wang et al29 showed that those carrying the ANGPT2 rs3739390 G allele were more likely to develop symptoms of hematuria and hypocomplementemia, and the GC genotype of rs3739390 was more prevalent in patients with anti–double‑stranded‑DNA antibodies, which are associated with more severe variants of the disease.29 In contrast, in patients with stroke, the G allele of ANGPT2 rs3739390 conferred a lower risk of lacunar infarction than the corresponding C allele.32
Moreover, in terms of clinical variables, we elucidated the ANGPT2 rs3739390 wild‑type C allele as a significant protective factor for DUs in our group of SSc patients. Digital ulcers are thought to constitute an important clinical manifestation of SSc‑related microangiopathy related to capillary loss and impaired angiogenesis that correspond in vitro with a sustained increase in Ang‑2 expression.5,7,11,15,33-37 However, no data have been reported yet specifically concerning DUs and angiopoietin polymorphisms in SSc. Some studies found other gene polymorphisms to be associated with a lower risk of DUs in SSc, including matrix metalloproteinase 9 rs3918242 SNPs in male patients and the TIMP‑1 rs4898 polymorphism in females SSc patients of White Italian origin.38,39
Given that Ang‑1/Ang‑2 serum concentrations are known to be altered in SSc patients, and that some ANGPT1 and ANGPT2 SNPs seem to affect their levels in other pathological conditions,28,32,40,41 we additionally explored the possible effect of the analyzed genetic variants of ANGPT1 and ANGPT2 on serum levels of their corresponding proteins in patients with SSc. Serum Ang‑2 levels were significantly increased in SSc cases in contrast to HCs and varied substantially by the ANGPT2 rs3739390 genotype. The CC genotype of rs3739390 conferred lower Ang‑2 levels than the CG variant. It corresponds well to the association between the C allele or CC genotype of ANGPT2 rs3739390 and a lower risk of either DUs or dcSSc reported in this study. Thus, along with the predicted pathogenic potential of increased serum Ang‑2 levels in SSc,7,11-15,42,43 our findings may offer 2 suggestions: 1) an indirect effect of ANGPT2 rs3739390 in SSc, that is, mediated through the Ang‑2 serum concentration, and 2) a possible preventive role of the rs3739390 C allele against digital vascular complications and a more severe disease subtype through lower Ang‑2 serum levels.
It must be noted that the functional role of the rs3739390 polymorphism is still not well documented; however, SNP function prediction tools reveal that this polymorphism is located in the 5‑prime untranslated region (5´-UTR) of the ANGPT2 gene in a block with rs3739391 and 3739392, and its SNPs may result in 5´-UTR variant or intron variant (NCBI SNP database, https://www.ncbi.nlm.nih.gov/snp/?term=rs3739390). Of note, alterations in 5´-UTR as well as the 3´-UTR are known to contribute to the post‑transcriptional regulation of gene expression.26,44 Moreover, TATA‑less and initiator‑less promoters as well as strong repressor elements of ANGPT2-promoter activity have been recently identified within the 5´-UTR of the ANGPT2 gene.45 It was also suggested that the 5´-UTR might be part of transcription factor binding sites and probably has an effect on protein synthesis.27,45 Consequently, ANGPT2 rs3739390 SNPs may result in a variance of endothelial cell‑specific and cytokine‑dependent Ang‑2 expression and its serum levels in different pathological conditions.
With respect to ANGPT2 rs2442598, serum Ang‑2 levels did not vary predictably by their genotypes. Since the ANGPT2 rs2442598 polymorphism correlated with an overall disease susceptibility in our SSc group, we believe that this correlation may result from direct effects of given SNPs or a shift in Ang‑2 isoform ratio in the plasma without an overall level change when measured by ELISA, as has been shown for rs1868554 T allele carriers with acute lung injury.16 In fact, similarly to our results, Wang et al29 reported comparable serum Ang‑2 concentrations among SLE patients irrespective of ANGPT2 rs2442598 genotypes.29
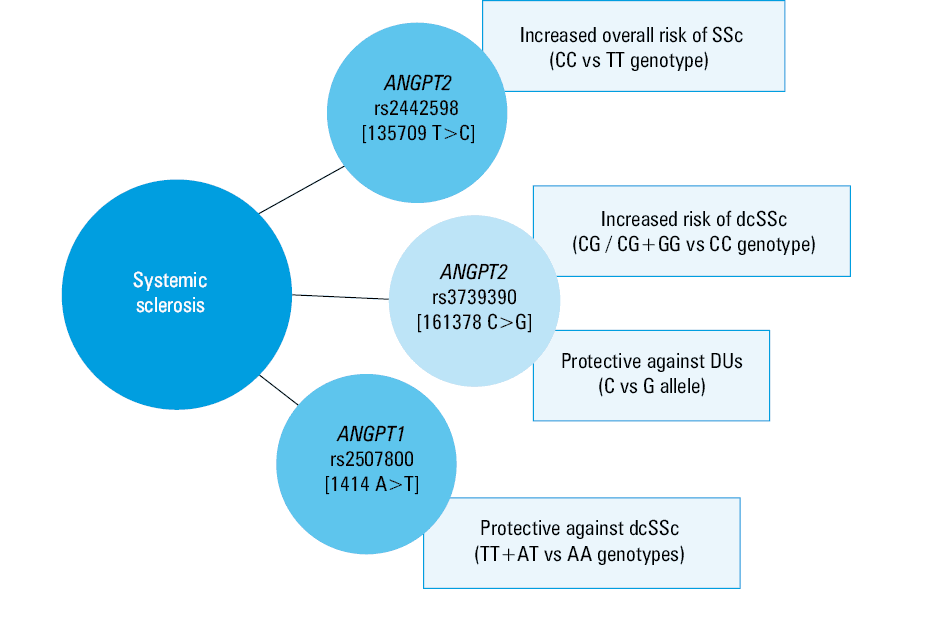
Importantly, Ang‑1 serum concentrations tended to be higher in our study patients with the TT genotype of ANGPT1 rs2507800 than in those with the AT or AA variants, although not significantly, possibly due to a power limitation caused by the low number of individuals recruited in the study. Of note, the A allele has been shown to suppress Ang‑1 translation by facilitating miRNA‑211 binding, while the T allele is resistant to miRNA‑211–induced reduction in translation. Thus, the TT genotype may be potentially associated with higher serum Ang‑1 levels compared with the AA genotype, as was recently shown in patients with stroke, women with preeclampsia, hypertensive small‑for‑gestational‑age (SGA) neonates, and SGA with abnormal uterine artery Doppler.40,41 These findings allow us to hypothesize that the ANGPT1 rs2527800 TT or TT+AT genotypes in SSc individuals may protect against a diffuse subtype of the disease by increasing Ang‑1 production; however, this needs to be confirmed. If significant in a larger group, our findings may be of significant prognostic and diagnostic value in view of the plausible role of low Ang‑1 levels in SSc‑related microangiopathy.7,11 Associations of the investigated ANGPT1 and ANGPT2 SNPs with disease susceptibility and phenotype found in this study are summarized in Figure 2.
We are aware of several limitations in our research, including a small sample size (partly due to the low disease incidence), restriction to a single population and region as well as a significant female predominance, which are likely to limit the statistical power and cause a selection bias. Therefore, replication in multi‑center studies with a greater number of enrolled individuals will be beneficial. Moreover, the number of assessed SNPs was limited; however, this study was preliminary and the first of its kind, thus we chose to test only those polymorphisms that are well documented. Another limitation of this study is the absence of a functional analysis and gene‑targeted assays. Consequently, future research with more ANGPT1 / ANGPT2 gene loci and their functional role seems necessary.
Our study also has some strengths, including the pioneer identification of a consistent genotypic association of the ANGPT2 rs2442598 polymorphism with SSc susceptibility as well as an ethnically homogenous population of European ancestry that reduces genetic admixture.
In conclusion, this study shows for the first time that ANGPT2 rs2442598 may represent a susceptibility locus for SSc in a Polish Caucasian population. Hence, ANGPT2 may be involved in SSc development as a genetic marker or a causative polymorphism, although the exact function of the rs2442598 SNP is to be established. We also confirmed that the ANGPT2 rs3739390 SNP may significantly increase the risk for a more severe diffuse subtype of the disease and history of DUs, whereas the ANGPT1 rs2507800 genetic variants are associated with a reduced dcSSc risk with no effects on SSc susceptibility per se. Thus, these should be considered disease‑modifying gene variants rather than disease‑susceptibility SNPs in SSc. Of note, these polymorphisms do not seem to be a candidate gene for either ILD or ANA specificity in our White population.
In spite of some limitations, these preliminary results could provide reference information to drive subsequent studies on a larger cohort to highlight the correlations between clinical variables and the genetic function of ANGPT1 / ANGPT2 polymorphisms in SSc; in particular, their potential role in early screening to predict the risk of SSc, course of the disease, and future genetic target of personalized therapies.
- Bergamasco A, Hartmann N, Wallace L, et al. Epidemiology of systemic sclerosis and systemic sclerosis‑associated interstitial lung disease. Clin Epidemiol. 2019; 11: 257‑273. | Crossref
- Matucci‑Cerinic M, Kahaleh B, Wigley FM. Review: evidence that systemic sclerosis is a vascular disease. Arthritis Rheum. 2013; 65: 1953‑1962. | Crossref
- Cantatore FP, Maruotti N, Corrado A, Ribatti D. Angiogenesis dysregulation in the pathogenesis of systemic sclerosis. Biomed Res Int. 2017; 2 017: 5345673. | Crossref
- Sierra‑Sepúlveda A, Esquinca‑González A, Benavides‑Suárez SA, et al. Systemic sclerosis pathogenesis and emerging therapies, beyond the fibroblast. Biomed Res Int. 2019; 2 019: 4569826. | Crossref
- Chung L, Fiorentino D. Digital ulcers in patients with systemic sclerosis. Autoimmun Rev. 2006; 5: 125‑128. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION