The effect of plant-based diets on thrombotic risk factors
Key words: coagulation, dietary patterns, plant-based, thrombosis, vegetarian



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
The effect of plant-based diets on thrombotic risk factors
Plant‑based diets are considered to improve cardiometabolic health and to protect against cardiovascular disease. Although they center around plant‑based foods, they do not necessarily exclude all animal products and comprise of a range of intakes that vary according to the type and the proportion of animal products included. Numerous metabolic pathways have been identified through which plant‑based diets can exert beneficial effects including improved body composition, lipid profile, and glucose metabolism and decreased inflammation and blood pressure. Their effects on thrombosis as a cardiovascular disease pathway are, however, less clear. Ample evidence for the effects of individual dietary components of plant‑based diets on thrombotic risk factors exists, but the effect of whole diets and / or dietary patterns remains less‑well explored with the existing literature reporting inconsistent and inconclusive findings. Here we aim to review the literature describing the effect of different plant‑based diets (vegan, lacto‑vegetarian, lacto‑ovo‑vegetarian, pescatarian, and flexitarian) and dietary patterns (Mediterranean, Nordic, Portfolio, and DASH) on specific thrombotic risk factors (fibrinogen, platelets, factor VII, fibrinolysis) in order to better clarify these relationships and to try to explain the apparent discrepant findings. We demonstrate that a one‑size‑fits‑all conclusion cannot be drawn and that the potential antithrombotic effect of different plant‑based diets depends on the nutrient composition, the content of active antithrombotic dietary components, the relative absence of prothrombotic dietary factors as well as the degree of total caloric restriction.
Introduction
Plant‑based diets primarily contain foods of plant origin, which include not only vegetables and fruit, but also nuts and seeds, legumes and beans, oils, and whole grains. Plant‑based diets do not necessarily exclude all animal products and can range from total exclusion (eg, vegan) to meat consumption once to twice a week (eg, flexitarian). The unifying focus is on the consumption of more foods from plant sources proportional to animal‑based foods.1
Consumption of plant‑based diets have been associated with a significant reduction in cardiovascular disease (CVD) risk,2-4 CVD mortality,5,6 and also all‑cause mortality.7,8 The beneficial effect of plant‑based diets on cardiometabolic health has been attributed to, amongst others, the low caloric density, lower saturated fat, and higher mono- and polyunsaturated fat content, high fiber content as well as its antioxidant and anti‑inflammatory compounds.1
Randomized control trials and observational studies have identified a number of pathways through which plant‑based diets can improve cardiometabolic health. These include a number of risk factors recognized by the European Society of Cardiology guidelines for CVD prevention9: reduction of obesity and its downstream sequelae, improved glycemic control and decreased insulin resistance, decreased blood pressure, and an improved lipid profile (reviewed by Kahleova et al10). In addition, plant‑based diets have been shown to improve other CVD‑related pathways such as cessation and reversal of atherosclerotic plaque deposition, decreased inflammation and thrombosis. There is a vast amount of literature investigating the relationship of diet with thrombosis, but most of these studies assessed the effect of individual nutrients or foods such as alcohol, dietary fat, n‑3 fatty acid supplementation, fiber, carbohydrates, and a variety of micronutrients (vitamins, minerals and phytochemicals) (reviewed by Pieters and De Maat11). Much less is known regarding the influence of whole diets—in particular, plant‑based diets and dietary patterns—on thrombotic factors such as platelet aggregation, coagulation, and fibrinolysis, with the existing literature reporting inconsistent and inconclusive findings. This is likely the result of the differences in composition of the investigated plant‑based diets (ranging from strictly vegan, to diets containing some meat or even high intakes of fish), the specific outcomes measured, and differences in study designs such as randomized controlled trials or observational studies, duration, selection of control groups, and health status of the participants (eg, healthy vs patients with CVD). Here we aim to review the existing literature describing the effect of different plant‑based diets (but not the individual constituent nutrients or foods) on specific thrombotic risk factors in order to better clarify these relationships and to try to explain the apparent discrepant findings. The thrombotic factors the review will focus on include platelet function, coagulation proteins (fibrinogen and factor VII [FVII]), and fibrinolysis, as most of the available evidence focuses on these outcomes.
Plant‑based diets
We first describe the composition of different plant‑based diets and dietary patterns in order to better interpret their potential varying effects on the discussed thrombotic factors. The 2021 European Society of Cardiology guidelines on CVD prevention in clinical practice recommend the adoption of a more plant‑based and less animal‑based food pattern consisting of less than 10% of total energy from saturated fatty acids, less than 5 g of salt, 30 to 45 g of fiber, at least 200 g of fruit, and at least 200 g of vegetables per day. They also recommend red meat consumption of no more than 350 to 500 g per week, with strict minimization of processed meat, (fatty) fish consumption 1 to 2 times per week, 30 g of unsalted nuts per day, no more than 100 g of alcohol per week, and discourage consumption of sugar‑sweetened beverages.9 These guidelines, in essence, describe the underpinning of plant‑based diets.
Although plant‑based diets center around plant‑based foods, they do not necessarily exclude all animal products. Therefore, plant‑based eating is comprised of a range of intakes that vary according to the type and the proportion of animal products included in the diet (Figure 1).
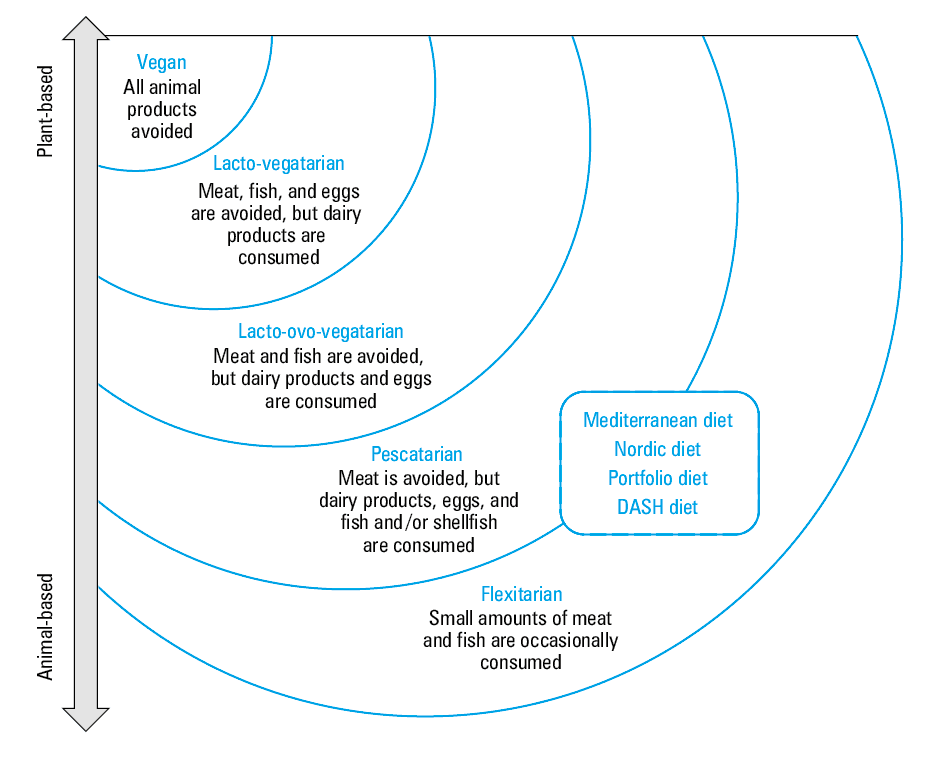
Veganism is considered the purest form of plant‑based eating, characterized by the omission of all animal products from the diet as well as foods that are high in fat, salt, and sugar while only whole food of plant origin is consumed. If not carefully planned and well‑balanced, vegan diets can lead to deficiencies in, amongst others, long‑chain n‑3 polyunsaturated fatty acids and vitamin B12 because of strict exclusion of animal products.12 Lacto‑vegetarian diets, while excluding meat and fish, include dairy products, whereas lacto‑ovo‑vegetarian diets include both dairy and eggs while excluding meat and fish.13 Pescatarian diets, also referred to as pesca‑vegetarian diets, include seafood along with eggs and dairy products while other animal products (poultry and red meat) are not consumed.14 Flexitarian diets, also known as semivegetarian diets, are mainly plant‑based but occasionally include meat, dairy and eggs and focus on variety while attempting to minimize animal product consumption.15
Within the context of the above‑mentioned plant‑based diets, a number of specific plant‑based dietary patterns that fall within the pescatarian and flexitarian diets (depending on whether only fish or both fish and red meat are consumed) have been investigated, and demonstrated to have cardiometabolic health benefits. These include the Mediterranean, Nordic, Portfolio, and DASH diets.13
Mediterranean diet
The Mediterranean diet is based on food patterns observed in the early 1950s in Greece, Crete, and the southern parts of Italy. Keys et al16 noticed in the Seven‑Countries Study that individuals who lived in those parts of the world (ie, in those parts of the Mediterranean region) had the lowest cardiovascular mortality rate whilst consuming the largest amount of fat among the countries included in the study.
Traditional practices included: the addition of olive oil to vegetables and legumes to improve their palatability, fruit rather than sweetened foods was eaten as a daily dessert, salads and stews were accompanied by cheeses, while red meat was reserved for special occasions only.17,18
Today the diet typically does not limit caloric intake; rather, it accentuates variety and the consumption of plant‑based foods with extra virgin, cold‑pressed olive oil (up to 8 servings) as its principal fat source. Plant‑based foods in the Mediterranean diet include vegetables (3–9 servings), fruit (0.5–2 servings), breads and whole grain cereals (1–13 servings), potatoes, nuts, legumes / pulses, seeds, and beans. Fish, poultry, dairy, and (red) wine are consumed in moderation while red meat, saturated fat, eggs, processed foods, and added sugars are limited.13,19 It typically contains high amounts of fiber (>30 g/day), around 35% total fat of which 15% to 20% is monounsaturated fat and less than 10% is saturated fat. Daily caloric intake is in the order of 9300 kJ.20
Nordic diet
The Nordic diet is considered a primarily plant‑based diet with animal products used in moderation, mainly as side dishes.21 Emphasis is placed on traditional Nordic food components, predominantly the healthier options, which are indigenous to and produced locally in the Nordic countries. Some region‑specific variation exists such as the type of fish, berries, fruit, vegetables, and bread that are consumed.22
The overall dietary pattern is based on 3 fundamental guidelines: 1) more calories from plant‑based foods and less from animal‑based foods (especially meat), 2) more foods from the sea and lakes, 3) more food from the countryside (indigenous game and vegetation).23
Plant‑based foods native to the Nordic region include cruciferous vegetables (mainly cabbage), root vegetables (like potatoes), berries (such as bilberries, lingonberries, strawberries, blueberries, cowberries, and cloudberries) and other fruit (like apples and pears), cereals (oats, barley, whole grain, and rye bread) as well as legumes. The long coastline provides a rich source of fatty fish (salmon and herring) and other seafood (shellfish and seaweed). Lean game meat (venison, goose, duck) and low‑fat dairy is also incorporated in the diet.13,24-28
Like the Mediterranean diet, the Nordic diet promotes the consumption of vegetables and fruit, whole grains, and fish, while restricting the use of saturated fat as well as red meat and processed foods. Instead of olive oil as in the Mediterranean diet, rapeseed oil (also known as canola oil) is used as the source of unsaturated fat.22
Portfolio diet
Another plant‑based dietary pattern is the Portfolio diet, which was first formulated in the early 2000s. It consists of a “portfolio” of 4 core food components (all plant‑based) that are known to lower cholesterol, namely: 1) nuts (tree nuts or peanuts); 2) plant‑based protein (soy products, lentils, beans, chickpeas and other legumes); 3) viscous soluble fiber from fruit (apples, oranges, berries), grains (oats, barley, psyllium) and / or vegetables (eggplant, okra); and 4) plant sterols (predominantly plant sterol‑enriched margarine).13,29-33
Jenkins et al34 proposed an enhanced Portfolio diet in which carbohydrates are replaced by monounsaturated fat, which is then added to the established 4 components of the original Portfolio diet to provide around 25% of energy.
DASH diet
The DASH diet, an acronym for “Dietary Approach to Stop Hypertension,” is based on the benefits of a plant‑based diet on blood pressure. This dietary pattern was designed to both treat and prevent hypertension.35,36 The design goal for the DASH diet was to establish plant‑based patterns associated with lowering blood pressure while still incorporating a sufficient amount of animal‑based products to ensure palatability of the diet for nonvegetarian users.36
This dietary pattern is low in fat and rich in carbohydrates. It encourages the intake of fruit, vegetables, whole grains, nuts, and legumes while fish, poultry, and dairy products (fat‑free or low‑fat) are consumed in moderation and dietary cholesterol, total and saturated fat, red meat, processed and refined foods with added sugars are minimized.13,37,38 Compared with regular omnivorous diets, the DASH diet provides more protein, fiber, magnesium, calcium, and potassium.39
Healthy vs unhealthy plant‑based diets
It is important to note that not all plant‑based diets are healthy. Diets high in sugary drinks, refined carbohydrates, and sweets are also plant‑based, but are not considered healthy nor do they have any protective effects in terms of CVD.6,40 Healthy plant‑based diets, therefore, contain high‑quality whole plant foods that are typically rich in dietary fiber, antioxidants, unsaturated fatty acids, and micronutrients. Unhealthy plant‑based diets, on the contrary, typically have a higher glycemic index and load, reduced fiber content, lower micronutrient and higher calorie content, and contain more processed foods.40
For this review, we used combinations of the following keywords in our search strings: plant‑based diets, vegetarian, Mediterranean diet, DASH diet, Portfolio diet, Nordic diet and thrombosis, hemostasis, coagulation, fibrinogen, fibrinolysis, and platelet* (function, aggregation). We found 26 articles that fit the inclusion criteria which will be discussed in the following sections according to the respective thrombotic factors.
Plant‑based diets and fibrinogen
Fifteen studies investigated the association between plant‑based diets and fibrinogen (Table 1), 10 of which were cross‑sectional investigations and 5 were interventions. Of the 10 cross‑sectional studies, 5 reported lower fibrinogen concentration in plant‑based diet consumers (ranging from vegan to flexitarian)41-45 and 5 reported no difference46-50 compared with omnivores. Two studies reported an inverse association between fibrinogen concentration and plant protein and fiber intake44,48 and one an inverse association with the adherence to the Mediterranean dietary pattern.41 One study also reported a positive association between fibrinogen concentration and food patterns containing high intakes of red meat, low‑fiber bread, and dairy products.45 The potential beneficial effect of habitual consumption of plant‑based diets on fibrinogen concentration has been attributed to lower intakes of saturated fats and higher intakes of non‑nutritive components, fish oil (in flexitarian and pescatarian diets) as well as the tendency for vegetarians to have a more‑healthy body mass index—all which have been linked to fibrinogen concentration.51,52 None of the intervention studies ranging from 2 weeks to 6 months, however, demonstrated a beneficial effect of plant‑based diets on reducing fibrinogen concentration.53-57 One study reported an increase in fibrinogen concentration, but this was related to a significant decrease in body mass index.54 Increased fibrinogen during rapid weight loss has been ascribed to a parallel increase in fatty acids which stimulate hepatic fibrinogen production.58 Furthermore, James et al44 previously reported that both under- and overnutrition were associated with higher fibrinogen and that dietary guidelines should therefore focus on preventing overnutrition and its consequences such as noncommunicable diseases, but also they should not be too limiting which could result in undernutrition. In a previous review,59 we concluded that the direct effects of the diet on fibrinogen concentration is likely modest, which is in agreement with the lack of effect observed in the intervention studies, but if the diet results in longer‑term health consequences, such as obesity, insulin resistance or diabetes, the effects become more pronounced.
No. | Study | Study population | Type of diet | Biomarker | Main results |
Abbreviations: BMI, body mass index; CHD, coronary heart disease; CRP, C‑reactive protein; E%, percentage of total energy | |||||
Cross‑sectional | |||||
1 | Corley et al41; the Lothian Birth Cohort 1936 | 792 participants (383 men and 409 women; mean age, 69.5 y); CRP >10 mg/ml excluded; Scotland | Food patterns associated with outcomes identified using principle component analysis:
| Fibrinogen (Clauss) | Fibrinogen was inversely associated with the Mediterranean dietary pattern, fruit intake and combined fruit and vegetable intake. |
2 | Famodu et al42; selection based on habitual intakes | 76 participants:
|
| Fibrinogen (clot weight) |
|
3 | Mezzano et al43 | 54 participants with no comorbidities:
|
| Fibrinogen (Clauss) | Fibrinogen was significantly lower in the vegetarian group compared with omnivorous controls. |
4 | Pan et al46 | 114 participants with no comorbidities:
|
| Fibrinogen (Clauss) | No significant difference in fibrinogen between the vegetarians and omnivores |
5 | Suwannuruks et al47 | 80 participants:
|
| Fibrinogen (the Ellis and Stransky method, 1961) | No significant difference in fibrinogen concentration between the vegetarians and omnivores |
6 | Mia and Vorster48 | 321 Indian adolescents:
|
The Indian vegetarian diet was not lower in fat (>40% TE in both groups) or higher in fiber than the omnivore diet. | Fibrinogen (Clauss) |
|
7 | THUSA44 | 1854 apparently healthy African men and women; age, >15 y; South Africa | The paper investigated the association between nutrient intakes, nutritional status, and fibrinogen concentration. Dietary intakes ranged from traditional low‑fat African diet to more Westernized diets. | Fibrinogen (Clauss) | Participants with the highest intake of dietary fiber and plant protein and with the lowest intake of trans fatty acids and animal protein had the lowest plasma fibrinogen concentration. |
8 | Liese et al45; the Insulin Resistance Atherosclerosis Study | 880 middle‑aged adults, 144 with diabetes mellitus; age, 45–74 y; African American, Hispanic, and non‑Hispanic White participants; USA | Identification of food patterns associated with fibrinogen using reduced rank regression | Fibrinogen (modified clot‑rate assay, Diagnostica STAGO) | Fibrinogen had a positive association with the food pattern containing high intake of red meat, low‑fiber bread and cereal, dried beans, fried potatoes, tomato vegetables, eggs, cheese and cottage cheese and low intake of wine. |
9 | Li et al49 | 139 healthy men; age, 20–50 y:
|
| Fibrinogen (Clauss) | Fibrinogen did not differ between the 4 dietary groups. |
10 | Haines et al50; controls were from the Northwick Park Heart Study | 332 nonsmokers, not using oral contraception; age, 18–65 y:
|
| Fibrinogen (method of Fearnley and Chakrabarti) | There was no significant difference in fibrinogen between the vegetarians and omnivores. |
Intervention | |||||
11 | Kahleova et al53; a 24‑week randomized, parallel study (diet and exercise interventions)
| 74 participants (35 men and 39 women) with type 2 diabetes: 37 vegetarians and 37 controls; age, 30–70 y; Czech Republic |
| Fibrinogen | There was no significant difference in fibrinogen after the first 12‑week diet‑only intervention in either group. Fibrinogen was, however, significantly decreased at the end of the 24‑week intervention period following the addition of 12 weeks of aerobic exercise. This decrease did not differ significantly between the vegetarian and the conventional diabetic diet groups. |
12 | Chainani‑Wu et al54; a 3‑month prospective cohort study nested within a larger cohort (Multisite Cardiac Lifestyle Intervention Program) | 125 participants:
United States (>90% White) | A comprehensive lifestyle intervention that included a low‑fat, whole‑foods, plant‑based diet, exercise, stress management, and group support meetings.
The dietary guidelines prescribed included approximately 10% of daily calories from fat, 15% from protein, and 75% from complex carbohydrates. | Fibrinogen | Significant increase in fibrinogen was observed in the high‑risk CHD group. This increase was inversely correlated to changes in BMI. No change in fibrinogen concentration in the CHD group. |
13 | Brestrich et al55; (article in German, data were taken from the abstract); intervention with the average duration of 24.2 days | 302 participants:
|
| Fibrinogen | There was no diet‑related change in fibrinogen concentration in either the lacto‑vegetarian or the omnivore group. |
14 | Marckmann et al56; a randomized cross‑over study with intervention duration of 2 weeks and a 2‑to‑6‑week washout period | 20 healthy women; age, 21–52 y; BMI, 20–25 kg/m2 | 3 ad libitum experimental diets:
The experimental diets were identical with respect to fish and marine n‑3 polyunsaturated fatty acid content. | Fibrinogen (Clauss) | Plasma fibrinogen was not significantly affected by any of the diets. |
15 | Marckmann et al57; a 2‑week randomized, crossover study | 21 healthy middle‑aged individuals:
5 light smokers;
Denmark |
| Fibrinogen
(Clauss) | Fibrinogen concentration was unaffected by the dietary change. |
Plant‑based diets and platelets
The effect of plant‑based diets on platelet function is varied, as summarized in Table 2. Two of the 6 cross‑sectional studies investigating the association between different plant‑based diets and platelets found increased platelet aggregation / function in vegetarians compared with omnivores.43,49 Three studies found no difference47,60,61 and a single report inhibited platelet activity measured as lower concentrations of platelet‑derived microparticles in individuals consuming a Nordic diet.28 There were also no consistent effects in the 4 intervention studies with durations ranging from 2 weeks to 6 months. Two of the studies (vegetarian and Mediterranean diet [with and without wine]) found increased platelet aggregation with at least one platelet agonist, while no difference in platelet function was reported with other agonists used.62,63 Two studies comparing the DASH diet to a control diet reported decreased platelet activation.64,65 In contrast to plant‑based diets, Mann et al63 found red and white meat not to affect platelet function while fish consumption resulted in a decreased collagen‑stimulated platelet thromboxane production but did not affect platelet aggregation.
No. | Author | Study population | Type of diet | Biomarker | Main results |
Abbreviations: ADP, adenosine diphosphate; AMI, acute myocardial infarction; CAD, coronary artery disease; CXCL4, platelet factor 4; DASH, Dietary Approaches to Stop Hypertension; HFD, high‑fat diet; MD, Mediterranean diet; TXB2, thromboxane B2 | |||||
Cross‑sectional | |||||
1 | Mezzano et al43 | 54 participants with no comorbidities:
Chile |
|
| Vegetarians had significantly higher blood platelet count and in vitro platelet function (aggregation and secretion) than omnivores. |
2 | Li et al49 | 139 healthy men, age, 20–50 y:
nonsmoking |
|
|
|
3 | Fisher et al60 | 50 participants:
|
| Platelet aggregation (ADP, collagen, epinephrine and arachidonic acid) in platelet‑adjusted plasma (250–350 × 109 platelets/l) | Platelet aggregation did not differ between the vegetarians and omnivores. |
4 | Chiva‑Blanch et al28; Omega‑3 Fatty Acids in Elderly Patients with Myocardial Infarction study | 174 patients, 2–8 weeks following AMI; age, 70–82 y; standard medication | Dietary patterns determined from habitual intake. High to low adherence to the Nordic diet (3 groups) | Platelet‑derived microvesicle quantification | A high adherence to the Nordic diet was associated with lower levels of platelet activation, as determined by a lower plasma concentration of platelet‑derived microvesicles. |
5 | Sanders and Roshanai61 | 40 participants with no comorbidities:
No medication; England |
| ADP, collagen and U44 619 (thromboxane A2 mimetic)-induced platelet aggregation using platelet‑adjusted plasma (2.5 × 108 platelets/l) | Platelet aggregation induced by ADP, compound U44619, and collagen were similar in both groups. |
6 | Suwannuruks et al47 | 80 participants:
No comorbidities; age, 18–50 y; Thailand |
| Platelet aggregation (ADP, collagen, and adrenaline) | No significant difference in platelet aggregation between the vegan, lacto‑vegetarian, lacto‑ovo‑vegetarians and omnivores |
Intervention | |||||
7 | Mezzano et al62; a 90‑day parallel study | 42 healthy men (mean age, 22 y):
Chile |
|
|
|
8 | Mann et al63; a 3 × 3‑week cross‑over study: 1‑week vegetarian run‑in followed by 2‑week meat (red, white or fish) consumption | 29 healthy participants (14 men, 15 women); age, 22–52 y | 3 × 3‑week interventions:
Week 1 = vegetarian diet followed by 2 weeks of either red meat (mean [SD], 351 [104] g/day, fat‑trimmed), white meat (mean [SD], 231 [52] g/day, fat‑trimmed), or fish (mean [SD], 133 [32] g/day, Atlantic salmon). This was followed by a 3‑week washout period.
During the next 2 cycles the meat sources (red, white or fish) were altered so all participants received all 3 treatments. |
|
|
9 | Makarewicz‑Wujec et al64; a 6‑month randomized, placebo‑controlled study (Dietary Intervention to Stop Coronary Atherosclerosis in Computed Tomography) | 81 participants with stable CAD:
|
| Plasma CXCL4 | The DASH diet decreased CXCL4 concentrations among patients with stable CAD. CXCL4 also correlated negatively with vegetable intake. |
10 | Yazici et al65; a 20‑week parallel study |
Participants did not exercise regularly. |
|
| Mean platelet volume was significantly decreased following the DASH and exercise intervention in the prehypertensive group, signifying decreased platelet activation. |
This lack of consistency in findings is not entirely surprising given the variation in platelet function outcomes measured (ex vivo platelet aggregation, thromboxane secretion, plasma microvesicle concentration), type and concentration of agonists used (adenosine diphosphate, collagen, epinephrine, arachidonic acid), and platelet concentration in the analyzed sample (whole blood, platelet‑rich plasma, platelet‑adjusted plasma). In addition, the dietary interventions considered to be plant‑based ranged from strictly vegan to diets containing occasional consumption of white meat and fish (DASH) and diets with high intakes of fatty fish such as the Nordic diet and, in the case of the Mediterranean diet, also containing moderate amounts of alcohol, particularly red wine. Different components of plant‑based diets have been reported to have varying effects on platelet function and inclusion / exclusion of these dietary components in the study diets will therefore differentially influence the outcome of the platelet function tests. A detailed discussion of the effects of these nutrients and foods on platelet function has been published in a number of reviews.11,12,66-74 While discussing the evidence for the individual nutrients and foods is outside the scope of this review, we aim to provide a broad overview of different components of plant‑based diets that may influence platelet function, highlighting the complexity of drawing conclusions regarding the effect of plant‑based diets on platelet function.
Foods and nutrients typically included in plant‑based diets such as dark chocolate, foods with a low glycemic index, garlic, ginger, onion, grapes (and juice), berries, tomato, vitamins, minerals, and phytochemicals (flavonoids and antioxidants) have all been shown to reduce platelet aggregation (reviewed by McEwen,67 Pieters and De Maat,11 Dutta‑Roy,69 Tubek et al,71 and Phang et al68). However, whether these changes are sufficient to alter thrombotic status is difficult to determine, as many of the micronutrients have limited bioavailability. The impact of alcohol (as the key component of the Mediterranean diet), on the other hand, is more complex and not yet fully elucidated, with a number of studies demonstrating inhibition of platelet activation, while evidence for enhanced platelet activation has also been reported (reviewed by Pieters and De Maat11).
Another important component of plant‑based diets is the type of fat consumed with typically proportionally higher intakes of monounsaturated fatty acids (olive oil) and varying ratios of n‑3 to n‑6 polyunsaturated fatty acids. Vegans have low intakes of long‑chain n‑3 polyunsaturated fatty acids while flexitarian / pescatarian diets, such as the Nordic diet, containing fatty fish, have a high content. The influence of monounsaturated fatty acids on platelet function remains unclear with several studies reporting inhibited platelet aggregation, others reporting no effect, and others even found increased aggregability (reviewed by Rajaram66 and Pieters and De Maat11). The effect of polyunsaturated fatty acids on platelet function is largely dependent on being either n‑3 or n‑6, with n‑3 inhibiting and n‑6 promoting platelet aggregation by competing for cyclooxygenase and lipoxygenase and in doing so, producing different eicosanoids (reviewed by Dutta‑Roy69). Compared with omnivores, vegetarians, especially vegans, have lower n‑3 polyunsaturated fatty acid levels in the platelet membrane phospholipids, which are associated with increased collagen and adenosine diphosphate–stimulated ex vivo blood platelet aggregation (reviewed by Li12). Fish consumers, on the other hand, have high n‑3 polyunsaturated fatty acid levels. Although the ability of fish oil to modulate platelet function by attenuating thromboxane A2 production is well known, supplementation studies did not consistently find inhibited platelet aggregation. A meta‑analysis of randomized controlled trials concluded that the supplementation of n‑3 polyunsaturated fatty acids was associated with a reduced platelet aggregation in individuals in poor health, but not in healthy individuals.70 This is in agreement with a recent review by Siniarski and Gajos75 that a degree of uncertainty still remains regarding the use of polyunsaturated fatty acids in the prevention of CVD since the initial promising findings from intervention studies were not supported by recent meta‑analyses and differences in the approach of seminal clinical trials resulted in divergent results. Furthermore, plant‑based n‑3 fatty acids were found to be less effective inhibitors of platelet aggregation than fish oils.76
Lastly, plant‑based diets are a source of dietary salicylic acid. It has previously been reported that vegetarians can have serum salicylic acid levels as high as patients taking 75 mg of aspirin a day.77 In fact, Janossy et al78 reported that a variety of plant foods can exert effects on platelet function comparable to those of prescription medicine and as such, dietary intake may need to be considered when prescribing antithrombotic (aspirin) treatment. This is in agreement with the recommendation by Aimo and De Caterina79 that aspirin treatment for primary prevention of CVD should be based on a tailored approach that considers the combined assessment of thromboembolic and bleeding risk, the patient’s general health, general preventive measures (that can include a plant‑based diet), and the patient’s 10‑year CVD risk.
Plant‑based diets and factor VII
Although there is some evidence for the effect of plant‑based diets on FVII, less information is available than for fibrinogen and platelets. We found 5 cross‑sectional studies of which 3 report decreased FVII (measured as FVII coagulant activity [FVIIc], FVII activity, and percentage) in vegans and lacto‑ovo‑vegetarians compared with omnivores43,49,50 and 2 report no differences (FVIIc)46,48 (Table 3). Two intervention studies,56,57 each with a duration of 2 weeks, investigating the Nordic diet, found lower FVIIc compared with the respective control diets while in one, no effect was observed for FVII antigen (FVIIag) or the FVIIc to FVIIag ratio.57 Diet‑related factors that have been associated with higher FVII include obesity (reviewed by Pieters and De Maat11) and consumption of saturated fatty acids, particularly C12–C1680,81 which tend to be lower in plant‑based consumers. The mechanism whereby dietary fat leads to FVII activation remains uncertain. Possible explanations include association with triglyceride‑rich lipoproteins, chylomicron size, serum phospholipid concentration, and the presence of procoagulant aminophospholipids as minor components of lipoproteins.82,83 Another novel proposal is that FVII activation follows the shift of pro‑coagulant phospholipids such as phosphatidylserine from the inner to the outer leaflet of cell‑surface membranes.84 Alcohol85 and fiber consumption,57,86 on the other hand, have been demonstrated to decrease FVII. According to a review by Lee and Lip,87 there is no consistent effect of n‑3 supplementation on FVII, with the majority of the studies finding no effect. Taken together, these data could suggest that the lower FVIIc observed in the studies employing the Nordic diet may not be the result of active lowering of FVII by the diet, but by higher levels in the control diets which were both high in fat. In agreement with this, none of vegetarian participants in any of the cross‑sectional studies listed above that reported lower FVII levels consumed fish, while 3 of the 5 studies reported the control groups to consume higher amounts of saturated fats,43,46,49 with one study50 not reporting fat intake. Lastly, the study by Mia and Vorster48 that found no difference in FVII between vegetarians and omnivores explicitly stated that there was no difference in total fat or fiber intake between the 2 groups.
No. | Author | Study population | Type of diet | Biomarker | Main results |
Abbreviations: FVIIact, factor VII activity; FVIIag, factor VII antigen; FVIIc, factor VII coagulant activity; SFA, saturated fatty acid; TE, total energy; others, see Table 1 | |||||
Cross‑sectional | |||||
1 | Mezzano et al43 | 54 participants with no comorbidities:
Chile |
| FVIIc | FVIIc was significantly lower in the vegetarian group compared with omnivores. |
2 | Pan et al46 | 114 participants with no comorbidities:
Age, 20–30 y; Chinese participants |
| FVIIc | No significant difference in FVIIc between vegetarians and omnivores. |
3 | Li et al49 | 139 healthy men; age, 20–50 y:
nonsmoking |
(Higher SFA intakes in meat‑eaters) | FVIIact
(ACL 200 system) | Vegans had a significantly lower FVIIact than meat‑eaters |
4 | Mia and Vorster48 | 321 Indian adolescents:
Age, 16–18 y; South Africa |
| FVIIc | FVIIc did not differ between the lacto‑ovo‑vegetarian and omnivore groups. The number of vegetarians in this study was small (10%) and the results therefore cannot be extrapolated to the general vegetarian population. |
5 | Haines et al50; controls were from the Northwick Park Heart Study | 332 non‑smokers, not using oral contraception; age, 18–65 y:
|
| FVII (%) | FVII was significantly lower in the vegetarians compared to the omnivores. |
Intervention | |||||
6 | Marckmann et al56; a randomized cross‑over study with intervention duration of 2 weeks and a 2‑to‑6‑week washout period | 20 healthy women; age, 21–52 y; BMI, 20–25 kg/m2 | 3 ad libitum experimental diets:
| FVIIc | Nonfasting FVIIc was significantly lower following the starch (Nordic) diet compared to the sucrose or fat diets, with nonfasting FVIIc levels also lower in the starch group; however, not significantly so. |
7 | Marckmann et al57; a randomized, crossover, 2‑week study | 21 healthy middle‑aged individuals:
5 light smokers; Denmark |
|
(one‑stage clotting assay)
|
|
Plant‑based diets and fibrinolysis
There were 11 studies that investigated the association between plant‑based diets and fibrinolysis, measured either as concentration or activity of individual proteins in the lytic pathway (activators and inhibitors) or making use of global assays (Table 4). Four of the 7 cross‑sectional studies found no difference in fibrinolytic markers between vegetarians (vegans and lacto‑ovo‑vegetarians) and omnivores.43,46,49,88 One reported higher fibrinolytic activity,42 one decreased fibrinolytic activity,50 and another lower plasminogen levels.43 One study reported a positive association between plasminogen activator inhibitor‑1 (PAI‑1) and a dietary pattern containing red meat, low‑fiber bread, and dairy.45 Regarding intervention studies, a study comparing a 4‑week DASH diet to a control diet higher in total and saturated fats and lower in fruit, vegetables, and low‑fat dairy, found the DASH diet to have no effect on any of the fibrinolytic markers analyzed.89 A 2‑week Nordic diet, compared with a high‑fat Danish diet, resulted in increased fibrinolytic activity (euglobulin lysis test) and increased tissue plasminogen activator activity but had no effect on PAI‑1.57 Two studies comparing an 8‑week American Heart Association diet90 and a 4‑week diet high in whole grains, nuts, legumes, and dairy91 with diets high in meat, both found PAI‑1 antigen to be higher in meat‑consumers. Kim et al91 additionally reported an inverse association between PAI‑1 and whole grain intake.
No. | Author | Study population | Type of diet | Biomarker | Main results |
Abbreviations: AHA, American Heart Association; EFA, euglobulin fibrinolytic activity; ELT, euglobulin lysis test; PAI‑1, plasminogen activator inhibitor‑1; PAI‑1ag, plasminogen activator inhibitor‑1 antigen; PAP, plasmin‑antiplasmin complex; tPA, tissue plasminogen activator; tPAact, tissue plasminogen activity; tPAag, tissue plasminogen activator antigen; others, see Table 2 | |||||
Cross‑sectional | |||||
1 | Famodu et al42; selection based on habitual intakes | 76 participants with no comorbidities; mean age, 48 y:
Nigeria |
|
|
|
2 | Mezzano et al43 | 54 participants with no comorbidities:
Chile |
|
|
|
3 | Pan et al46 | 114 Chinese participants with no comorbidities:
Age, 20–30 y |
| Plasminogen | No significant difference in plasminogen between vegetarians and omnivores. |
4 | Liese et al45; the Insulin Resistance Atherosclerosis Study | 880 middle‑aged adults, 144 with diabetes mellitus; age, 45–74 y; African American, Hispanic, and non‑Hispanic White participants; USA | Identification of food patterns associated with fibrinogen using reduced rank regression | PAI‑1ag (2‑site immunoassay sensitive to free active and latent PAI but not PAI‑1 complexed with tPA) | PAI‑1 had a positive association with the food pattern containing high intake of red meat, low‑fiber bread and cereal, dried beans, fried potatoes, tomato vegetables, eggs, cheese and cottage cheese and low intake of wine. |
5 | Ho and Chwang88 | 35 healthy participants:
|
(12 consumed milk, 14 consumed eggs)
|
Before and after venous occlusion test | There was no significant difference in tPAag, PAI‑1act or ELT before or after the venous occlusion test between the vegetarians and omnivores. |
6 | Li et al49 | 139 healthy men; age, 20–50 y:
|
| Plasminogen | Plasminogen did not differ significantly between the 4 dietary groups. |
7 | Haines et al50; controls were from the Northwick Park Heart Study | 332 non‑smokers, not using oral contraception; age, 18–65 y:
|
| Fibrinolytic activity (method of Fearnley and Chakrabarti expressed as the reciprocal of blood clot lysis time in hours × 100) | Fibrinolytic activity was significantly lower in vegetarian men than in omnivorous men. |
Intervention | |||||
8 | Kim et al91; randomized crossover study of two 4‑week interventions with a washout period of minimum 2 weeks (average, 3 weeks) | 51 (15 men, 36 women) participants without type 2 diabetes; mean age, 35.1 y; Australia / New Zealand |
Total energy was matched, and vegetables and fruit were limited to 1–2 servings in both diets. | PAI‑1ag |
|
9 | Lopez‑Learrea et al90; an 8‑week randomized, parallel trial (RESMENA: Metabolic Syndrome Reduction in Navarra) | 96 Caucasian participants (51 men, 45 women) with obesity and metabolic syndrome features; mean age, 50 y:
Spain |
| PAI‑1ag | PAI‑1ag was significantly reduced in the control‑diet, and only borderline significantly decreased in the RESEMNA (high protein) diet following the 8‑week intervention. |
10 | Erlinger et al89; a 4‑week parallel intervention | 55 hypertensive participants (35 African‑American, 20 Whites) taking no anti‑hypertensive medication / agreed to undergo supervised withdrawal of antihypertensive medication for 2 weeks prior to screening:
|
The DASH diet was lower in total and saturated fats and higher in fruit, vegetables and low‑fat dairy products.
Diets did not differ regarding sodium content (approximately 3 g/day). |
| The DASH diet did not affect any of the fibrinolytic markers. |
11 | Marckmann et al57; a 2‑week randomized, crossover study | 21 healthy middle‑aged individuals:
5 light smokers; Denmark |
|
|
|
The evidence for dietary factors that can improve fibrinolysis is limited and inconclusive. Nutrients and foods that have, thus far, received the most attention include alcohol, fats (monounsaturated fatty acids, n‑3 fatty acid supplementation), and a number of micronutrients such as vitamin C, D, and E, retinol, and zinc (reviewed by Lee and Lip87 and Pieters and De Maat11). For most of these, the number of investigations is limited, and the available evidence produced contradictory findings. Also, most of the studies investigated individual activators or inhibitors in the fibrinolytic pathway such as plasminogen, or tissue plasminogen activator or PAI‑1 activity or antigen as surrogate markers of fibrinolytic activity, without directly measuring fibrinolytic potential.
The evidence for dietary habits that can inhibit fibrinolysis is much stronger. Again, for individual nutrients and foods, the evidence is limited, but there is a strong relationship between consequences of overnutrition such as obesity and metabolic syndrome and decreased fibrinolytic potential and in particular increased PAI‑1. A major source of PAI‑1 is adipose tissue, with visceral fat producing more PAI‑1 than subcutaneous fat, since it produces more proinflammatory cytokines, which stimulates PAI‑1 secretion (being an acute‑phase protein) and it contains more stromal cells, which is the cellular component of adipose tissue that produces PAI‑1.92-94 The metabolic syndrome is characterized by abdominal obesity, as well as dyslipidemia, hypertension, and glucose intolerance (insulin resistance), all of which have been linked to increased PAI‑1.95,96 In fact, the relationship of PAI‑1 with metabolic syndrome is so strong, that it is considered by some to be a true component of the metabolic syndrome.97 In agreement with PAI‑1, global fibrinolytic assays have also demonstrated decreased lysis in both obesity and metabolic syndrome, confirming their hypofibrinolytic effects.98,99
Thus, while the evidence for the effect of individual components of plant‑based diets on fibrinolysis is still to be confirmed, the lower prevalence of obesity7 and metabolic syndrome in plant‑based consumers (reviewed by Babio et al100)supports a beneficial relationship between plant‑based diets and fibrinolytic potential.
Plant‑based diets and other hemostatic factors
The relationship between plant‑based diets and a number of other hemostatic variables have also been investigated and is summarized in Table 5, although the number of studies is small with varying results. Five cross‑sectional studies43,46,47,49,50 found no difference in some, but not all of the hemostatic variables measured between vegetarians (vegans and lacto‑ovo‑vegetarians) and omnivores, and 343,46,50 reported both lower levels of some and higher levels of other hemostatic variables in vegetarians. There was one intervention study of 90 days that reported longer bleeding times following a Mediterranean diet but no difference in von Willebrand factor levels compared with a high‑fat diet.62 The addition of wine did not significantly affect either outcome. Mezzano et al43 concluded that these findings may be related to the origin of the hemostatic factors since plasma levels of coagulation or fibrinolytic factors and inhibitors synthesized in the liver were lower in vegetarians than in omnivorous controls while those of predominantly extrahepatic origin were not. Much more research, in particular large intervention trials, is required to corroborate findings regarding the effect of plant‑based diets on these hemostatic variables, before firm conclusions can be drawn or recommendations to the public can be made.
No. | Author | Study population | Type of diet | Biomarker | Main results |
Abbreviations: APTT, activated partial thromboplastin clotting time; ATIII, antithrombin III; FII, factor II; FVc, factor V coagulant activity; FX, factor X; PT, prothrombin time; TAT, thrombin‑antithrombin complex; TT, thrombin time; vWF, von Willebrand factor; vWFag, von Willebrand factor antigen; others, see Tables 2 and 3 | |||||
Cross‑sectional | |||||
1 | Pan et al46 | 114 participants with no comorbidities:
Age, 20–30 y; Chinese participants |
|
|
|
2 | Mezzano et al43 | 54 participants with no comorbidities:
Chile |
|
|
|
3 | Haines et al50; controls were from the Northwick Park Heart Study | 332 non‑smokers, not using oral contraception; age, 18–65 y:
|
|
|
|
4 | Li et al49 | 139 healthy men; age, 20–50 y:
nonsmoking |
|
| No significant difference between the 4 dietary groups for PT, APTT or ATIII. |
5 | Suwannuruks et al47 | 80 participants:
No comorbidities; age, 18–50 y; Thailand |
|
| No significant difference in APTT, PT and TT between the vegetarians and omnivores. |
Intervention | |||||
6 | Mezzano et al62; a 90‑day intervention | 42 healthy men (mean age, 22 y):
Chile |
|
|
|
Conclusion
Healthy plant‑based diets have established benefits for cardiometabolic health, and they may do so, in part, through effects on thrombotic factors. However, this relationship is complex and depends on the energy, nutrient, and food composition of the diet. Strictly vegan diets, if not carefully planned and balanced may result in deficiencies (eg, n‑3 fatty acids and vitamin B12) that may have a negative impact on thrombosis. While some components of plant‑based diets (eg, fiber, phytochemicals, long‑chain n‑3 polyunsaturated fatty acids, moderate alcohol consumption) may actively decrease thrombotic factors, the limiting of prothrombotic components (eg, saturated fat and animal protein), present in typical omnivorous diets, may provide indirect benefit. In addition, healthy plant‑based diets, being comparatively hypo‑caloric (regardless of the composition), generally protect against overnutrition and its metabolic consequences such as obesity and metabolic syndrome, which are also considered prothrombotic. A one‑size‑fits‑all conclusion can therefore not be drawn as the potential antithrombotic effect of different plant‑based diets depends on the nutrient composition (based on the degree of exclusion of animal products), the content of active antithrombotic dietary components, the relative absence of prothrombotic dietary factors as well as the degree of total caloric restriction.
- Kahleova H, Becerra‑Tomas N, Blanco Mejia S, et al. Plant‑based eating and cardiometabolic health. Alpro Foundation; 2020.
- Orlich MJ, Singh PN, Sabaté J, et al. Vegetarian dietary patterns and mortality in Adventist Health Study 2. JAMA Intern Med. 2013; 173: 1230‑1238. | Crossref
- Crowe FL, Appleby PN, Travis RC, et al. Risk of hospitalization or death from ischemic heart disease among British vegetarians and nonvegetarians: results from the EPIC‑Oxford cohort study. Am J Clin Nutr. 2013; 97: 597‑603. | Crossref
- Kwok CS, Umar S, Myint PK, et al. Vegetarian diet, Seventh Day Adventists and risk of cardiovascular mortality: a systematic review and meta‑analysis. Int J Cardiol. 2014; 176: 680‑686. | Crossref
- Key TJ, Appleby PN, Rosell MS. Health effects of vegetarian and vegan diets. Proc Nutr Soc. 2006; 65: 35‑41. | Crossref
ARTICLE INFORMATION