Acute kidney injury (AKI) is a common complication in patients with COVID‑19 and affects 3% to 78% patients depending on the severity of infection. The pathogenesis of COVID‑19 AKI is multifactorial and includes indirect effects resulting from systemic viral infection and its treatment as well as direct mechanisms like glomerulopathy, endothelial dysfunction, complement activation, coagulopathy, potentially inducing the activation of the thrombotic microangiopathy (TMA) pathway.1,2 After kidney transplantation (KTx), the immune stimulation of alloantibodies production has also been postulated.3
We present a 41‑year‑old man 11 months after a second KTx, with end‑stage renal disease in the course of immunoglobulin (Ig) A nephropathy admitted to the transplantation center for the assessment of graft dysfunction. One month earlier, he had COVID‑19. He presented to a local hospital with pneumonia, diarrhea, anemia, a rise in creatinine level from 2.45 to 3.8 mg/dl (reference range, 0.73–1.18 mg/dl). The management included antibiotics and modification of immunosuppressive regimen (mycophenolate mofetil withdrawn, steroids increased, tacrolimus reduced).
Before COVID‑19, slow progression of graft failure (serum creatinine level rose from 1.65 mg/dl at the time of the first visit in the transplant outpatient clinic, to 2.45 mg/dl, one month before COVID‑19), non‑nephrotic proteinuria and erythrocyturia were observed. Tacrolimus trough levels were between 6.9 and 12.9 µg/l; 7.4 µg/l before COVID‑19. At that time, renal ultrasound did not show any abnormalities, BK virus infection was excluded.
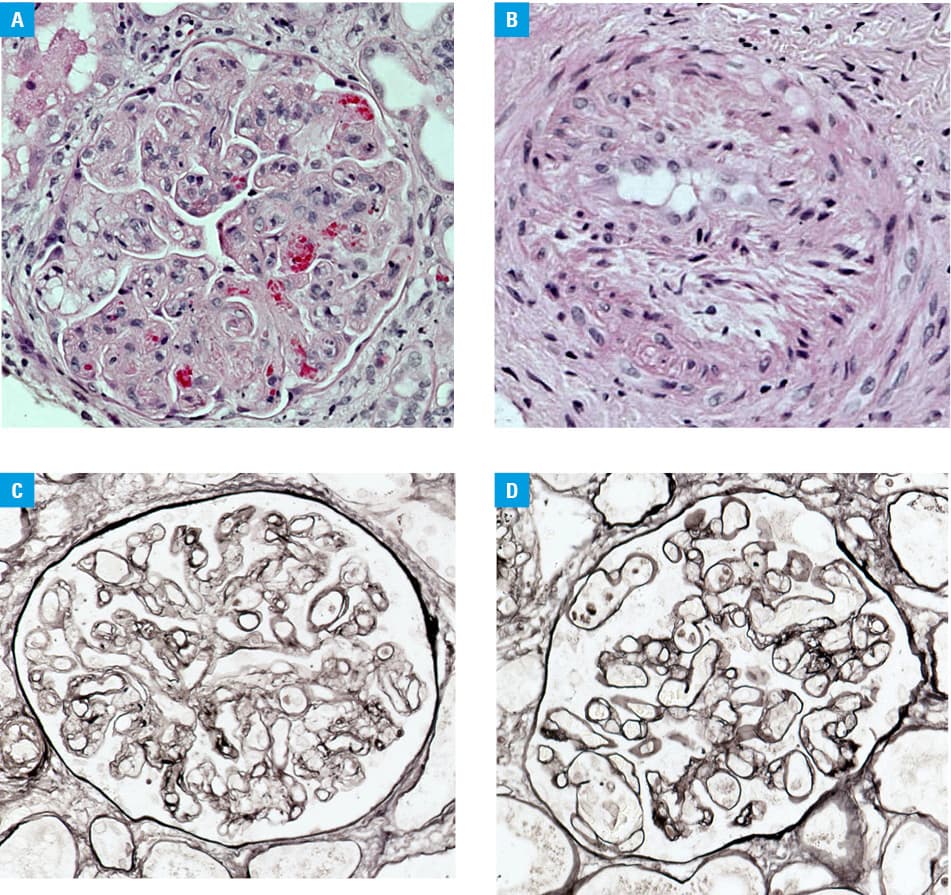
On admission to the transplantation center, the patient demonstrated recurrent diarrhea, volume overload, impaired graft function (serum creatinine, 3.67 mg/dl), uncontrolled hypertension and nephrotic proteinuria of 3520 mg/24 h (reference range <150 mg/24 h). A polymerase chain reaction test for SARS‑CoV‑2 was negative, chest X‑ray showed post‑COVID‑19 abnormalities, stool culture, stool polymerase chain reaction test and rectal swabs were negative. Cytomegalovirus, BK virus, hepatitis B virus, hepatitis C virus, and HIV infections were excluded. Mean tacrolimus trough levels were maintained below 6.0 µg/l. Diarrhea, overhydration, and hypertension resolved after symptomatic treatment. Kidney biopsy revealed acute TMA, chronic transplant glomerulopathy probably secondary to microangiopathy, proliferative arteriopathy, and signs of IgA nephropathy in the transplant. Acute tubular necrosis was present, no significant interstitial fibrosis and tubules atrophy, as well as no features of T‑cell rejection and polyoma virus nephropathy were found. Staining for C4d was negative (Figure 1A–1D). Some alterations in laboratory tests potentially related to TMA were noticed: decreased hemoglobin level (8.3 g/dl; reference range, 13–17 g/dl) and platelet count (115 G/l; reference range, 150–410 G/l), elevated schistiocytes count (38/1000 red blood cells; reference range <10/1000 red blood cells) and lactate dehydrogenase concentration (335 U/l; reference range, 125–220 U/l). ADAMTS‑13 activity was normal. The Coombs test and ADAMTS‑13 antibodies were negative. Donor‑specific antibodies were not found.
It was assumed that TMA might be associated with the history of COVID‑19. The treatment included transfusions of fresh frozen plasma and plasmapheresis. No improvement in renal function and proteinuria was achieved. Four months later, the patient started hemodialysis treatment, graftectomy of the first graft was performed, and he was qualified for retransplantation. Panel reactive antibodies were undetectable at the time of writing of this study.
Patients after KTx are especially vulnerable to crucial risk factors for COVID‑19 AKI and to unfavorable outcomes.1 The reported indications for kidney biopsy in COVID‑19 were, besides AKI, heavy proteinuria, and erythrocyturia, and the most frequent histopathological findings were acute tubular injury, collapsing type glomerulopathy, and TMA. TMA after KTx is predominantly induced by antibody‑mediated rejection, calcineurin and mammalian target of rapamycin inhibitors toxicity, viral infections, but ADAMTS‑13 deficiency, Shiga toxin–mediated injury, and recurrence of TMA should also be considered. In the presented case, absence of donor‑specific antibodies and no C4d deposits in biopsy raise doubts on antibody‑mediated rejection as the cause of TMA. Calcineurin inhibitor toxicity seems to be unlikely, as tacrolimus trough levels did not exceed recommended concentrations. Moreover, doses were reduced due to COVID‑19. No prominent interstitial fibrosis and tubular atrophy were present in biopsy specimens. The most common infections associated with TMA were also not confirmed. IgA nephropathy, as a known cause of end‑stage renal disease, as well as evidence of its recurrence in graft biopsy, are not consistent with recurrent TMA. Proteinuria, erytrocyturia, and deterioration of graft function before COVID‑19 seem to be related to IgA nephropathy recurrence.
There are few reports demonstrating TMA in native and transplanted kidneys in the course of COVID‑19, with variable but usually unfavorable outcomes.3-5 The outcome in our case was not satisfactory, probably due to delayed diagnosis. It suggests the need to be aware of renal manifestations in SARS‑CoV‑2 infection, including TMA in kidney transplant recipients.
- Nadim MK, Forni LG, Mehta RL, et al. COVID‑19‑associated acute kidney injury: consensus report of the 25th Acute Disease Quality Initiative (ADQI) Workgroup. Nat Rev Nephrol. 2020; 16: 747‑764. | Crossref
- Levi M, Thachil J. Coronavirus disease 2019 coagulopathy: disseminated intravascular coagulation and thrombotic microangiopathy‑either, neither, or both. Semin Thromb Hemost. 2020; 46: 781‑784. | Crossref
- Akilesh S, Nast CC, Yamashita M, et al. Multicenter clinicopathologic correlation of kidney biopsies performed in COVID‑19 patients presenting with acute kidney injury or proteinuria. Am J Kidney Dis. 2021; 77: 82‑93. | Crossref
- Jespersen Nizamic T, Huang Y, Alnimri M, et al. COVID‑19 manifesting as renal allograft dysfunction, acute pancreatitis, and thrombotic microangiopathy: a case report. Transplant Proc. 2021; 53: 1211‑1214. | Crossref
- Bascuñana A, Mijaylova A, Vega A, et al. Thrombotic microangiopathy in a kidney transplant patient with COVID‑19. Kidney Med. 2021; 3: 124‑127. | Crossref
ARTICLE INFORMATION