Ultrasound predictors of left adrenal metastasis in patients with lung cancer: a comparison of computed tomography, positron emission tomography–computed tomography, and endoscopic ultrasound using ultrasound bronchoscope
Key words: endoscopic ultrasound, left adrenal gland, lung cancer staging, positron emission tomography–computed tomography



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Ultrasound predictors of left adrenal metastasis in patients with lung cancer: a comparison of computed tomography, positron emission tomography–computed tomography, and endoscopic ultrasound using ultrasound bronchoscope
Introduction: Patients with resectable lung cancer require invasive evaluation of the enlarged left adrenal gland (LAG). Few studies showed the utility of endoscopic ultrasound using ultrasound bronchoscope (EUS‑B) in LAG assessment. Moreover, little is known on the combination of computed tomography (CT), positron emission tomography–computed tomography (PET‑CT), and EUS‑B for predicting left adrenal metastasis.
Patients and methods: In this retrospective cohort study performed from 2012 to 2019, patients with left adrenal enlargement were evaluated by CT, PET‑CT, and EUS‑B, followed by complete endoscopic mediastinal staging. The adrenal glands were sampled by EUS‑B–guided fine‑needle aspiration. Patients were followed for 6 months.
Results: During the staging of lung cancer in 2176 patients, 113 enlarged LAGs (5.19%) were biopsied. Malignancy was reported in 51 LAGs (45.13%). Endoscopic ultrasound upstaged 7 patients (6.2%) and downstaged 11 patients (9.37%) after false CT or PET‑CT findings. There were no biopsy‑related complications. Radiologic predictors of left adrenal metastases had the highest yield at the following cutoff points: Hounsfield units >23, standardized uptake value >4.2, and LAG size >25 mm. Hypoechogenic LAGs with loss of sea‑gull shape on EUS‑B were associated with a 28.67‑fold higher likelihood of metastases. The sensitivity, specificity, accuracy, negative predictive value, and positive predictive value for all ultrasound predictors were 86.21%, 85.45%, 85.84%, 85.45%, and 86.21%, respectively. When combined with radiologic features, the respective values were 93.10%, 94.55%, 93.81%, 92.86%, and 94.74%.
Conclusions: Hypoechogenicity and loss of sea‑gull shape on EUS‑B are the most reliable predictors of left adrenal metastasis. The combination of CT, PET‑CT, and EUS‑B improves the noninvasive diagnosis of left adrenal metastases in lung cancer patients.
What's new?
There are insufficient data on the diagnostic efficacy of endoscopic ultrasound combined with endobronchial ultrasound using ultrasound bronchoscope (EUS‑B) for left adrenal gland assessment in patients with lung cancer. Therefore, the technique is underused by pulmonologists. This study assessed ultrasound predictors of malignancy using EUS‑B alone and in combination with computed tomography and positron emission tomography–computed tomography in lung cancer patients with suspicion of left adrenal metastasis. The analysis of routine radiologic features showed that lung cancer can be overstaged if it is not evaluated by cytology. However, the risk of overstaging can be reduced when radiologic features are combined with proposed ultrasound predictors. Such an approach helps increase the accuracy and specificity of imaging tests and decide on whether to perform EUS‑B–guided fine‑needle aspiration of the enlarged adrenal gland. These findings may help design future studies on completely minimally invasive staging of lung cancer.
Introduction
The adrenal glands, liver, brain, and bones are predilection sites for lung cancer metastases. The presence of distant metastases (M1b/c category in the TNM classification) has a significant impact on prognosis and treatment.1 Different imaging techniques are currently used in routine clinical practice to assess the adrenal glands of patients with lung cancer, predominantly non–contrast‑enhanced computed tomography (CT), 18F‑fluorodeoxyglucose (18F‑FDG) positron emission tomography–computed tomography (PET‑CT), and, rarely, magnetic resonance imaging. A normal adrenal gland consists of a body (width ≤10 mm) and 2 limbs: a lateral limb and a medial limb (width ≤5 mm each). In patients with lung cancer, the incidence of adrenal metastases based on imaging studies ranges from 4.1% to 18%.2 Therefore, cytologic examination is critical, because metastatic involvement of the adrenal glands determines the most appropriate type of treatment, either a surgery or systemic oncological therapy.3 Conventional imaging techniques are not sensitive and specific enough to differentiate between benign and malignant lesions, with the rate of false‑positive and false‑negative CT results reaching 10%.4,5 Conventional CT, which measures the density of the adrenal glands in Hounsfield units (HUs), is helpful but not sufficient to exclude malignancy.5 On the other hand, PET‑CT has high sensitivity (94%) and specificity (85%) to diagnose distant metastasis to the adrenal glands in patients with lung cancer.6 However, the positive predictive values (PPVs) of CT and PET‑CT reach only up to 62% and 81%, respectively.7-9 Therefore, tissue biopsy is recommended, particularly to exclude metastatic spread and thus to avoid upstaging patients based on radiologic findings.10 Conventional CT‑guided adrenal biopsy has its own limitations, including a high rate of nondiagnostic samples (up to 14%) and complications (up to 12%).11,12 A conventional (ie, using a convex ultrasound gastroscope) endoscopic ultrasound–guided fine‑needle aspiration (EUS‑FNA) is a promising alternative to sample adrenal lesions, particularly in the left adrenal gland (LAG). The technique is relatively safe and has a high diagnostic yield because it is performed under real‑time ultrasound guidance.13-15 For the past decade, endobronchial ultrasound (EBUS) combined with endoscopic ultrasound using ultrasound bronchoscope (EUS‑B) has been the staging procedure of choice for the entire mediastinum.16-18 Nevertheless, only a few studies attempted to evaluate the diagnostic yield and safety profile of EUS‑B–guided fine‑needle aspiration (EUS‑B‑FNA) for the assessment of the LAG.19,20 Little is known on the utility of combined imaging modalities including CT, PET‑CT, and EUS‑B for adrenal assessment in patients with potentially resectable lung cancer. Moreover, there are not enough data on EUS‑B features that could be used to predict left adrenal metastasis. Considering these gaps in knowledge, we decided to evaluate the usefulness of malignancy predictors obtained by noninvasive techniques (CT, PET‑CT, and EUS‑B). On the basis of literature data and own experience, we aimed to determine whether any combination of these noninvasive tests could be sensitive and specific enough to predict left adrenal metastasis and avoid needle biopsy in patients with lung cancer.
Patients and methods
This retrospective cohort study was conducted in Pulmonary Hospital in Zakopane, Poland, and the Department of Thoracic Surgery of Medical University of Silesia in Katowice, Poland. The records of patients with either confirmed lung cancer or highly suspected for lung cancer who underwent complete endosonographic staging were assessed. Only patients with confirmed lung cancer who underwent complete endosonographic staging were included in the study. The LAG was assessed to investigate the correlation between HU on CT scans, standardized uptake value (SUV) on PET‑CT, and EUS‑B features. In our institutions, the combined use of EBUS and EUS‑B techniques has been a routine practice for cancer staging according to the TNM classification since 2012. The LAGs suspected of malignancy on radiologic imaging and EUS‑B were defined as those with a body short axis of more than 15 mm in width or with one of the limbs of more than 10 mm in width, with absence of a normal sea‑gull shape, regardless of echogenicity. These LAGs were punctured using real‑time EUS‑B by a transgastric approach. The diagnostic yield of the 3 predictors of left adrenal metastasis obtained by EUS‑B, namely, the loss of sea‑gull shape, hypoechogenicity, and inhomogeneity, was examined by calculating the sensitivity, specificity, accuracy, negative predictive value (NPV), and PPV for each predictor separately and for all the predictors combined. Hypoechogenicity was defined as the presence of hypoechogenic areas (in comparison with normal echogenicity) within the adrenal limb and / or body. The loss of normal sea‑gull shape was defined as an increase in the dimensions of the body and limb short axis above 15 mm and 10 mm, respectively, or the presence of additional adrenal masses. We also assessed the diagnostic yield of radiologic (CT and PET‑CT) predictors of left adrenal metastasis for the currently used and proposed cutoff points. Finally, we measured the diagnostic yield of the combination of ultrasound and radiologic predictors.
All endosonographic procedures were done in 2 bronchoscopy departments by 4 experienced chest physicians, who were specifically trained in EBUS and EUS‑B. The procedures were performed following the standard protocols. After providing informed consent, patients underwent EUS‑B in one session under mild conscious sedation with the use of intravenous midazolam (2–5 mg) and fentanyl (0.025–0.1 mg). Intravenous propofol (40–100 mg) was added if necessary. All EUS‑B‑FNA and EBUS‑guided transbronchial needle aspiration procedures were performed in the supine position. Flexible videobronchoscopes with an integrated convex ultrasound probe (BF‑UC160F‑OL8 and BF‑UC180F Olympus Medical Systems Corporation, Tokyo, Japan), which can visualize not only the mediastinal and hilar structures but also the LAG, were used for all EBUS and EUS‑B procedures. Dedicated ultrasound processors (EU‑ME1/2, Olympus Medical Systems Corporation and Aloka α7, Hitachi, Japan) with Doppler flow imaging to detect blood vessels and real‑time ultrasound guidance to obtain biopsy samples were used. The cytological 22‑gauge 40‑mm needles with 20‑ml syringes (NA‑201SX‑40/22, Olympus Medical Systems Corporation) were used for all biopsies. In each patient, 2 to 5 transgastric biopsy samples were obtained in one session.
Specimens were prepared as at least 2 to 5 smears in alcohol solution and cell blocks fixed in cytospin collection fluid or 10% buffered formalin and were then sent to the pathology department. On‑site cytopathology was not performed in any case. Standard staining with hematoxylin and eosin was used for all specimens, while immunochemistry and molecular testing were performed if necessary. All slides were examined by 2 experienced cytopathologists.
All patients who underwent the biopsy procedure were followed for at least 6 months. The lack of adrenal involvement was diagnosed if the biopsy was negative and follow‑up CT scans did not show adrenal enlargement. On the other hand, if the biopsy was positive or the LAG was enlarged on follow‑up CT scans, patients were considered positive for LAG involvement.
Ethics approval
The study protocol was approved by the regional bioethics committee (no. OIL/KBL/22/2017). All patients provided consent to undergo the study procedures. The study was conducted in accordance with the Declaration of Helsinki.
Statistical analysis
The sensitivity, specificity, accuracy, PPV, and NPV (including 95% CI) were calculated using the MedCalc statistical software (MedCalc Software Ltd, Ostend, Belgium). The receiver operating characteristic curves and the optimal cutoff points according to the Youden index were calculated using Statistica v13 (StatSoft Polska Sp. z o.o., Kraków, Poland). The significance level was set at a P value of less than 0.05.
Results
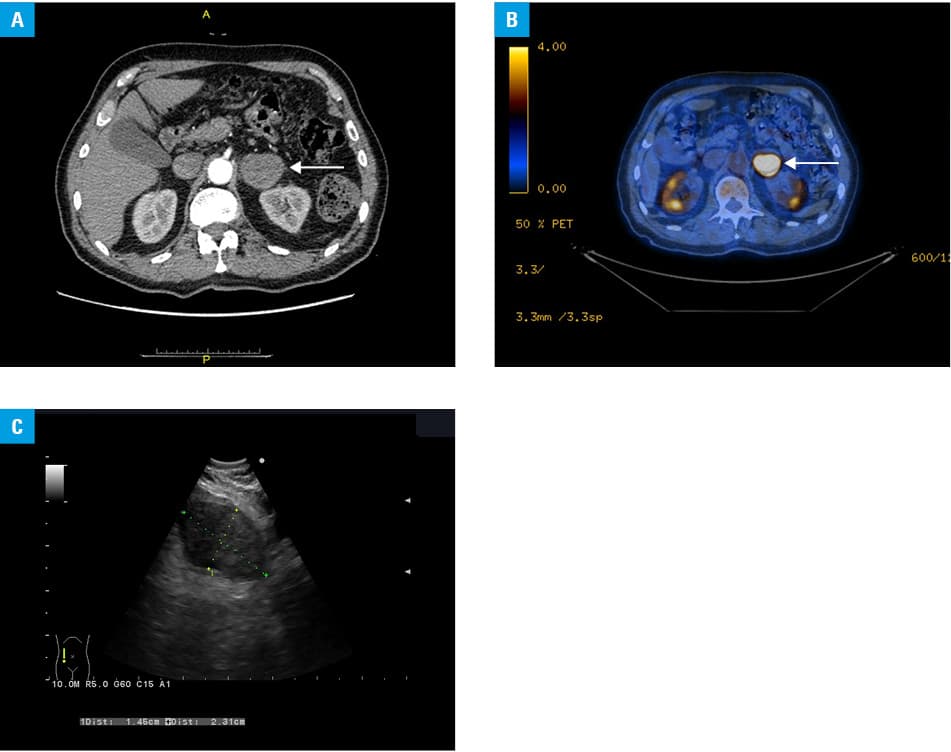
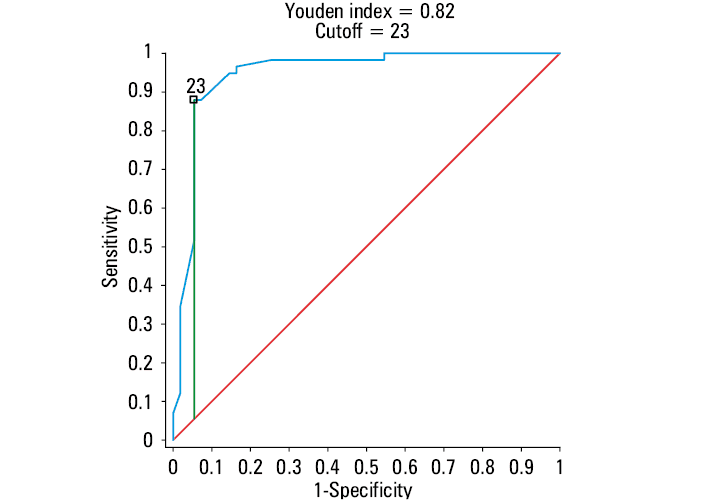
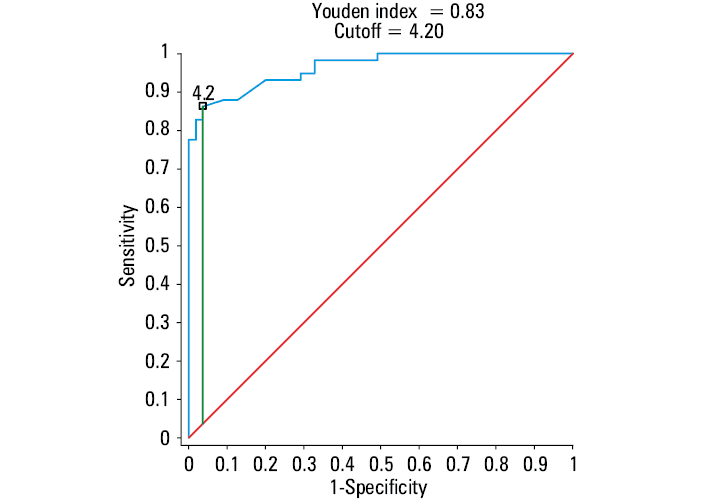
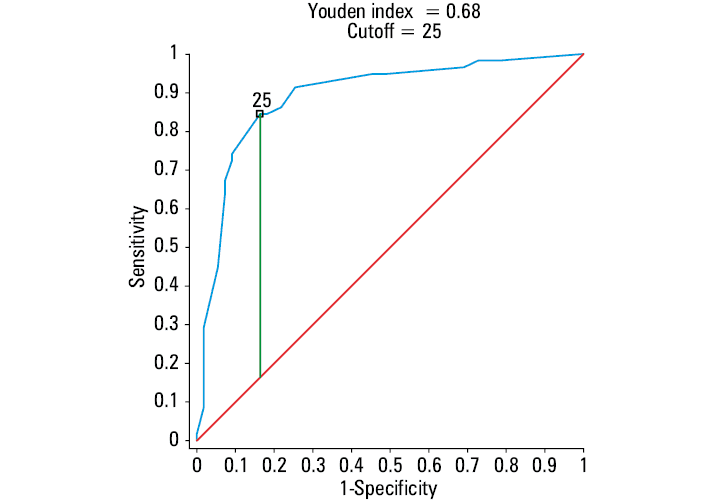
From 2012 to 2019, 2176 patients with lung cancer potentially eligible for lung resection were staged by the complete endosonographic approach combining EBUS and EUS‑B. The enlargement of the LAG was noted in 113 patients (5.19%), including 65 men and 48 women (mean [SD] age, 65.1 [7] years). All patients were diagnosed by combined endoscopic techniques and had histologically confirmed primary lung cancer. In particular, adenocarcinoma was diagnosed in 53 patients (46.9%); squamous cell carcinoma, in 30 (26.5%); small cell lung cancer, in 17 (15.1%); non–small cell lung cancer, in 6 (5.3%); non–small cell lung cancer (no otherwise specified) in 5 (4.4%); and large cell carcinoma, in 2 patients (1.8%). Adrenal involvement based on positive EUS‑B‑FNA findings was noted in 58 of the 113 patients (51.33%; 95% CI, 41.74%–60.84%). In 7 cases (6.2%), it was confirmed by LAG enlargement during follow‑up. A benign adrenal adenoma was confirmed by EUS‑B‑FNA in 55 of the 113 patients (48.67%), and the follow‑up did not reveal malignancy. Examples of left adrenal metastasis on CT, PET‑CT, and EUS‑B are shown in Figures 1A, 1B, and 1C, respectively. None of the patients developed any severe complications after biopsy. Endoscopic ultrasound resulted in upstaging of lung cancer in 7 patients (6.2%) after negative CT or PET‑CT findings, while it downstaged the cancer in 11 patients (9.37%) after positive CT or PET‑CT findings for left adrenal metastases. The specificity, PPV, and accuracy of radiologic predictors for left adrenal metastases were quite low at a HU cutoff higher than 10 based on the results of non–contrast‑enhanced CT, a SUV cutoff higher than 2.5 based on PET‑CT, and the transverse diameter of the LAG higher than 15 mm (Table 1). The diagnostic yield of the proposed radiologic predictors of left adrenal metastases calculated with the cutoff points based on the Youden index for the receiver operating characteristic curves is presented in Table 2. The following cutoff points were determined: HUs higher than 23 for CT (Figure 2), SUV higher than 4.2 for PET‑CT (Figure 3), and LAG size exceeding 25 mm in diameter (Figure 4). The ultrasound predictors of left adrenal metastases based on EUS‑B features, namely, hypoechogenicity, inhomogeneity, and the loss of sea‑gull shape were associated with higher odds of adrenal metastases by 28.67 (95% CI, 9.63–85.36; P <0.001), 7.37 (95% CI, 2.85–19.05; P <0.001), and 28.67 (95% CI, 9.63–85.36; P <0.001), respectively. The diagnostic yield of these ultrasound predictors is presented in Table 3, while the diagnostic yield of the combined radiologic and ultrasound predictors is presented in Table 4.
Parameter | LAG size (>15 mm) on CT | CT (HU >10) | PET‑CT (SUV >2.5) | |||
Value | 95% CI | Value | 95% CI | Value | 95% CI | |
Abbreviations: CT, computed tomography; HU, Hounsfield unit; LAG, left adrenal gland; NLR, negative likelihood ratio; NPV, negative predictive value; PET‑CT, positron emission tomography–computed tomography; PLR, positive likelihood ratio; PPV, positive predictive value; SUV, standardized uptake value | ||||||
Sensitivity, % | 96.55 | 88.09–99.58 | 98.28 | 90.76–99.96 | 96.61 | 88.29–99.59 |
Specificity, % | 30.91 | 19.14–44.81 | 61.82 | 47.73–74.59 | 67.27 | 53.29–79.32 |
Accuracy, % | 64.60 | 55.05–73.37 | 80.53 | 72.02–87.38 | 82.46 | 74.21–88.94 |
PLR | 1.40 | 1.16–1.68 | 2.57 | 1.84–3.61 | 2.95 | 2.01–4.32 |
NLR | 0.11 | 0.03–0.46 | 0.03 | 0.00–0.20 | 0.05 | 0.01–0.20 |
PPV, % | 59.57 | 55.09–63.90 | 73.08 | 65.94–79.19 | 76.00 | 68.37–82.27 |
NPV, % | 89.47 | 67.31–97.23 | 97.14 | 82.81–99.58 | 94.87 | 82.39–98.65 |
Parameter | LAG size (>25 mm) on CT | CT (HU >23) | PET (SUV >4.2) | |||
Value | 95% CI | Value | 95% CI | Value | 95% CI | |
Abbreviations: see Table 1 | ||||||
Sensitivity, % | 83.33 | 70.71–92.08 | 87.93 | 76.70–95.01 | 86.21 | 74.62–93.85 |
Specificity, % | 83.64 | 71.20–92.23 | 94.55 | 84.88–98.86 | 96.36 | 87.47–99.56 |
Accuracy, % | 83.49 | 75.16–89.91 | 91.15 | 84.33–95.67 | 91.15 | 84.33–95.67 |
PLR | 5.09 | 2.77–9.37 | 16.12 | 5.34–48.64 | 23.71 | 6.06–92.77 |
NLR | 0.20 | 0.11–0.37 | 0.13 | 0.06–0.26 | 0.14 | 0.08–0.27 |
PPV, % | 83.33 | 73.11–90.19 | 94.44 | 84.93–98.09 | 96.15 | 86.47–98.99 |
NPV, % | 83.64 | 73.57–90.37 | 88.14 | 78.71–93.72 | 86.89 | 77.65–92.66 |
Parameter | Loss of sea‑gull shape | Hypoechogenicity | Inhomogeneity | All ultrasound predictors | ||||
Value | 95% CI | Value | 95% CI | Value | 95% CI | Value | 95% CI | |
Abbreviations: see Table 1 | ||||||||
Sensitivity, % | 74.14 | 60.96–84.74 | 74.14 | 60.96–84.74 | 50.00 | 36.58–63.42 | 86.21 | 74.62–93.85 |
Specificity, % | 90.91 | 80.05–96.98 | 90.91 | 80.05–96.98 | 87.27 | 75.52–94.73 | 85.45 | 73.34–93.50 |
Accuracy, % | 82.30 | 74.00–88.84 | 82.30 | 74.00–88.84 | 68.14 | 58.71–76.59 | 85.84 | 78.03–91.68 |
PLR | 8.16 | 3.49–19.07 | 8.16 | 3.49–19.07 | 3.93 | 1.88–8.22 | 5.93 | 3.10–11.34 |
NLR | 0.28 | 0.18–0.44 | 0.28 | 0.18–0.44 | 0.57 | 0.43–0.76 | 0.16 | 0.08–0.31 |
PPV, % | 89.58 | 78.62–95.26 | 89.58 | 78.62–95.26 | 80.56 | 66.44–89.66 | 86.21 | 76.56–92.28 |
NPV, % | 76.92 | 68.14–83.86 | 76.92 | 68.14–83.86 | 62.34 | 55.66–68.58 | 85.45 | 75.36–91.86 |
Imaging method | Sensitivity,% | Specificity, % | Accuracy, % | NPV, % | PPV, % |
Abbreviations: EUS‑B, endoscopic ultrasound using ultrasound bronchoscope; others, see Table 1 | |||||
CT + PET‑CT (current cutoff points) | 93.10 | 81.82 | 87.67 | 91.84 | 84.38 |
CT + PET‑CT (proposed cutoff points) | 94.83 | 92.73 | 93.81 | 94.44 | 93.22 |
CT + PET‑CT + EUS‑B (current cutoff points) | 82.76 | 92.73 | 87.61 | 83.61 | 92.31 |
CT + PET‑CT + EUS‑B
(proposed cutoff points) | 93.10 | 94.55 | 93.81 | 92.86 | 94.74 |
Discussion
A radiologic assessment of distant metastases, including metastases to the adrenal glands, has become a noninvasive standard for lung cancer staging. A non–contrast‑enhanced CT, which describes the density of the adrenal glands in HUs, is helpful but insufficient to exclude malignancy.5 Three‑phase CT is much more effective in adrenal assessment, but it is not routinely performed in most patients undergoing staging for lung cancer. Because the diagnostic yield of radiologic techniques is relatively low, it is still necessary to obtain tissue confirmation. Eloubeidi et al15 assessed the correlation between the size of the adrenal glands and the risk of malignancy. Although the adrenal glands with a malignant lesion were more likely to be larger than 3 cm, the accuracy of EUS to differentiate them from benign lesions was 68%. Our study confirmed that malignant lesions cannot be differentiated from benign ones only on the basis of their size on CT and EUS‑B, because the specificity and accuracy are too low at the LAG size of more than 15 mm (30.9% and 64.6%, respectively). Only at the LAG size of more than 25 mm, the specificity and accuracy improve to 83.9% and 83.49%, respectively. Porte et al11 reported the rate of false‑positive results for malignancy of 21% and the rate of false‑negative results of 11% based on CT features alone. Our data also showed that CT results become more reliable if the HU cutoff point is higher than 23. This results in improved specificity and accuracy from 61.82% and 80.53% to 94.55% and 91.15%, respectively. With advancement in technology, PET‑CT may seem a reliable noninvasive option to evaluate adrenal lesions. The correlation between 18FDG‑PET and EUS‑FNA results was assessed by Schuurbiers et al.8 Of the 46 patients referred for EUS‑FNA based on the positive results of 18FDG‑PET, malignancy was confirmed in 32 (70%). The PPV of 18FDG‑PET was 74%.8 Similarly, in a study by Erasmus et al,21 the specificity of PET to detect malignancy in patients with lung cancer and adrenal lesions was 80%. In their review article, Stone et al6 reported a high sensitivity of PET‑CT (94%), but since specificity was lower than 90%, tissue confirmation was recommended.6 These findings are in line with our study, which showed high sensitivity ranging from 86.21% to 96.61%, while specificity depended on the SUV cutoff points and ranged from 67.27% for a cutoff higher than 2.5 to 96.36% for a cutoff higher than 4.2. In the group of lung cancer patients with left adrenal enlargement, the prevalence of metastases was 51.33%, which is comparable to data reported by Crombag et al.20 Patil et al22 reviewed 11 studies and noted that although the majority of adrenal lesions described as hypoechogenic were more suspicious for malignancy, this was not supported by cytologic outcome. A study by Darwiche et al23 confirmed that the visualization of the LAG with an EBUS scope is feasible, safe, and reliable in cases with or without a previous suspicion of malignancy. The 3 learning curves presented in their study support our opinion that EUS‑B has a potential for a much wider application in chest medicine.23 Of note, recently, a new type of biopsy needles (so called core needles) dedicated for EBUS scopes have become available. They have a modified tip in order to obtain a cytological biopsy of better quality. This is important especially in patients with advanced lung cancer because proper immunochemistry and molecular analysis allows targeted chemotherapy and / or immunotherapy.24 In our study, we directly compared CT, PET‑CT, and EUS‑B features such as left adrenal enlargement, loss of sea‑gull shape, and echogenicity to develop the new imaging model for predicting left adrenal metastases. Hypoechogenicity and the loss of sea‑gull shape were associated with 28.67‑fold higher odds of adrenal metastasis. The diagnostic yield of the combination of all 3 ultrasound features for predicting malignancy was higher than 85%. These findings suggest that if the adrenal glands are enlarged but show normal echogenicity and sea‑gull shape, the puncture can be avoided. In our study, we also confirmed the reliability of CT and 18F‑FDG PET‑CT for detecting adrenal malignancy, but mainly in the case of higher cutoff points (HU >23 and SUV >4.2). This suggests that combined endoscopic ultrasound using EUS‑B for lung cancer staging should be performed regardless of CT and PET‑CT findings. This combination improves the specificity to 94.55% and the PPV to 92.86% compared with radiologic imaging alone.
Our study is limited mainly by its retrospective design with a possible selection bias. Not all patients with left adrenal enlargement on CT underwent PET‑CT; therefore, it was not always possible to compare all noninvasive methods directly. It is unclear why PET‑CT was not performed in some cases. Perhaps it was unavailable, which would result in lower bias than in the case it was skipped intentionally despite CT findings strongly suggesting left adrenal metastasis. Moreover, in most cases, surgical biopsy to confirm malignancy was unavailable, which is the major limitation of our study and was reported also by others.13 This is consistent with most studies of EUS, in which cytology is considered a reference standard to determine malignancy mainly because of advanced disease stage. There was also no surgical pathology confirmation of benign lesions. The lack of histopathological assessment can lead to bias if all negative biopsies were considered as true negatives. However, we believe that this was minimized by the careful analysis of the medical history and the minimum radiologic follow‑up of 6 months.
In conclusion, our study showed that the hypoechogenicity and loss of sea‑gull shape on EUS‑B are the most reliable predictors of malignancy in patients with left adrenal enlargement. A combination of radiologic assessment based on CT and PET‑CT with EUS‑B findings improves the noninvasive diagnosis of left adrenal metastases in patients with lung cancer.
- Riihimaki M, Hemminki A, Fallah M, et al. Metastatic sites and survival in lung cancer. Lung Cancer. 2014; 86: 78‑84. | Crossref
- Silvestri GA, Tanoue LT, Margolis ML, et al. The noninvasive staging of non‑small cell lung cancer: the guidelines. Chest. 2003; 123: 147S‑156S. | Crossref
- Chapman GS, Kumar D, Redmond J 3rd, et al. Upper abdominal computerized tomography scanning in staging non‑small cell lung carcinoma. Cancer. 1984; 54: 1541‑1543. | Crossref
- Bodtger U, Vilmann P, Clementsen P, et al. Clinical impact of endoscopic ultrasound‑fine needle aspiration of left adrenal masses in established or suspected lung cancer. J Thorac Oncol. 2009; 4: 1485‑1489. | Crossref
- Boland GW, Lee MJ, Gazelle GS, et al. Characterization of adrenal masses using unenhanced CT: an analysis of the CT literature. AJR Am J Roentgenol. 1998; 171: 201‑204. | Crossref
ARTICLE INFORMATION