Patterns of multimorbidity in 4588 older adults: implications for a nongeriatrician specialist
Key words: multimorbidity, older adults, population study



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Patterns of multimorbidity in 4588 older adults: implications for a nongeriatrician specialist
Introduction: Multimorbidity has been recognized as an important factor in geriatric medicine. However, its importance for other specialists is still to be fully appreciated.
Objectives: The aim of the study was to assess the prevalence and patterns of multimorbidity in older patients drawn from the general population.
Patients and methods: The PolSenior was a nationwide, multicenter, cross‑sectional survey of aged population in Poland. Questionnaire, physical examination, and laboratory data were gathered. Multimorbidity was defined as a coexistence of 2 and more chronic diseases or medical problems out of 17 identified. Factor analysis was employed to identify clusters of conditions.
Results: Of 4588 patients, 51.9% were men; 640 were aged 55 to 59 years; 3948, ≥65 years; and 1757, ≥80 years. Multimorbidity depended on age and sex, and was diagnosed in 70.9% of those aged 55 to 59 years, 88.4% of those aged 65 to 79 years, and 93.9% of those aged ≥80 years. Only 8.5% of participants aged 55 to 59, 2.2% aged 65 to 79 years, and 0.9% aged ≥80 years had no diagnosis of chronic disease. Hypertension, metabolic diseases, and obesity predominated in those aged 55 to 59 and 65 to 79 years, whereas hypertension, eye disorders, and cognitive impairment prevailed in the oldest group. The highest likelihood of multimorbidity was found in the youngest participants who had stroke, kidney disease, cancer, or a composite of Parkinson disease / epilepsy; in 65‑to‑79‑year‑olds with a history of stroke; and in ≥80‑year‑olds with a history of stroke or heart failure.
Conclusions: The age‑specific analysis of clustering revealed differences in prevalence and patterns of comorbidities, which stresses the importance of individual approach to older patients.
What's new?
We demonstrate patterns of multimorbidity in 4588 older adults drawn from the general population. Cardiovascular disease strongly clusters with other chronic disease states, and prevalence of single cardiovascular disease involvement decreases sharply with age. This means that the physician caring for the older patient will need to take into account concomitant presence of other diseases, which would likely influence the diagnosis, treatment, and outcome of the index cardiovascular disease. We present a pictorial shorthand representation of possible multimorbidity patterns for the use by the “organ specialist,” as a reminder of possible conditions that may have clustered with a given cardiovascular problem in a given patient.
Introduction
The populations worldwide are ageing. The majority of older patients are affected by cardiovascular disease or other conditions. This often leads them to the nongeriatrician specialist’s consultation room, and in many a case means long‑term follow‑up by a specialist.1 However, due to an increased propensity toward chronic disease, older persons are frequently diagnosed with multimorbidity, which has been recognized as an important public health issue.2-4
Multimorbidity is defined as a coexistence of 2 or more diseases in an individual.5,6 Disease‑centered approach, as opposed to patient‑centered one, to the multimorbid individual may lead to medication errors, and in consequence, potentially avoidable health‑related adverse events including unnecessary hospitalization and death, as well as unnecessary expenditure on medical care.2,7-10 Currently, the awareness of the issues related to multimorbidity in “organ specialists” seems to be far from optimal.1 In our study, we seek the patterns that the multimorbidity may assume. The appreciation of such patterns may result in a better allocation of resources, avoidance of under and overtreatment, and avoidance of negligence of particular conditions, potentially hidden behind forefront diagnoses in the given patient.1,2
Patients and methods
Study design and participants
The PolSenior was a nationwide, multicenter, cross‑sectional survey, which aimed to assess medical, psychological, economic, and social aspects of ageing in Poland. The protocol of the survey has been described in detail elsewhere.11 Briefly, the study was conducted between 2007 and 2011. The participants had been randomly selected, with the proportional sex, age, and place‑of‑residence group stratified selection method. We included patients aged 55 to 59 years and 65 years or older.11 The study protocol was approved by the local ethics committee. Each patient gave an informed consent to participate in the study. Of the 5695 participants initially enrolled, we included data of 4588 (80.6%; 3948 aged ≥65 years and 640 aged 55–59 years). Those with missing data for at least one of the pre‑specified 17 morbidities or conditions used in the analysis were excluded from this study (for reasons of exclusions, see Supplementary material, Figure S1).
For the purpose of the present analysis, the participants were divided into 3 age subgroups: 55 to 59 years (n = 640), 65 to 79 years (n = 2191), and ≥80 years (n = 1757).
Assessment of multimorbidity
We obtained data about the following diagnoses and health‑related problems: hypertension, metabolic diseases, obesity, psychiatric disorders, arrhythmia, thyroid disease, respiratory disease, ischemic heart disease, osteoporosis, eye disorders, heart failure, anemia, cognitive impairment, chronic kidney disease, cancer, Parkinson disease / epilepsy, stroke.
The diagnoses were based on the medical questionnaire including history of hospitalizations, elements of geriatric assessment, diagnoses by caring physicians, laboratory results, anthropometric measurements, and in the case of hypertension, blood pressure measurements and the use of antihypertensive medications.
In the part of the diagnostic workup, which was based on laboratory or technical assessment, we used the following respective cutoff values. Hypertension was defined as the average of 2 latter of 3 consecutive readings of sitting blood pressure taken by a trained nurse of more than 139/89 mm Hg. Diabetes mellitus was defined as fasting plasma glucose level of 100 mg/dl or greater; obesity, as body mass index (BMI) of 30 kg/m2 or greater; thyroid disease, as thyroid‑stimulating hormone levels of less than 0.2 mIU/l or more than 4.5 mIU/l; impaired kidney function, as estimated glomerular filtration rate of less than 60 ml/min/1.73 m2, calculated according to the Chronic Kidney Disease Epidemiology Collaboration equation; anemia, as hemoglobin level of less than 130 g/l for men and less than 120 g/l for women. A psychiatric disease was recognized if a participant confirmed that she / he has ever been diagnosed with depression or any psychiatric disease or depressiveness was suspected on the basis of the result of mood screening assessment with the Geriatric Depression Scale (GDS) of 6 points or more. Cognitive impairment was suspected if the Mini‑Mental State Examination result was less than 24 points.
Multimorbidity was defined as a coexistence of 2 or more chronic diseases or health‑related problems.5,12
Statistical analysis
The database management and the statistical analysis were performed with the STATA 12 software (StataCorp LLC, College Station, Texas, United States). Means were compared with standard normal Z test, and the frequencies with the χ2 test. The analyses were weighted by sex and age to match the current structure of the Polish population.
We employed logistic regression models to evaluate the odds ratios of concurrent presence of 2 or more diagnoses, with and without adjustment for sex and age. To analyze the patterns of coexistence of diagnoses contributing to multimorbidity, we performed the factor analysis separately in the 3 specified age groups. The factor is defined as a group of diseases and conditions sharing possible common unknown feature responsible for their clustering. The number of factors in each age group was determined based on the amount of explained variability, and by inspection of scree plots. We performed an iterated principal factor analysis with the tetrachoric correlation. We applied the orthogonal Varimax rotation to obtain factors that were uncorrelated. In order to obtain clinically usable multimorbidity patterns, in each factor (cluster), we only present conditions with correlation coefficients exceeding 0.3.
Results
Group characteristics
A total of 4588 participants (men, 51.9%) were included in the present analysis. Of them, 1757 (38.3%; men, 55.2%) were at least 80 years of age with a mean (SD) age of 86.5 (4.6) years, 2191 (47.8%; men, 51.0%) were aged 65 to 79 years with a mean (SD) age of 72.0 (4.1) years, and 640 (13.9%; men, 45.6%) were aged 55 to 59 years with a mean (SD) age of 57.1 (1.4) years.
Prevalence of multimorbidity
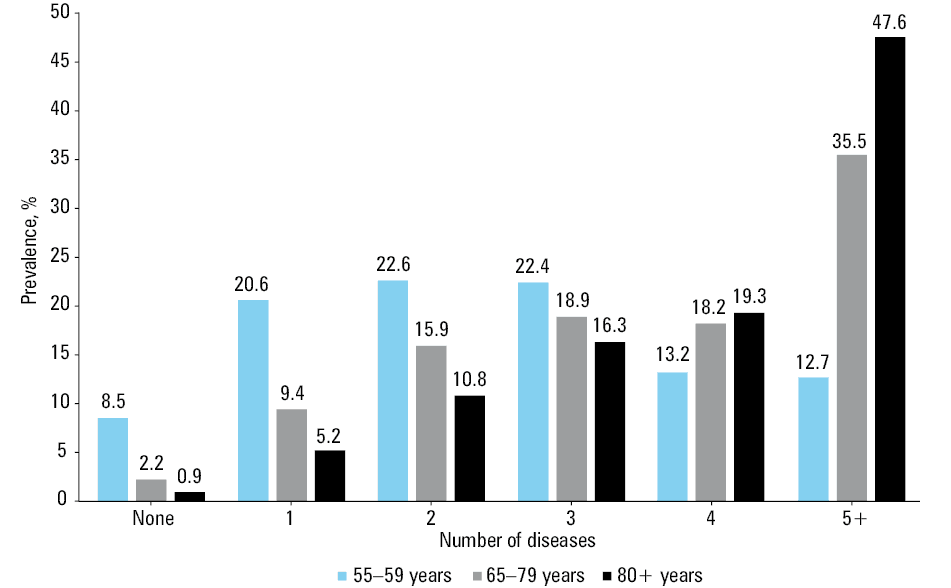
Multimorbidity was identified in 70.9% of participants aged 55 to 59 years, 88.4% of those aged 65 to 79 years, and in 93.9% of those aged 80 years and older (P <0.05) (Figure 1).
The odds of multimorbidity were higher in participants aged 65 to 79 years and those aged 80 years and older, respectively, when compared with the youngest respondents (OR, 2.94; 95% CI, 2.38–3.64, and OR, 5.5; 95% CI, 4.27–7.07, respectively; P <0.001).
The accretion of diseases across age groups is presented in Figure 1. In the youngest age stratum, 20.6% were affected with a single disease, 22.6% with 2, and 22.4% with 3 diseases, respectively. In those aged 65 to 79 years, and 80 years or older, 5 or more diseases / coexisting conditions affected highest percentage of individuals, 35.5%, and 47.6%, respectively. A total of 2.2% of persons aged 65 to 79 years, 0.9% of those aged 80 years and more, and 8.5% of those aged 55 to 59 years had no diagnosis of chronic disease (Figure 1).
Prevalence and coexistence of diseases
Hypertension, metabolic diseases, and obesity predominated in participants aged 55 to 59 years and 65 to 79 years, and hypertension, eye disorders, and cognitive impairment predominated in those aged 80 years or older (Supplementary material, Figures S2–S4).
In all the age subgroups, hypertension constituted the most frequent single diagnosis, present in 7.8%, 4.1%, and 2% of those aged 55 to 59 years, 65 to 79 years, and 80 years or older, respectively. In participants younger than 80 years of age, metabolic disease, obesity, arrhythmia, psychiatric, and thyroid diseases were the conditions that each occurred individually more often than in 1% of the participants, whereas in the octogenarian and older group, cognitive impairment was the only condition that met this threshold (Supplementary material, Figures S2–S4).
In the youngest participants, kidney disease, cancer, Parkinson disease / epilepsy, and stroke always coexisted with at least one other disease. In those aged 65 to 79 years, stroke, and in those aged 80 years and older, stroke and heart failure, always coexisted with other conditions (Table 1).
Chronic disease | 55–59 years old | 65–79 years old | ≥80 years old |
Data are presented as odds ratio (95% CI) adjusted for sex and age.
a Disease perfectly predicted multimorbidity | |||
Hypertension | 11.6 (7.7–17.6) | 10.1 (7.6–13.5) | 6.4 (4.3–9.6) |
Metabolic diseases | 5.9 (3.6–9.6) | 10.7 (6.8–17.0) | 18.1 (6.7–49.5) |
Obesity | 8.4 (4.8–14.4) | 11.0 (6.6–18.1) | 10.5 (3.8–28.9) |
Psychiatric diseases | 6.7 (3.7–12.2) | 10.9 (5.9–20.1) | 11.4 (5.0–26.0) |
Arrhythmia | 10.9 (5.2–22.7) | 13.5 (7.3–24.8) | 69.7 (9.7–500.2) |
Thyroid diseases | 6.4 (3.0–13.5) | 6.7 (3.3–13.8) | 19.5 (2.7–140.7) |
Respiratory diseases | 16.0 (3.9–66.1) | 4.7 (2.6–8.4) | 11.2 (3.5–35.5) |
Ischemic heart disease | 11.6 (3.6–37.6) | 28.0 (8.9–87.8) | 43.7 (6.1–314.1) |
Osteoporosis | 7.0 (2.1–22.9) | 5.9 (2.7–12.8) | 7.9 (1.9–32.4) |
Eye disorders | 9.7 (2.3–40.8) | 7.5 (4.2–13.5) | 12.9 (6.0–27.9) |
Heart failure | 14.0 (1.9–103.6) | 16.6 (4.1–67.4) | a |
Anemia | 5.5 (1.3–23.6) | 16.0 (4.0–64.9) | 10.3 (3.8–28.2) |
Cognitive impairment | 11.4 (1.5–84.5) | 10.8 (4.4–26.4) | 2.8 (1.8–4.4) |
Kidney disease | a | 10.3 (4.2–25.2) | 18.5 (6.8–50.5) |
Cancer | a | 8.6 (2.1–35.1) | 9.2 (1.3–66.4) |
Parkinson disease and epilepsy | a | 4.0 (0.97–16.6) | 4.8 (0.66–35.2) |
Stroke | a | a | a |
In participants aged 55 to 59 years, the highest odds ratios for coexistence of 2 diagnoses were noted for: hypertension and kidney disease (OR, 11.36; 95% CI, 1.51–85.42), cognitive impairment and stroke (OR, 10.82; 95% CI, 2.63–44.44), cognitive impairment and kidney disease (OR, 9.06; 95% CI, 3.02–27.16), cognitive impairment and Parkinson disease / epilepsy (OR, 7.54; 95% CI, 1.95–29.17), kidney disease and stroke (OR, 8.50; 95% CI, 1.68–42.90), kidney disease and heart failure (OR, 7.05; 95% CI, 2.39–20.77), ischemic heart disease and arrhythmia (OR, 6.62; 95% CI, 3.88–11.28), ischemic heart disease and heart failure (OR, 6.52; 95% CI, 3.08–13.83), and heart failure and arrhythmia (OR, 7.82; 95% CI, 3.63–16.82). In individuals aged 65 to 79 years, for: ischemic heart disease and heart failure (OR, 6.55; 95% CI, 4.89–8.77), and for arrhythmia and heart failure (OR, 5.91; 95% CI, 4.35–8.05), arrhythmia and ischemic heart disease (OR, 4.22; 95% CI, 3.40–5.23). In the octogenarians and older participants, for: arrhythmia and ischemic heart disease (OR, 4.98; 95% CI, 3.93–6.31), and arrhythmia and heart failure (OR, 6.79; 95% CI, 4.95–9.32). The details of these analyses are presented in Supplementary material, Table S1.
Multimorbidity patterns
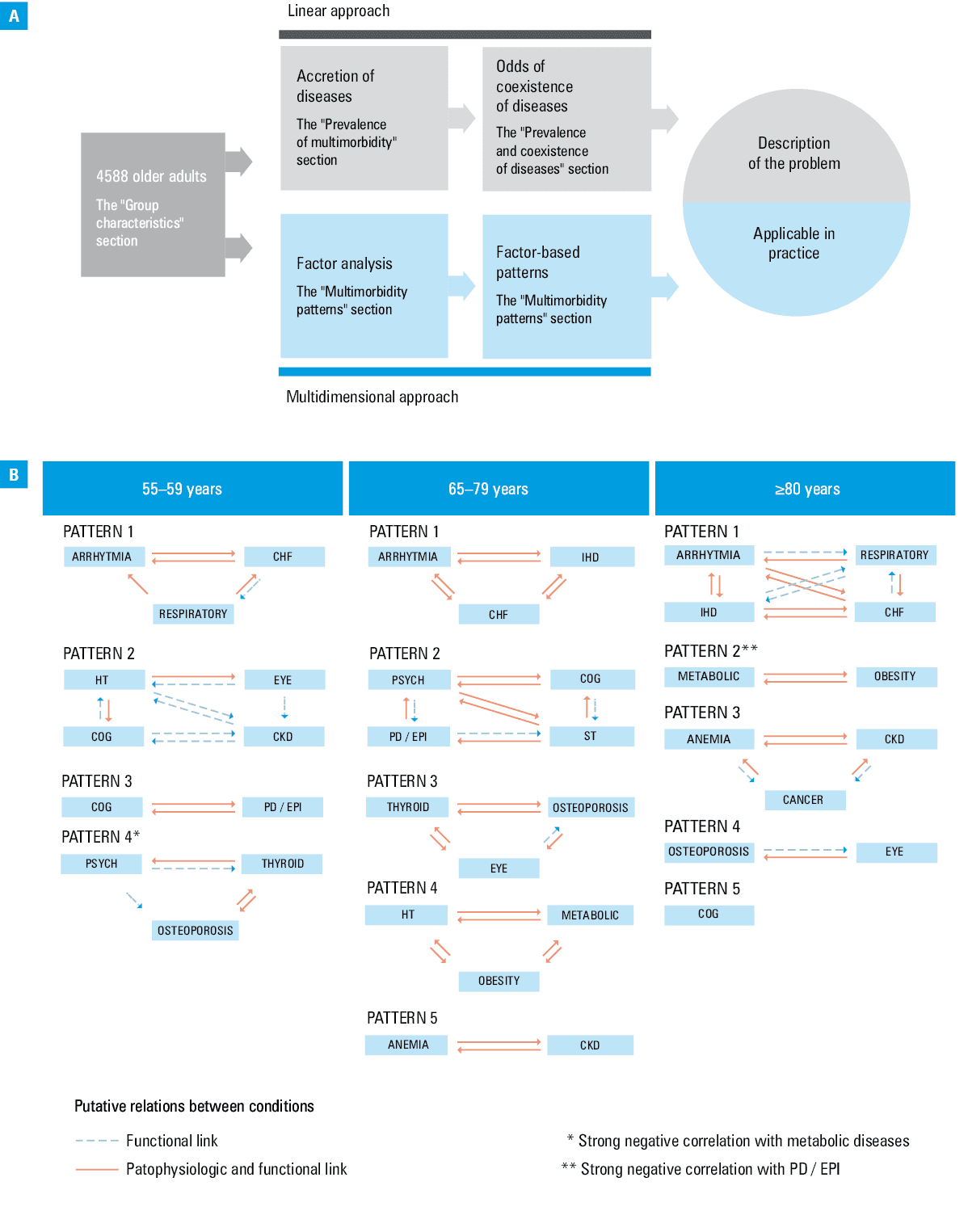
Both in participants aged 65 to 79 years and those aged 80 years or older, we established 5 multimorbidity patterns, composed of the diseases with highest loadings drawn from the 5 respective clusters. In those aged 55 to 59 years, patterns drawn from 4 clusters were established (Table 2). The first factor was cardiovascular disease‑related, with respiratory diseases included in the youngest and oldest participants. In the 55‑to‑59‑year‑old group, other patterns were as follows: the second pattern including cognitive impairment and Parkinson disease / epilepsy, the third pattern including chronic kidney disease, hypertension, eye disorders, and cognitive impairment; and the fourth including osteoporosis and psychiatric, thyroid, and metabolic diseases.
Chronic disease | 55–59 years olda | 65–79 years oldb | ≥80 years oldb | |||||||||||
Factor 1 | Factor 2 | Factor 3 | Factor 4 | Factor 1 | Factor 2 | Factor 3 | Factor 4 | Factor 5 | Factor 1 | Factor 2 | Factor 3 | Factor 4 | Factor 5 | |
a Four‑factor analysis
b Five‑factor analysis | ||||||||||||||
Hypertension | – | 0.597 | – | – | – | – | – | 0.505 | – | – | – | – | – | – |
Metabolic diseases | – | – | – | –0.372 | – | – | – | 0.447 | – | – | 0.386 | – | – | – |
Obesity | – | – | – | – | – | – | – | 0.484 | – | – | 0.689 | – | – | – |
Psychiatric diseases | – | – | – | 0.395 | – | 0.492 | – | – | – | – | – | – | – | – |
Arrhythmia | 0.678 | – | – | – | 0.662 | – | – | – | – | 0.719 | – | – | – | – |
Thyroid diseases | – | – | – | 0.339 | – | – | 0.408 | – | – | – | – | – | – | – |
Respiratory disease | 0.368 | – | – | – | – | – | – | – | – | 0.323 | – | – | – | – |
Ischemic heart disease | – | – | – | – | 0.712 | – | – | – | – | 0.757 | – | – | – | – |
Osteoporosis | – | – | – | 0.668 | – | – | 0.612 | – | – | – | – | – | 0.499 | – |
Eye disorders | – | 0.384 | – | – | – | – | 0.397 | – | – | – | – | – | 0.478 | – |
Heart failure | 0.733 | – | –– | 0.791 | – | – | – | – | 0.763 | – | – | – | – | |
Anemia | – | – | – | – | – | – | – | – | 0.659 | – | – | 0.412 | – | – |
Cognitive impairment | – | 0.383 | 0.580 | – | – | 0.615 | – | – | – | – | – | – | – | 0.649 |
Chronic kidney disease | – | 0.799 | – | – | – | – | – | – | 0.329 | – | – | 0.758 | – | – |
Cancer | – | – | – | – | – | – | – | – | – | – | – | 0.353 | – | – |
Parkinson disease & epilepsy | – | – | 0.696 | – | – | 0.496 | – | – | – | – | –0.355 | – | – | – |
Stroke | – | – | – | – | – | 0.372 | – | – | – | – | – | – | – | – |
In participants aged 65 to 79 years, beside the cardiovascular disease‑related pattern (heart failure, ischemic heart disease, arrhythmia), we identified: the mental pattern (cognitive impairment, Parkinson disease / epilepsy, psychiatric diseases, and stroke), the cardiometabolic pattern (hypertension, obesity, metabolic disease), the renal pattern (chronic kidney disease, anemia), and the pattern which included: osteoporosis, thyroid diseases, and eye disorders.
In the oldest, in addition to the cardiovascular pattern, the following patterns were traced: the metabolic pattern (obesity, metabolic diseases with Parkinson disease / epilepsy), the pattern including chronic kidney disease, anemia, and cancer, and the pattern with osteoporosis and eye disorders, and cognitive impairment as separate pattern (all other diseases in this factor had loadings of less than 0.3). Full results are presented in Table 2.
Discussion
We demonstrated that older patients (55–59 and 65+, years) are rarely diagnosed with a single disease, and the most prevalent form of pathology is cardiovascular disease. Further, irrespective of age group under study, arrhythmia, ischemic heart disease, and heart failure were the key conditions to cluster with other chronic pathologies. At all ages under study, stroke was related to multimorbidity, whereas heart failure was always linked with other conditions in patients aged 80 years or older (Figure 2).
We showed a high prevalence of chronic diseases and medical problems in those aged 65 years and more, but also in those aged 55 to 59 years. The median number of chronic conditions was 2 in the youngest participants and 4 in those aged 65 years and older, with the total number of chronic diseases and multimorbidity indices increasing steeply with age.
The patterns of multimorbidity in individuals aged 80 years or older differ from the overall picture. A total of 94% of oldest patients have multimorbidity and are burdened with 5 or more chronic conditions, on average. This underlines the often unmet needs of the oldest with hypertension, eye problems, and cognitive impairment, the 3 most frequent chronic medical problems in this group. An important practical aspect of our study is that of the 3 most frequent diseases demonstrated in the oldest, 2, namely hypertension and eye disorders, are potentially amenable to therapy.
Of note is the fact that only a minority of participant did not have any of the assessed chronic medical problems. Hypertension was the most frequent single condition in all age groups, followed by cognitive impairment (1.2%) in the oldest age group. However, the frequency of hypertension as a single ailment was low in absolute terms and was decreasing with age (from 7.8% to 4.1% to 2.0%, youngest to oldest age groups, respectively).
Our study was cross‑sectional, thus precluding assessment of causality. However, we determined the patterns of comorbidities which may be seen as pathophysiologically linked or functionally linked (Figure 2). The noticeable differences with regard to multimorbidity patterns between the analyzed age groups point to the need of individual care and specific diagnostic protocols based on age.
Results in the context of published reports
Our interest in multimorbidity, estimated at the national level, is in line with a worldwide concern for adequate healthcare and welfare provided for the older patients.2-4 It is hard to compare different studies on the topic due to varied methodologies and statistical approaches employed, as well as differences between study groups.6,12,13 Guisado‑Clavero et al14 studied 190 108 patients with multimorbidity. They used the electronic registry to assess clustering. Guisado‑Clavero et al14 identified 6 clusters; however, their clusters included up to 25 conditions which, in the face of lack of prioritization based on loadings, hampers the practical use of the information from this well‑performed study. In our study, we limited the patterns to diseases with loadings of more than 0.3, in respective clusters, which results in a maximum of 4 conditions per cluster. This, in turn, translates to a greater potential practical applicability of our results (Figure 2). In a study of multimorbidity, based on the German claims data of the participants aged 65 and older, van den Bussche et al15 showed that 73% of patients had at least 2, and 62% at least 3 chronic conditions, with the latter group classified as multimorbid having 5.8 chronic diseases on average. In the whole sample of those older insured patients, the average number of chronic conditions was 3.9, from a complete list of the 46 analyzed chronic diagnoses. Likewise, Kirchberger et al16 in the population‑based KORA‑Age study conducted in Southern Germany, estimated the prevalence of multimorbidity at 58.6%, with the median number of 2 out of the 13 examined chronic conditions. Of note, the numerical results describing multimorbidity depended, apart from the number of medical problems, on clinical methods used to confirm a diagnosis, investigated populations, and the quality and availability of healthcare in general.
Globally, the multimorbidity indices varied from 0.7% to 90.5%.17 However, the prevalence depends on the study setting, the definitions of multimorbidity, the diagnostic approaches in a given country at a given time, and the age of the population included.17,18 Some of the older studies give the values of 49% to 92% in the community‑dwelling older adults in urban and rural China, respectively, 65% (with 2 chronic diseases on average) in those living in sub‑Saharan Africa in Burkina Faso, 52% in older Australians, to even 93.9% in the inhabitants of a South Mediterranean region of Spain (with almost 8 chronic diagnosis per each multimorbid person).19-23 Garin et al24 analyzed data from 9 countries including Poland. Overall, the prevalence of multimorbidity was 62.7%. The estimated prevalence of multimorbidity in Poland was 69.4%, which is in line with our findings. They traced 3 main patterns, including a cardiorespiratory, metabolic, and mental‑articular patterns—a finding which we reproduce and extend.
In our analysis, we demonstrated that it is very rare for the elderly not to be diagnosed with any chronic disease or a single chronic disease. The likelihood of multimorbidity was related to the particular pathology, with heart failure, ischemic heart disease, arrhythmias, and chronic kidney disease increasing the risk more than 10‑fold, and stroke being associated with concomitant medical problems in all cases. Our finding of the high disease burden related to kidney disease corresponded to the results obtained by van den Bussche et al,15 showing the highest risk for multimorbidity in patients with renal insufficiency. In the KORA‑Age Study, Kirchberger et al16 found the strongest association between hypertension and diabetes, and hypertension and stroke, and next, they specified 4 comorbidity patterns, with cardiovascular and metabolic, and mental and neurological disorders confirmed by our results. Similar results were obtained, despite different setting, by Foguet‑Boreu et al23 with regard to the association of hypertensive disease and metabolic disorders in a study of the older population of Spain, and Schäfer et al25 in their study, based on the analysis of 46 chronic diagnoses put in claims data of almost 150 000 older respondents. Vetrano et al26 traced the 12‑year trajectories of cluster classifications. While persons categorized to cognitive and sensory impairment, eye disorders and cancer, and heart diseases tended to remain convergent on 2 to 3 main tracks, the persons in respiratory and musculoskeletal disorders cluster did not. This underlines the possibility of some clusters having less pathophysiologic bearing than other. Of note, the special role played by the cardiovascular burden is capable of modifying risk in multimorbid patients.27
Limitations
Our results should be considered within the context of the study limitations. First, the study was cross‑sectional which precluded assessment of causality. On the other hand, the purpose of the study was to show clustering of common chronic conditions and health‑related conditions to indicate to nongeriatricians the need to focus their limited time and resources on conditions associated with the index diagnoses. Also, as in any survey, both under- and overdiagnosis were possible. Further, as in the case of cognitive impairment and psychiatric diseases, the point estimates of ORs for multimorbidity tended to numerically differ between the age groups. However, the overlapping confidence intervals make the interpretation of these trends as real differences between the age‑groups impossible.
Third, although the causative nature of association cannot be inferred, the pathophysiologic consideration makes it possible to link conditions that constitute the patterns based on common pathophysiology or functional links (Figure 2). We had to exclude 19% of participants initially available in our database due to partially missing data. However, as judged by the unchanged prevalence of the particular conditions considered singly at the level of the entire group, the exclusion did not markedly influence the structure of the database (Supplementary material, Table S2).
The strength of our study rests on the fact that our data are based on a representative sample of the Polish population, the fifth largest in the European Union.
Conclusions and implications
Multimorbidity is prevalent in older patients. As cardiovascular disease has greatest potential for clustering, the recognition of other clustering conditions may be of special interest to nongeriatrician specialists, for instance cardiologists, and their patients in the process of shared decision making. Based on the data of 4588 older patients, we provide a guide to multimorbidity, with possible pathophysiologic links between clustering conditions in hope that this would serve as a useful shorthand reminder in daily care for older patients.
- Forman D, Maurer M, Boyd C, et al. Multimorbidity in older adults with cardiovascular disease. J Am Coll Cardiol. 2018; 71: 2149‑2161. | Crossref
- The Academy of Medical Science. Multimorbidity: a priority for global health research. 2018. https://acmedsci.ac.uk/file‑download/82222577. Accessed August 26, 2021.
- Pearson‑Stuttard J, Ezzati M, Gregg EW. Multimorbidity a defining challenge for health systems. Lancet Public Health. 2019; 4: e599‑e600. | Crossref
- Palmer K, Marengoni A, Forjaz MJ, et al. Joint Action on Chronic Diseases and Promoting Healthy Ageing Across the Life Cycle (JA‑CHRODIS). Multimorbidity care model: Recommendations from the consensus meeting of the Joint Action on Chronic Diseases and Promoting Healthy Ageing across the Life Cycle (JA‑CHRODIS). Health Policy. 2018; 122: 4‑11. | Crossref
- Kernick D, Chew‑Graham C, O’Flynn N. Clinical assessment and management of multimorbidity: NICE guideline. Br J Gen Pract. 2017; 67: 235‑236. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION