Assessment of pulmonary embolism severity and the risk of early death
Key words: mortality risk prediction, pulmonary embolism, risk stratification



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Assessment of pulmonary embolism severity and the risk of early death
Currently, venous thromboembolism, including deep vein thrombosis and acute pulmonary embolism (PE), is globally the third most frequent acute cardiovascular syndrome with rising incidence rates. The clinical presentation of PE is heterogenous: from incidental findings on imaging studies to sudden cardiac death. Hemodynamic instability identifies patients at high risk of early mortality. In hemodynamically stable patients, further stratification into intermediate- and low‑risk categories is advised, preferably using a combined risk assessment strategy based on clinical parameters, laboratory findings, and imaging markers. Treatment should be tailored to the risk of early death, with more aggressive treatments reserved for patients at higher risk of complications. This review offers an update on the current strategies for assessing PE severity and the risk of early death and discusses developments in predicting mortality risk in patients with PE.
Introduction
Justification for assessing pulmonary embolism severity and risk of early death
With epidemiological studies reporting that the current annual incidence rates of pulmonary embolism (PE) in Europe reach up to 115 per 100 000 population and of deep vein thrombosis (DVT), up to 162 for 100 000 population, taken together, venous thromboembolism (VTE) is the third most common cause of cardiovascular death in the Western World.1 Longitudinal studies show that there is also a rising tendency in PE incidence over time and it is plausible to expect that its prevalence will be steadily driven by the elongation of life span and increasing comorbidity of diseases which are risk factors for VTE (ie, obesity, cancer, heart failure) and a growing availability and sensitivity of diagnostic imaging techniques.2-5 It should be underlined that even though PE‑related mortality may be falling, its incidence is rising.
It has been established that in the course of PE, hemodynamic instability and right ventricular dysfunction (RVD) or failure resulting from rapid pressure overload are the main determinants of the patient’s risk of an adverse outcome. Thus, the evaluation of RV function remains the cornerstone of mortality risk assessment in PE.1 Depending on the degree of RV function compromise, a heterogeneous clinical presentation of PE from asymptomatic incidental findings on imaging studies to sudden cardiac death may be observed.
Based on clinical presentation as well as laboratory and imaging parameters, the European Society of Cardiology (ESC) guidelines on the diagnosis and management of acute PE classify PE into one of 4 categories (Figure 1).1 High‑risk PE is defined by the presence of hemodynamic instability, presenting as obstructive shock, cardiac arrest, or persistent hypotension refractory to treatment and not attributed to concomitant factors. This is the smallest subgroup accounting for 5% of all PE patients; however, with very high mortality rates approaching 30%. In order to prove that hemodynamic instability results from PE and to diagnose high‑risk PE, confirmation of RVD on imaging studies is required. At the other end of the severity spectrum, low‑risk PE is characterized by preserved RV function on the basis of both imaging studies and laboratory makers, along with a sufficiently low score using clinical risk prediction tools (such as the simplified PE severity index [sPESI], the PE severity index [PESI]). This group makes up about 25% to 35% of PE patients, with a very low mortality rate of 1% or lower. The last subgroup of intermediate‑risk PE is the largest and most heterogeneous, accounting for up to 60% of all PE cases, and with early mortality rates as low as 2% or as high as 10%. This population includes normotensive patients with evidence of RV compromise (on imaging studies, in laboratory parameters, or both) and patients classified as not being at low risk by clinical risk prediction tools.
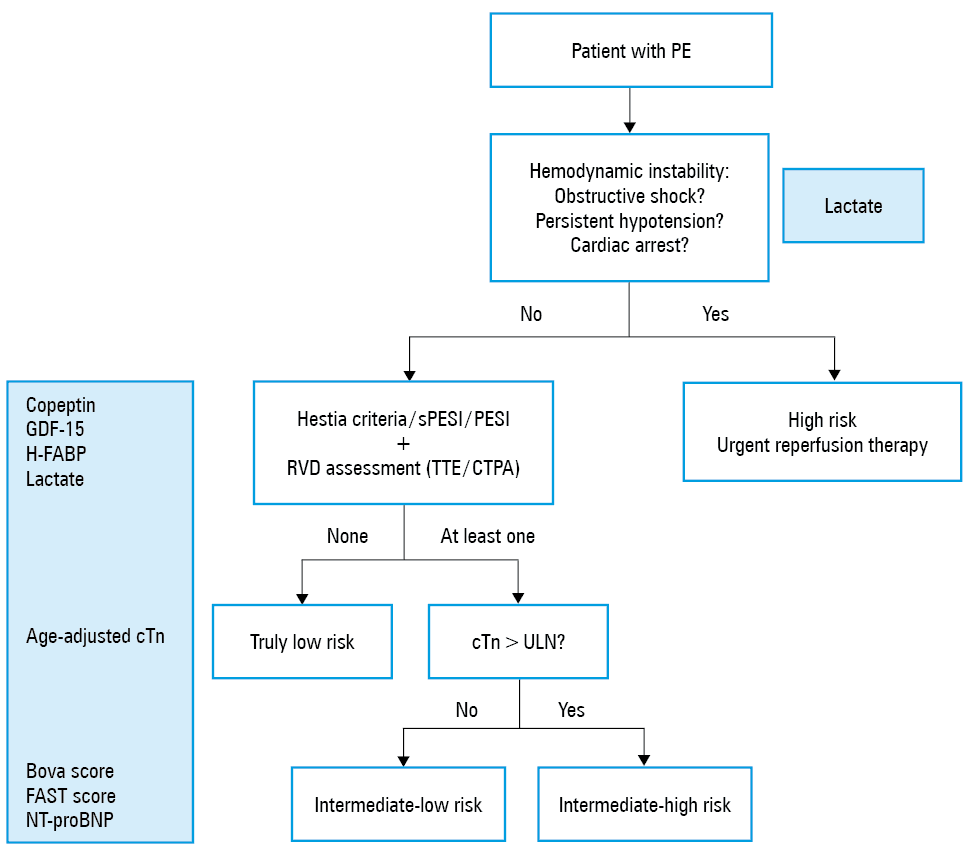
Abbreviations: cTn, troponin concentration; CTPA, computed tomography pulmonary angiography; GDF‑15, growth differentiation factor‑15; FAST, H‑FABP, syncope, tachycardia score; H‑FABP, heart‑type fatty acid‑binding protein; NT‑proBNP, N‑terminal pro‑B‑type natriuretic peptide; PE, pulmonary embolism; PESI, pulmonary embolism severity index; RVD, right ventricular dysfunction; sPESI, simplified pulmonary embolism severity index; TTE, transthoracic echocardiography; ULN, upper limit of normal
The quest for optimal risk assessment in PE stems from the notion that the administered treatment should be tailored to the risk of early death, with more advanced treatment options reserved for those with an elevated risk of early PE‑related mortality. Currently, a broad range of therapeutic strategies for PE is available: from oral to parental anticoagulation, systemic fibrinolysis, percutaneous interventions, or surgical interventions. In initially normotensive patients, mortality risk assessment and further management are challenging and require a multimodal diagnostic approach, with decisions preferably reached on a patient‑by‑patient basis by consensus in a dedicated interdisciplinary PE response team (PERT).6,7 The goal of risk stratification is to identify patients with the best benefit / risk ratio for more aggressive treatment at the upper end of the risk spectrum, and the candidates for early discharge and home treatment at the lower end. Despite many available tools, some of which are discussed below, stratification remains challenging in the intermediate‑high–risk group, where it continues to be an important area of ongoing research.
This review aims to present the current state of knowledge on mortality risk stratification in PE through the lens of established and emerging clinical characteristics, biomarkers, and imaging data. We briefly discuss a selection of proposed risk assessment strategies comprising the aforementioned components. Lastly, we touch on the most pressing gaps in knowledge involving risk assessment in normotensive patients with evidence of RV comprise.
Clinical predictors of an adverse outcome
Current research suggests that mortality in PE is dependent on the severity of the PE episode itself as well as the presence of comorbidities. Thus, risk stratification begins with the assessment of clinical parameters.
Validated clinical scores integrating severity and comorbidity of pulmonary embolism
The 2019 ESC guidelines offer an extensive definition of high‑risk PE, which comprises the following 3 clinical manifestations: cardiac arrest, obstructive shock, or persistent hypotension with systolic blood pressure of less than 90 mm Hg or its drop of 40 mm Hg or greater, lasting longer than 15 minutes and not attributed to new‑onset arrhythmia, hypovolemia, or sepsis.1 Accordingly, clinical symptoms and signs of overt RV failure and hemodynamic instability indicate a high risk of early (in‑hospital or 30 day) mortality.
Conversely, to identify the subgroup of low‑risk patients, a stepwise combined assessment is advised using the sPESI or PESI, or the Hestia exclusion criteria, preferably accompanied by RV function assessment with imaging studies. The components of each of these scores are presented in Table 1. Briefly, the PESI and sPESI are simple bedside scoring systems for prognostication of the risk of 30‑day adverse outcomes based on clinical parameters and concomitant diseases with the PESI score used in the landmark clinical trial PEITHO (Pulmonary Embolism Thrombolysis), as well as it being the only one validated in a randomized clinical trial.8-11 As one of its parameters is age of 80 years or older, its utility in patients under the age of 50 years old has been questioned and was ultimately positively tested in a comparative study.12 The Hestia exclusion criteria were developed and first tested in a prospective cohort study in patients with acute PE, who were selected for outpatient treatment if they did not meet a predefined set of exclusion criteria comprising 11 yes / no questions regarding the clinical presentation, comorbidities, familial and social factors of the patient.13 The Hestia criteria were tested in a study of 550 patients and performed satisfactorily when used to guide the decision on outpatient treatment.14 The concept of these 2 scoring systems was further investigated in the recently completed HOME‑PE (Hospitalization or Out‑treatment Management of PE) study, which compared the sPESI and Hestia criteria directly showing that both clinical scores may be used for initial risk stratification, with the sPESI classifying more patients as non‑low risk than the Hestia criteria, and more physicians choosing to override sPESI recommendations and aim for outpatient treatment.15
PESI | sPESI | Hestia exclusion criteria | ||
Item | Points | Item | Points | |
a Include the following criteria but leave them to the discretion of the investigator: systolic BP <100 mm Hg with heart rate >100 bpm; condition requiring admission to the intensive care unit.
b Gastrointestinal bleeding in the preceding 14 days, recent stroke (<4 weeks ago), recent operation (<2 weeks ago), bleeding disorder or thrombocytopenia (platelet count <75 × 109/l), or uncontrolled hypertension (systolic BP >180 mm Hg or diastolic BP >110 mm Hg).
c Calculated CrCl according to the Cockroft‑Gault formula.
d Left to the discretion of the physician.
Abbreviations: BP, blood pressure; CrCl, creatinine clearance; others, see Figure 1 | ||||
Age | = age in years | Age | 1 | Is the patient hemodynamically unstable?a |
Male sex | 10 | – | – | Is thrombolysis or embolectomy necessary? |
Cancer | 30 | Cancer | 1 | Active bleeding or high risk of bleeding?b |
Chronic heart failure | 10 | Chronic heart failure or chronic pulmonary disease | 1 | More than 24 h of oxygen supply to maintain oxygen saturation >90%? |
Chronic pulmonary disease | 10 | Is PE diagnosed during anticoagulant treatment? | ||
Pulse rate ≥110 bpm | 20 | Pulse rate ≥110 bpm | 1 | Severe pain needing intravenous pain medication for more than 24 h? |
Systolic BP <100 mm Hg | 30 | Systolic BP <100 mm Hg | 1 | Medical or social reason for treatment in the hospital for >24 h (infection, malignancy, or no support system)? |
Respiratory rate >30 breaths per minute | 20 | – | – | Does the patient have a CrCl of <30 ml/min?c |
Temperature <36° C | 20 | – | – | Does the patient have severe liver impairment?d |
Altered mental status | 60 | – | – | Is the patient pregnant? |
Arterial oxyhemoglobin saturation <90% | 20 | Arterial oxyhemoglobin saturation <90% | 1 | Does the patient have a documented history of heparin‑induced thrombocytopenia? |
Interpretation | ||||
|
| If at least one positive criterion, then the patient cannot be treated at home. | ||
There is growing evidence that, even in initially low‑risk patients, assessment of RV function may be warranted and risk stratification based on clinical prediction rules alone may not be sufficient. This is mentioned in the ESC guidelines, which recommend further RV assessment in initially clinically low‑risk patients (level of recommendation IIa, level of evidence B).1 The HOT‑PE (Home Treatment of Patients with Low‑Risk PE with the Oral Factor Xa Inhibitor Rivaroxaban) trial investigated the safety and efficacy of home treatment of PE using rivaroxaban in a low‑risk population, defined by the adapted Hestia criteria and the absence of RV enlargement or dysfunction (RV / left ventricle [RV/LV] ratio ≥1.0), and of free‑floating thrombi in the right atrium or ventricle on echocardiography or computed tomographic pulmonary angiography (CTPA). From the reported initial population of 2854 patients with objectively confirmed PE, 300 patients had either RV dysfunction or free‑floating thrombi despite being initially classified as low risk (ie, did not meet any of the Hestia exclusion criteria).16 Furthermore, a recent meta‑analysis of 3295 patients from 21 studies showed (20 using sPESI/PESI, one using the Hestia criteria) that RV dysfunction, primarily defined by RV pressure overload assessed on imaging tests, alternatively by elevated biomarkers, may have a significant impact on the early prognosis of patients classified as low risk based on the PESI, sPESI, or Hestia criteria.17
The same was demonstrated in the latest meta‑analysis of 5010 low‑risk patients which concluded that RV dysfunction assessed by echocardiography, computed tomography, or elevated B‑type natriuretic peptide (BNP) / N‑terminal pro–B‑type natriuretic peptide (NT‑proBNP) levels and increased troponin levels is associated with short‑term death in patients with acute PE at low risk based on the aforementioned clinical models.18
This brings forward the notion that home treatment of truly low‑risk PE should be encouraged; however, even in initially low‑risk patients according to clinical models, RV status using either imaging studies or troponin levels should be assessed on admission before the decision of home treatment / early discharge is made to correctly identify sufficiently low‑risk individuals who may be safe candidates for home treatment.
Laboratory markers of an adverse outcome
Troponins
Troponin T (TnT) and troponin I (TnI) are released from cardiomyocytes in response to increased cell membrane permeability, as in the case of ischemia or stretching due to increased preload or afterload.19 Elevated TnT and TnI levels have been associated with RV dysfunction on imaging studies as well as complicated outcomes in patients with PE.20-24 However, the low positive predictive value of troponins make them an unsuitable solitary tool for risk stratification, but alternatively, the high negative predictive value for mortality (98% in Lankeit et al)25 of high‑sensitivity TnT (hsTnT) with a cutoff of 14 ng/l is encouraging when used to distinguish patients at high risk of complications as part of a multimodal approach.1,25,26 A more recent concept is the use of age‑adjusted TnT cutoffs.27 In patients aged ≥5 years, a cutoff value of 45 pg/ml predicted an adverse outcome and provided additive and independent prognostic information on top of the sPESI and echocardiography with the area‑under‑the‑curve for the model of 0.770.27 Ebner et al28 recently investigated whether the use of high‑sensitivity TnI (hsTnI) could be of value in risk stratification of normotensive patients, concluding that hsTnI concentrations greater than 16 pg/ml predicted in‑hospital adverse outcome and all‑cause mortality suggesting that hsTnI and hsTnT can be used interchangeably for risk stratification. Consequently, employing high‑sensitivity troponin on top of the sPESI score may be feasible to identify “truly” low‑risk patients.14,28-30 Whether the same benefit may be seen for the Hestia criteria remains to be assessed, as data from the VESTA study up hereto remain inconclusive.31
Natriuretic peptides
Cardiomyocytes release NT‑proBNP in response to ventricular wall stress caused by volume or pressure overload, both of which are present in acute PE. Cardiomyocyte stretching initiates pre‑proBNP synthesis, which is subsequently cleaved into proBNP, and later into the active hormone BNP and its inactive N‑terminal fragment, called NT‑proBNP. Next, they are released into the blood in equimolar quantities.32 NT‑proBNP is characterized by a longer half‑life than active BNP and thus is more often measured in the serum. Primarily, increased BNP and NT‑proBNP levels were described as diagnostic tools in diseases of the LV.33 Subsequently, it was demonstrated that elevated serum NT‑proBNP levels: 1) are present in patients with RV overload; 2) are associated with RV overload on imaging studies.34-38 Due to its low specificity and positive predictive value (for early mortality) the ESC guidelines recommend employing NT‑proBNP to identify normotensive patients with an expected benign course of the disease, using a threshold of 500 pg/ml.1,39 To increase specificity to identify individuals at risk of complications, higher cutoff values, namely 600 pg/ml, may be used.37 NT‑proBNP has not been investigated in a conclusive randomized clinical trial focused on natriuretic peptide–guided management in PE.
Some authors present data on the utility of combining both aforementioned biomarkers (with the upper limit of normal for NT‑proBNP of 600 pg/ml and TnI either 0.04 μg/ml or 0.05 μg/ml, depending on the assay used) and signs of RV strain on either echocardiography or CTPA to identify intermediate‑high risk patients at risk of death or need for rescue thrombolysis.40,41
Further laboratory biomarkers
Contemporary ESC guidelines uniformly recommend using a multimodal approach, which includes biomarkers (namely troponins) to further stratify normotensive patents. The guidelines also state that “the optimal, clinically most relevant combination (and cutoff levels) of clinical and biochemical predictors of early PE‑related death remain to be determined, particularly about identifying possible candidates for reperfusion treatment among patients with intermediate‑risk PE”, hence the ongoing search for novel markers.
Systemic hypoperfusion and hypoxemia developing due to the impaired gas exchange together with the congestion associated with right heart failure lead to decreased tissue oxygenation, increased glycolysis, and release of lactate as a by‑product of the metabolic pathway. Typically, the primary isomer produced in humans, L‑lactate, is measured in the plasma. Increased arterial L‑lactate levels (>2 mmol/l) have been demonstrated to be associated with higher mortality in PE patients, showing an additive value to that of established biomarkers (troponin, NT‑proBNP).42-44 This has been explored especially in the subgroups of higher risk PE patients, that is, with intermediate‑high and high‑risk of death. Recently, Ebner et al45 proposed adding the easily obtained venous lactate levels above a higher cutoff, defined as more than 3.3 mmol/l, to the 2019 ESC stratification protocol and found that this results in increased sensitivity and specificity in adverse outcome and mortality prediction in the intermediate‑high risk subgroup of patients. The proposed higher than previously suggested cutoff may be in part explained by physiologically occurring slight differences in lactate concentrations between venous and arterial blood. Finally, Ebner et al46 also investigated whether the subgroup of high‑risk PE clinically presenting as obstructive shock could be better defined in terms of end‑organ perfusion and mortality with lactate measurement, reporting that patients with levels above 3.8 mmol/l were characterized by higher mortality and that applying this improved risk stratification.
Growth differentiation factor‑15 (GDF‑15) is a distant member of the transforming growth factor superfamily (TGF-β). It was first identified as a chemokine secreted by activated macrophages in response to oxidative stress.47 Now it has been shown that ischemic injury, mechanical stretch, neurohormones, and proinflammatory cytokines also stimulate the expression of GDF‑15 in cardiac myocytes.48 A growing body of evidence confirms its diagnostic and prognostic value in cardiovascular diseases including myocardial infarction, chronic coronary syndromes, chronic heart failure, DVT, and in relation to bleeding complications in patients with atrial fibrillation on anticoagulation.49-57 In contrast to many reports focusing on GDF‑15 and left heart disease, there is a vast gap in the knowledge regarding the RV. In 2008, Lankeit et al58 published a prospective report on the association between baseline serum GDF‑15 concentrations and the occurrence of death and adverse outcomes during a 30‑day observation period, based on a group of 123 normotensive patients. 82% of the study population had elevated levels of GDF‑15 (above 1200 ng/l). Multivariate analysis revealed GDF‑15 to be a better prognostic factor of mortality than the serum concentration of TnT or NT‑proBNP (odds ratio, 10 vs 4.3 for GDF‑15 and TnT, respectively; P <0.001; area under the curve for GDF‑15, 0.84 vs 0.72 for TnT). GDF‑15 concentrations have also been shown to adequately predict bleeding risk in patients with PE on anticoagulation and may be useful in mortality risk stratification.59
Studies indicate that a prothrombotic clot phenotype, characterized by the formation of compact fibrin clots relatively resistant to lysis, can be detected in patients with arterial and venous thromboembolic events including those following PE. Thus, venous thromboembolism is connected with the occurrence of thrombi resistant to lysis, and that prolonged clot lysis time assessed in plasma on admission might help identify intermediate‑risk patients with acute PE at increased risk of PE‑related death.60,61 Consequently, data on another thrombotic condition, atrial fibrillation, showed that a predictive value of GDF‑15 could be in part attributed to its association with prothrombotic blood alterations resulting in prolonged clot lysis.59-63 Finally, a recently published population‑based nested case‑control study comprising 416 patients with VTE and 848 age- and sex‑matched controls demonstrated that plasma GDF‑15 levels are a risk marker for future thromboembolism as well.64
Heart‑type fatty acid‑binding protein (H‑FABP) in the context of short‑term risk stratification in PE was first described by Kaczyńska et al65 in 2006 in a prospective cohort. These findings were later reproduced in both normotensive and unselected PE populations demonstrating that H‑FABP seems to be a promising biomarker for risk‑stratifying low‑intermediate risk patients with acute PE.66-68 A meta‑analysis of 9 studies including 1680 patients found that elevated H‑FABP levels of 6 ng/ml or greater were associated with a complicated clinical course, and 30‑day PE‑related mortality.69 These data are promising; however, randomized clinical trials designed to assess biomarker‑guided treatment are necessary to validate the feasibility of this marker.
Copeptin, the C‑terminal fragment of the precursor protein of vasopressin, is released upon hypotension, low cardiac output, and endogenous stress. It has been reported in a multicenter validation study that copeptin, with a cutoff of 24 pmol/l or greater helps distinguish normotensive patients with PE at risk of adverse events, especially if integrated into a biomarker‑based algorithm.70-72
Imaging parameters of an adverse outcome
Echocardiography
Acute PE may lead to RV pressure overload and dysfunction in approximately 2% of patients, which can be detected by echocardiography. Given the peculiar geometry of the RV, there is no individual echocardiographic parameter that provides fast and reliable information on RV size or function. Therefore, various echocardiographic parameters including RV enlargement and hypokinesis, flattening of the intraventricular septum, an elevated velocity of tricuspid valve regurgitation, a decreased RV contractility assessed with tricuspid annular plane systolic excursion (TAPSE) were reported to be of prognostic value in acute PE.73-76 Mortality rates observed in various cohorts of normotensive PE patients with RVD diagnosed by different echocardiographic criteria varied from 4.3% to 16.4%.73,77 Despite this, according to the ESC guidelines on PE, echocardiographic assessment is not a mandatory part of the routine diagnostic workup in hemodynamically stable patients with suspected PE. However, importantly, it was reported that RVD affects the prognosis also in patients clinically classified as low risk.17,18 In contrast, hemodynamically stable patients with a preserved RV function have a favorable prognosis and are potential candidates for short‑term hospitalization or ambulatory treatment.75 Therefore, RVD by echocardiography or computed tomography especially when associated with elevated troponins levels is associated with early death in patients with acute PE at low risk based on clinical models. RVD assessment should be considered to improve the identification of low‑risk patients that may be candidates for outpatient management or short hospital stay.78 On the other hand, mortality rates observed in various cohorts of normotensive patients with PE and RVD diagnosed by different echocardiographic criteria varied from 4.3% to 16.4%.73,77 Systematic reviews and meta‑analyses have indicated that RVD is associated with an elevated risk of short‑term mortality, its overall positive predictive value for PE‑related death is low.73 However, no uniform definition of RVD was used across the studies for prognostic assessment.
Recently, a large European multicenter prospective cohort study including 490 normotensive PE patients managed according to the current ESC guidelines provided a proposal of the optimal definition of RVD for prognostic assessment.79 A multivariable analysis identified systemic systolic blood pressure, RV / LV ratio, and TAPSE to be independent predictors of PE‑related mortality, hemodynamic collapse, or rescue thrombolysis within the first 30 days. Importantly, a combined RVD criterion (TAPSE <16 mm and RV/LV ratio >1) was present in 60 patients (12%) and showed a positive predictive value of 23.3% with a high negative predictive value of 95.6% for adverse outcomes (hazard ratio, 6.5; 95% CI, 3.2–13.3; P <0.0001). It seems that RVD on echocardiography defined by RV / LV ratio of more than 1 in combination with TAPSE of less than 16 mm identifies among normotensive PE patients those with an increased risk of 30‑day adverse outcome including PE‑related mortality. This echocardiographic definition of RVD may be helpful in better defining intermediate high‑risk PE.79
Computed tomographic pulmonary angiography
The general inclination towards RV assessment in a CTPA is the possibility of running both a diagnostic and prognostic test at once. It is reassuring that repeated measurements performed by expert radiologists as well as physicians trained in CTPA interpretation show a satisfactory intra- and interobserver correlation.26 Among tested parameters, the RV / LV ratio measured in the transverse view by identifying the maximal distance between the ventricular endocardium and the interventricular septum, perpendicular to the long axis of the heart has the most robust evidence as a prognostic marker and recent reports show that it can be reliably measured automatically in the majority of real‑world cases of acute PE, with good reproducibility.80,81 Values of 1.0 or greater are believed to be appropriate to indicate a poor prognosis; however, it should be noted that they are very common in the initially low‑risk subgroup classified using clinical prognostic rules.80,81 Defining the optimal cutoff for low‑risk patients remains to be determined, with some studies conducted on smaller groups of patients suggesting a threshold of 1.2.82 In all patient subgroups, the odds ratio for adverse outcomes increases with increasing values of RV / LV ratio.80 Other explored indices, however with less plethoric data, are listed below: 1) assessed qualitatively / semiqualitatively: the presence of contrast backwash to the inferior vena cava, septal bowling83,84; 2) assessed quantitively: ratio of the RV to aortic outflow tract diameters, the volume of heart chambers.85
Combined risk‑assessment strategies
Several other strategies have been proposed, focusing on the subgroup of normotensive patients with signs of RV strain. Both the Bova score and the FAST (H‑FABP, syncope, tachycardia) score have been validated in cohort studies. Employing easily obtainable clinical, laboratory, and imaging parameters (Table 2), the Bova score stratifies normotensive patients with acute PE into stages of increasing risk of 30‑day PE‑related complications.86-88 Further prognostic may be achieved by combining lactate measurement with the Bova score.88 The FAST score—quick as the name suggests—does not require imaging parameters. Instead, the FAST score focuses on syncope, tachycardia, and H‑FABP concentration.89 Although a promising biomarker, H‑FABP is not routinely available in the majority of hospitals. Hobohm et al90 tested whether substituting H‑FABP for TnT or TnI yields a comparable risk stratification algorithm (named the modified FAST), concluding its feasibility but not superiority when compared with the ESC 2019 algorithm. Prospective management trials designed to externally validate and implement emerging prediction rules are necessary before these can be integrated into routine clinical practice.
Bova | FAST (modified) | ||
Item | Points | Item | Points |
a Troponin T or troponin I above the manufacturer’s cutoff
b ≥6 ng/ml
Abbreviations: CT, computed tomography; others, see Figure 1 | |||
Elevated cardiac troponina | 2 | Elevated H‑FABPb (or troponina) | 1.5 |
Heart rate >110 bpm | 1 | Heart rate >100 bpm | 2 |
Systolic blood pressure, 90–100 mm Hg | 2 | Syncope | 1.5 |
RVD (TTE or CT) | 2 | – | – |
Risk classes | |||
|
| ||
COVID‑19 and thrombosis
The possibility of concurrent PE complicating COVID‑19 should be considered when a patient exhibits hemodynamic instability or poor gas exchange that is not fully explained or is out of proportion to the stage, duration, and rate of progression of COVID‑19. According to the ESC guidelines, although the specificity of D‑dimer tests may be lower in patients with COVID‑19 compared with other clinical settings, it is still advised to follow diagnostic algorithms starting with pretest probability and D‑dimer testing and followed by imaging studies.91,92 On the other hand, a CHEST guideline and Expert Panel Report by Moores et al93 discourages employing biomarkers in the diagnostic evaluation for suspected DVT or PE, concluding that there are insufficient data to guide clinical practice on this basis. Notwithstanding the above, it is plausible that any diagnostic and therapeutic decisions regarding patients with COVID‑19 with the suspension of concomitant PE should be reached in a local PERT, on an individual patient‑by‑patient basis.94-96
Conclusions
Given the plethora of therapeutic options for patients with PE, ranging from oral medication to percutaneous interventions, clinical outcome–driven, randomized controlled trials are needed to further elucidate proper risk stratification, especially regarding the management of the intermediate‑high risk subgroup.
- Konstantinides SV, Meyer G, Becattini C, et al. The 2019 ESC guidelines on the diagnosis and management of acute pulmonary embolism. Eur Heart J. 2019; 40: 3453‑3455. | Crossref
- Becattini C, Agnelli G. Acute treatment of venous thromboembolism. Blood. 2020; 135: 305‑316. | Crossref
- Keller K, Hobohm L, Ebner M, et al. Trends in thrombolytic treatment and outcomes of acute pulmonary embolism in Germany. Eur Heart J. 2020; 41: 522‑529. | Crossref
- Bikdeli B, Wang Y, Jimenez D, et al. Pulmonary embolism hospitalization, readmission, and mortality rates in US older adults, 1999‑2015. JAMA. 2019; 322: 574‑576. | Crossref
- Lehnert P, Lange T, Møller CH, et al. Acute pulmonary embolism in a national Danish cohort: increasing incidence and decreasing mortality. Thromb Haemost. 2018; 118: 539‑546. | Crossref
ARTICLE INFORMATION