Aspects of the modern management of bronchiectasis
Key words: bronchiectasis, intervention, management



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Aspects of the modern management of bronchiectasis
While bronchiectasis is an old condition, it is only in the last decade that there have been major strides in our understanding of this disease and its treatment. Recent evidence has shown that the “vicious cycle” hypothesis remains valid. This, and the concept of “treatable traits,” provide useful frameworks on which to base the management of this condition. In all recently diagnosed patients, a search should be undertaken for specific etiologies. A number of factors, including chronic infection by Pseudomonas aeruginosa, have been shown to be associated with increased morbidity and mortality. While airway clearance strategies remain the mainstay of therapy, other treatments including nebulized hypertonic saline and inhaled antibiotic treatment are discussed. Greater emphasis is being placed on immune‑modulatory therapies, not just long‑term macrolide therapy but other more innovative strategies. The role of surgical lung resection in the management of this condition is also discussed.
Introduction
This article will focus on several recent developments and other aspects that will hopefully be of interest to specialists in internal medicine. It is not intended as a comprehensive review of bronchiectasis and its management; for this, the reader is directed to other recent publications.1-4
Bronchiectasis was first described by the French physician Rene Theophile Hyacinthe Laënnec, the inventor of the stethoscope, in 1819 in his book, the English version of which is entitled A Treatise on the Diseases of the Chest and on Mediate Auscultation. However, it is only in the last decade that bronchiectasis has gone from a “neglected cause of respiratory morbidity and mortality”5 with a very limited evidence base for management, and has “…(shaken) off its orphan status.”6 The condition has recaptured its name (and is no longer referred to as “noncystic fibrosis bronchiectasis”).7 It is now the topic of clinical prediction tools,8,9 a comorbidity index,10 an updated computed tomography (CT) scoring system,11 disease‑specific quality of life scales,12,13 a research priority register listing the 55 (!) key research priorities,14 and a number of large good quality randomized controlled trials (RCTs). In the light of these substantial developments, and the fact that bronchiectasis is a condition responsible for a substantial global economic and human burden,15 it is an ideal topic for a contemporary clinical review.
Diagnosis
Nowadays, the diagnosis of bronchiectasis is based on radiologic, specifically high‑resolution CT scans criteria. The criteria are as follows: a lack of tapering of airways, visible airways within 1 cm of the pleural surface but most often a B:A ratio (the ratio of the diameter of the airway to the diameter of the accompanying branch of the pulmonary artery) of >1. However, it must be remembered that bronchiectasis is first and foremost a clinical condition. This is reflected in the definition: “a chronic condition characterized by irreversible destruction and dilatation of airways, generally associated with chronic bacterial infection and symptoms of cough and sputum.”1
Not all patients who meet the radiologic criteria fulfil the clinical criteria. This is particularly the case in older patients, often with chronic airways disease, who have thin‑walled “bronchial dilatation” affecting the basal segmental branch of the lower lobes, without symptoms of cough and sputum production. There is some evidence that in such patients the increased B:A ratio is not due to bronchial dilatation but due to narrowing of pulmonary arteries,16 possibly on the basis of regional hypoxic vasoconstriction related to basal airway closure during tidal breathing in the elderly. The finding that bronchial lumen size was more strongly correlated with forced expiratory volume in first second of expiration (FEV1) than pulmonary artery diameter is also consistent with the concept of dysanapsis; that the bronchial tree and lung parenchyma may develop relatively independently of each other. The increased B:A ratio seen in smokers (and likely responsible at least in part for the high rate of “bronchiectasis” cases reported in patients with chronic obstructive pulmonary disease) seems to be mainly due to reductions in vascular caliber rather than bronchial dilatation17 and thus termed “mistaken identity” in an accompanying editorial.
It is not clear to what extent the increasing prevalence of bronchiectasis, particularly in the elderly, reported in several countries, is due to increased use of thoracic CT scans and / or differences in diagnostic criteria (related to some of the points above).
Etiology
The “vicious cycle” hypothesis of airway wall damage, impaired clearance of secretions, chronic infection and inflammation, and worsening pulmonary damage, was proposed a number of decades ago by Professor Peter Cole.18 In recent years, a number of studies exploring the microbiologic as well as the inflammatory and immunologic basis of bronchiectasis have provided modern evidence supporting Cole’s hypothesis.19-21 Neutrophils in bronchiectasis inherently have greater activation, increased degranulation, but impaired phagocytosis and bacterial killing.20,21 This “vicious cycle” and the current therapeutic interventions directed towards its various aspects are illustrated in Figure 1.
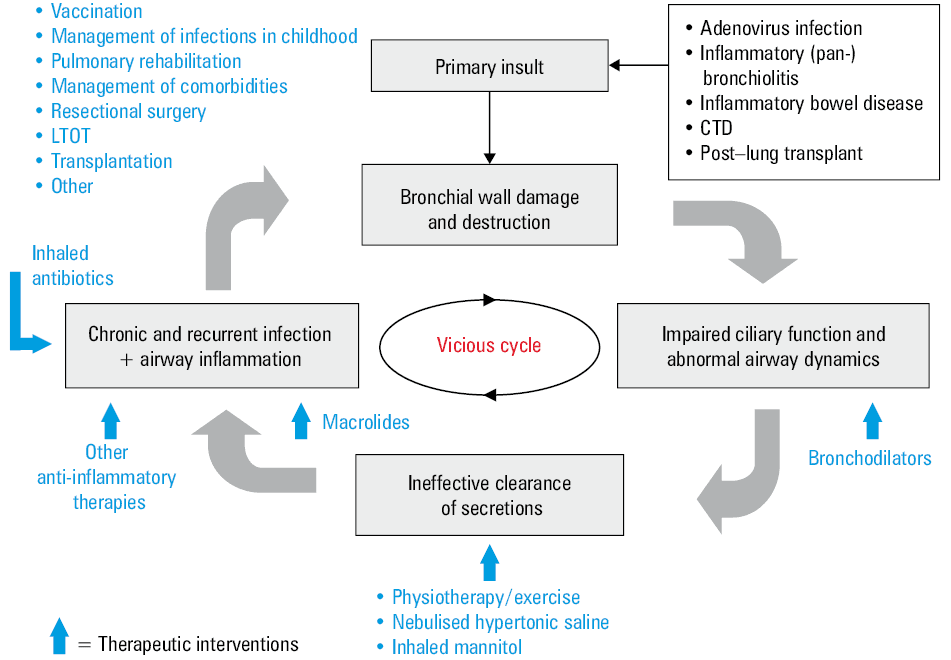
Abbreviations: CTD, connective tissue disease; LTOT, long‑term oxygen therapy
The concepts of “treatable traits” has been applied to the management of a number of airway diseases, and bronchiectasis is no exception.3 The management of the condition is approached under the headings of:
-
pulmonary (manifestations),
-
etiological,
-
extra‑pulmonary manifestations or related conditions (such as chronic rhinosinusitis and gastroesophageal reflux), and
-
environmental / lifestyle factors.
While this approach merely formalizes the approach already undertaken by many clinicians, it nevertheless provides a useful framework through which to approach the management of bronchiectasis.
As an example, Table 1 lists the tests recommended for the investigation of the etiology of bronchiectasis. Nevertheless, in most cases, no specific etiology is found and is labelled “idiopathic.”22 While many such cases are thought to be due to infection in early childhood (adenoviral bronchiolitis perhaps being the best studied), seldom is there compelling evidence for such an etiology, and there is often the difficulty of distinguishing between a causative event and an infection occurring as a complication of pre‑existing disease and leading to the diagnosis.
Abbreviations: IgE, immunoglobulin E |
|
The British Thoracic Society (BTS) guidelines1 recommend the measurement of specific antibody levels to identify specific polysaccharide antibody deficiency and argue that low antibody levels against Streptococcus pneumonia may represent an indication for the 23 valent polysaccharide pneumococcal vaccination. Another approach is to measure the antibody response to vaccination of those with low or borderline immunoglobulin levels to determine the adequacy of the humoral immune response. Measurement of sweat chloride (to detect abnormalities of ion and water transport), rather than genotyping, is used to “screen” for cystic fibrosis (CF). Only if sweat chloride is high (>60 mmol/l) or intermediate (40–60 mmol/l) should genotyping be undertaken. If 2 causative mutations are not identified on the local panel tested, then CFTR gene sequencing may be required. Many patients diagnosed with CF as adults will have retained pancreatic exocrine function and therefore are likely to have been missed on newborn screening testing based on the measurement of immune‑reactive trypsinogen. Because of the increasing availability of cystic fibrosis transmembrane regulator modulator therapy and the dramatic responses to such therapy, it is important that this condition is not missed. The measurement of nasal nitric oxide levels is recommended as the first‑line investigation for primary ciliary dyskinesia; it has a specificity of 96% but a sensitivity of 91%.1 It is useful to remember that most men with CF or primary ciliary dyskinesia are infertile, so a history of paternity is important. Routine screening for alpha‑1 antitrypsin deficiency is not recommended because of a low rate of detection.23 Bronchiectasis may be a feature of some connective tissue diseases (particularly rheumatoid disease) and inflammatory bowel diseases (ulcerative colitis but also Crohn disease).24
While the underlying mechanisms in bronchiectasis differ from those in cystic fibrosis (where mutations in the genes encoding the ion channel protein, cystic fibrosis transmembrane regulator, cause abnormalities in ion and water transport), recent studies of the mucus and airway secretions from patients with bronchiectasis have shown some similarities to the findings in CF. In mucus from bronchiectasis patients, there is a higher percentage of solids (an index of dehydration), a dysregulation of mucus secretion with greater amounts of MUC5B, increased mucus osmotic pressure, and higher DNA content.25 These factors lead to changes in the physical properties of the mucus (increased viscosity and elasticity) of a magnitude that would lead to an impairment of mucociliary clearance. The solid content of the mucus correlates with indicators of disease severity. In a clinical component of this study, the inhalation of nebulized hypertonic saline reduced mucus concentration by 25%. While nebulized hypertonic saline is now a mainstay of therapy in CF on the basis of good‑quality evidence, there have been only 2 small RCTs of this treatment conducted in patients with bronchiectasis26,27 with varying results. Nevertheless, the BTS guidelines conclude that hypertonic saline “may improve quality of life, outcomes and sputum clearance in individuals with bronchiectasis…” Nebulized hypertonic saline is a cheap, well‑tolerated treatment that influences the physical properties of airway mucus in a way that may lead to more effective clearance of airway secretions, particularly if used in association with conventional airway clearance strategies that remain the mainstay of therapy in bronchiectasis.1,28
However, there are fundamental differences in the underlying pathophysiology between CF and bronchiectasis, and treatments that may be effective in one are not necessarily effective in the other. Perhaps the best example of this is Pulmozyme (dornase alfa, recombinant human DNase) which is effective in CF, but has been shown to increase the exacerbation rate in bronchiectasis.29 Thus, it is not justified to use treatments for bronchiectasis based solely on their effectiveness in CF.
There is also the danger of extrapolating from other conditions to the management of bronchiectasis. The United States bronchiectasis registry30 demonstrated that more than a third of patients with bronchiectasis were taking inhaled corticosteroids, despite a Cochrane Review on the subject showing no convincing benefit in idiopathic bronchiectasis31 and that inhaled corticosteroids may increase the risk of infection by nontuberculous mycobacteria (NTM).32
Morbidity
Bronchiectasis is a heterogeneous condition in terms of etiology, clinical manifestations, radiologic appearance, exacerbation frequency, impairment of pulmonary function, and microbiology—and it is this heterogeneity (and therefore varying responses) which is thought to have contributed to the somewhat disappointing results of many RCTs, particularly of inhaled antibiotics.33 Based on clinical prediction tools8,9 a number of factors have been associated with a poorer outcome, increased morbidity and mortality. These factors include high dyspnea scores, impaired pulmonary function, the radiologic extent of disease, chronic Pseudomonas aerigunosa infection, hospitalizations, and frequent exacerbations. Thus, patients with one or more of these factors, certain etiologies, and high morbidity should be considered for follow‑up by an internal medicine specialist. These factors are listed in Table 2.
Abbreviations: NTM, nontuberculous mycobacteria; PA, Pseudomonas aeruginosa |
Etiology |
|
Severity |
|
High morbidity |
|
A previous challenge for those conducting trials in bronchiectasis was the absence of a reliable, relevant, and responsive primary outcome. FEV1, used in studies of asthma and chronic obstructive pulmonary disease, is not responsive in bronchiectasis and may be of limited clinical significance. Sputum measures (volume, purulence, and inflammatory markers) are beset by technical factors and concerns about clinical relevance. The situation has improved greatly with the development of a consensus definition of a pulmonary exacerbation34 and the validation of disease‑specific quality‑of‑life measures.11,12
Bronchiectasis registers have been established in the United States30 and Europe,35 and in time, they should provide valuable data on etiology, microbiology, management, and natural history of bronchiectasis. However, it is important that these registries are representative of the bronchiectasis population in the community. The United States registry may not reflect the majority of patients with bronchiectasis as in this register, White female patients chronically infected with NTM predominated—likely a reflection of the clinical expertise in the contributing centers. Disproportionately, bronchiectasis is a disease of indigenous populations (specifically in New Zealand, Australia, and Canada), the poor, and the disadvantaged. The next challenge is to recruit patients into these registers from a wider range of centers, to be more geographically representative, and to include ethnic minorities and the socioeconomically disadvantaged.
Microbiology
A recent study of the lung microbiome in bronchiectasis36 has shown that in severe disease, there is a reduced diversity of bacterial species and that organisms such as Pseudomonas aerigunosa, Enterobacteriaceae, and Stenotrophomonas predominate, both when clinically stable and during exacerbations. Individual patients’ microbial profiles were relatively stable over time. The evidence of limited microbiologic change during exacerbations challenges the conventional view that exacerbations are primarily caused by bacteria, specifically Gram‑negative bacteria found in expectorated sputum cultures.
Chronic Pseudomonas aerigunosa infection is associated with an increased exacerbation rate, poorer quality of life, greater impairment of pulmonary infection, and increased mortality. It is for that reason that many advocate attempts to eradicate this organism when it is first cultured. However, there is no evidence as to what regimen is most effective, although the BTS guidelines1 recommend oral ciprofloxacin for 2 weeks, as the first of several alternatives.
The high rate of chronic infection by NTM, predominantly Mycobacteria avium‑intracellulare complex (MAIC) is increasingly recognized in patients with idiopathic bronchiectasis; more than 60% in one study.30 Many bronchiectasis patients have NTM infection and the majority of patients with NTM have some radiologic evidence of bronchiectasis. The relationship between NTM and bronchiectasis is likely to be complex and bidirectional. Originally described in slim elderly females, with predominantly right middle lobe bronchiectasis (the so‑called Lady Windermere Syndrome), the spectrum of disease is now recognized to be much wider. Diagnosis is based on sputum culture, as there is considerable overlap of the CT appearances of bronchiectasis and NTM infection. The decision‑making about if, when, and how to treat NTM infection is no easier in this situation than in others.
Aspects of management
The goals of management in bronchiectasis are to reduce symptoms, prevent exacerbations, and to prevent further decline in lung function. Therapeutic interventions have targeted all aspects of the “vicious cycle” (Figure 1). In the following paragraphs, only a limited number of theses interventions will be discussed. Nevertheless, airway clearance techniques remain the mainstay of therapy, although even modern studies indicate that this is undertaken on a daily basis by only about 50% of patients.30
Because of the adverse consequences associated with chronic Pseudomonas aerigunosa infection outlined earlier, chronic suppressive inhaled antibiotic therapy has been suggested as a means of reducing bacterial burden, reducing inflammation and as a result, reducing morbidity. Multiple antibiotics and a variety of modes of delivery have been trialed. While some trials have produced positive results, overall, the results have been disappointing,21 despite demonstrated reductions in bacterial load.
One of the studies producing a positive result used an old and cheap antibiotic—the intravenous formulation of gentamicin delivered by nebulizer.37 Over the 12 months of the study, nebulized gentamicin (compared with placebo) produced microbiologic improvements (reduced sputum bacterial density, an increased rate of Pseudomonas aerigunosa eradication), reduced inflammation / infection (less sputum purulence and lower inflammatory markers in sputum) and improvements in patient‑centered outcomes (improved exercise capacity, fewer exacerbations, and improved quality of life) but no change in lung function. Hence, nebulized gentamicin (or alternately nebulized colistin) is a treatment recommended by the BTS guidelines1 as suppressive therapy for patients with chronic PA infection experiencing frequent exacerbation or other morbidity.
Given the fundamental importance of abnormal mucociliary clearance in the pathogenesis of bronchiectasis, it is not surprising that therapeutic strategies to augment airway clearance techniques (chest physiotherapy) have been investigated. Classes of drugs studied include expectorants, mucoregulators, mucolytics, and mucokinetic agents. Despite the attractions of cost and safety of nebulized hypertonic saline, there are limited data on its use (see above). Other agents have shown nil or only limited effectiveness. For example, a 52‑week double‑blind, randomized controlled trial of inhaled mannitol (versus control) in bronchiectasis patients with chronic cough and sputum and high rate of exacerbations, failed to show a statistically significant reduction in exacerbations but did show benefits in a number of secondary outcomes.38
In recent years, there has been greater attention to modulating the immune responses in order to reduce symptoms, prevent exacerbations, and reduce long‑term damage to the lung. Macrolides can influence various aspects of innate immunity including suppression of neutrophil‑mediated lung damage, improved mucociliary clearance, and beneficial effects on the virulence properties of bacteria. Three “large,” double‑blind, placebo‑controlled RCTs of long‑term macrolide therapy in patients with bronchiectasis39-41 have demonstrated significant reductions in exacerbations and a number of other benefits over the 6- to 12‑month period. In all studies where it was examined, long‑term macrolide therapy led to the development of macrolide resistance, although the clinical significance of this remains unclear. Also to be considered are cardiac and auditory complications of macrolides, the need for care in patients with renal impairment, and the requirement to exclude NTM infection before initiating such therapy. In view of this, and considering responsible antibiotic stewardship, macrolide therapy should not be used in all patients with bronchiectasis. An individual patient data meta‑analysis failed to identify subgroups more likely to respond.42 The potential benefits need to be weighed against the risks of adverse effects and the development of resistance. The BTS guidelines1 recommend that macrolide therapy (azithromycin 250 mg 3 times per week) be reserved for those with high morbidity, poorly controlled bronchopulmonary suppuration, and / or more than 3 exacerbations per year.
Previous studies have examined means of enhancing the immune response and thus facilitating bacterial suppression or eradication in bronchiectasis. However, there is evidence to suggest that there is an exuberant inflammatory response (to infection) in bronchiectasis and that this is at least in part responsible for lung damage; a sort of “collateral damage.” Reducing this excessive response without overly suppressing the immune response may be beneficial.
Dipeptidyl peptidase 1, also known as cathepsin C, is the enzyme responsible for the activation of the neutrophil serine proteases (neutrophil elastase, proteinase 3, and cathepsin G) found within cytoplasmic granules of the neutrophil and which can cause lung damage through a variety of mechanisms. Brensocatib is an oral, reversible, partial inhibitor of dipeptidyl peptidase 1. A double‑blind, placebo‑controlled, randomized phase II study of brensocatib in bronchiectasis43 demonstrated reduced rates of exacerbations without significant adverse effects such as compromised antibacterial defenses. A phase III study is underway. It is likely that future studies in bronchiectasis will also focus on modulating the immune response.
An issue that exercises clinicians is the role of surgical resection of affected lung in the management of bronchiectasis. Guidelines are relatively silent on this issue; not surprisingly, in view of the lack of data on which to base recommendations. What is still probably the best summary of the situation was written by the famous Scottish respiratory physician, Sir John Crofton, in 1966:
Most physicians would agree that surgical treatment is highly successful in patients with moderate or severe symptoms, whose bronchiectasis is localized to a single lobe or segment and without clinical or bronchographic evidence of bronchiectasis or bronchitis affecting other parts of the lung. Unfortunately such cases are relatively rare.
A decision regarding surgery is therefore difficult. Many patients have such extensive bilateral disease that surgery is out of the question. In others, symptoms are so mild and so easily controlled medically that the discomfort and slight risk of resection seem hardly justifiable. Between these extremes are many patients in whom the balance of decision is more even.44
The situation is little changed and the decisions are no easier. Surgical resection is generally only considered in those with localized disease and symptoms that are poorly controlled despite conventional therapy. However, resectional surgery may be considered for those with more extensive disease, if there are symptoms of poorly controlled bronchopulmonary suppuration with frequent exacerbations and if the majority of disease is resectable. Surgery may also be considered for those experiencing life‑threatening complications; for example, hemoptysis, unresponsive to or unsuitable for bronchial artery embolization, as long as the site of bleeding can be confidently identified. Other factors to consider when contemplating surgery are listed in Table 3. Although there are limited data, surgical resection for bronchiectasis is still associated with significant morbidity and mortality. In a recent large series45 of 53 patients undergoing surgical resection and in whom medical therapy was “unsuccessful,” there were 2 deaths (4%) and 25% experienced significant postoperative complications. There was no change in exercise capacity, but there was an improvement in quality of life which was greatest in those with the poorest preoperative quality of life. Thus, while the pendulum against surgical resection for bronchiectasis may have swung too far and while surgery may still have a role in selected patients, it is not without significant risk.
Questions to be addressed |
|
As indicated at the beginning, this article is not a comprehensive review of bronchiectasis and its management; rather, a few select topics have been discussed. For further and more detailed information, the reader is directed to other recent publications.1-4
- Hill AT, Sullivan AL, Chalmers JD, et al. British Thoracic Society guidelines for bronchiectasis in adults. Thorax. 2019; 74 (Suppl 1): 1‑69. | Crossref
- Polverino E, Geominne PC, McDonnell MJ, et al. European Respiratory Society guidelines for the management of adult bronchiectasis. Eur Respir J. 2017; 50: 1700629. | Crossref
- Boaventura R, Sibila O, Agusti A, Chalmers JD. Treatable traits in bronchiectasis. Eur Respir J. 2018; 52: 1801269. | Crossref
- Bell SC, Elborn JS, Byrnes CA. Bronchiectasis: treatment decisions for pulmonary exacerbations and their prevention. Respirology. 2018; 23: 1006‑1022. | Crossref
- Wells AU, Kolbe J. Bronchiectasis: a neglected cause of respiratory morbidity and mortality. Respirology 1996; 1: 221‑225. | Crossref
ARTICLE INFORMATION