Significant humoral response to mRNA COVID-19 vaccine in kidney transplant recipients with prior exposure to SARS-CoV-2: the COViNEPH Project



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Significant humoral response to mRNA COVID-19 vaccine in kidney transplant recipients with prior exposure to SARS-CoV-2: the COViNEPH Project
Introduction
Kidney transplant recipients (KTRs) are at an increased risk of SARS‑CoV‑2 infection, with mortality rates ranging from 13% to over 30%.1 In the absence of causal drugs against SARS‑CoV‑2, vaccination may improve the prognosis associated with COVID‑19 in KTRs.2 Despite limited information on the safety and immunogenicity of new mRNA vaccines in solid organ transplant recipients (SOTRs), both the European and the American Societies for Transplantation recommend vaccination. The Kidney Disease Improving Global Outcomes recommendations emphasize the importance of vaccinating patients prior to transplantation as vaccine immunogenicity is generally reduced in post‑transplant settings, and also some vaccines are more immunogenic when given before transplantation.3 However, due to the sudden outbreak of the COVID‑19 pandemic, the majority of SOTRs are vaccinated after transplantation. Initial immunogenicity studies in KTRs after a single dose of mRNA vaccine showed a weak immune response with seroconversion in anti‑S antibody of 10.8% and 17%.4,5 Recent studies indicate that seroconversion after 2 doses of mRNA vaccine in KTRs does not exceed 50%.6 These observations contrast with the strong immunogenicity of up to 100% observed in the general population.7 The results of our previous studies indicate that seroconversion is also observed in the vast majority of dialysis patients.8,9 More light on the immunogenetic potency of SARS‑CoV‑2 itself in comparison with vaccination has come from the studies in people with prior SARS‑CoV‑2 infection. The immune memory in convalescents may facilitate rapid and strong anamnestic antibody responses following re‑exposure to the virus or vaccination. Individuals from the general population previously infected with SARS‑CoV‑2 developed an antibody response after a single vaccine dose that was comparable or even stronger to that seen after the vaccination course in individuals without prior infections.10 To extend this knowledge, we conducted a study in KTRs and immunocompetent patients without kidney disease to compare the humoral response after BNT162b2 mRNA vaccine (Comirnaty, BioNTech/Pfizer) in COVID‑19 convalescents and individuals without a history of COVID‑19.
Patients and methods
Patient population
The study population comprised 149 KTRs (87 men [58.4%]) at a median (interquartile range [IQR]) age of 54 (43–63) years who were under the care of the University Clinical Center in Gdańsk, Poland, and 30 controls without chronic kidney disease (20 men [66.7%]) at a median (IQR) age of 49 (45–69) years, treated in the University Center of Maritime and Tropical Medicine in Gdynia, Poland.
Study design
This longitudinal study was performed to analyze the titer magnitude of immunoglobulin (Ig) G antibodies directed against S‑specific SARS‑CoV‑2 antigen after the second dose of the BNT162b2 mRNA vaccine in KTRs. KTRs were considered eligible if they were at least 1 month after transplantation and had received vaccination with BNT162b2 with a 6‑week interval between the first and second dose from March 8 to May 19, 2021. Control patients (estimated glomerular filtration rate >60 ml/min/1.73 m2) were vaccinated for COVID‑19 with the same vaccine and schedule as the KTRs.
Stratification based on the evidence of previous COVID‑19 divided the KTR cohort into an infection‑naïve group (n = 103) without a history of COVID‑19 and negative results for nucleocapsid (N)-specific antibodies (KTR[–]) a and previously infected group (n = 46; KTR[+]). The control groups included 15 infection‑naïve patients with no history of COVID‑19 and negative results for N‑specific antibodies (CONTROL[–]) and 15 previously infected controls (CONTROL[+]). Serum samples for the measurment of antibody titer were obtained before the first and 14 to 21 days following the second dose of BNT162b2.
Ethics approval for the study was obtained at the Medical University of Gdansk (NKBBN/167/2021).
Details regarding the measurement methods of anti–SARS‑CoV‑2 antibodies and statistical analysis are provided in Supplementary material (Anti–SARS‑CoV‑2 antibodies measurement and Statistical analysis sections, respectively).
Results
Patient characteristics are described in Supplementary material (Patient characteristics section and Table S1).
Infection‑naïve groups of kidney transplant recipients and controls
S‑specific immune response with a median (IQR) antibody IgG titer of 82 (31.2–172) AU/ml was seen in 49 patients from the KTR(–) group (47.6%). In 12 individuals (11.65%), humoral response with a titer above 200 AU/ml was observed. Patients from the KTR(–) group who responded to vaccination had a significantly lower titer of antibody as compared with previously infected KTRs and both control groups (Kruskal–Wallis H test; P <0.001) (Supplementary material, Table S2).
In 54 patients from the KTR(–) group (52.4%; 28 men [51.8%]), S‑specific seroconversion was not found. KTR(–) nonresponders were older than the responders, with a median (IQR) age of 58.5 (50–67) years versus 49 (40–61) years (P = 0.013). All patients from the CONTROL(–) group (n = 15) responded to vaccination with a titer above 200 AU/ml (median [IQR] S‑antibody titer was 800 [782–1670] AU/ml).
Previously infected groups of kidney transplant recipients and controls
In the KTR(+) group, the median S‑antibody titer before vaccination was 36.6 (10.7–107) AU/ml and it was not different from that in the CONTROL(+) group (33.5 [18.4–144] AU/ml). All patients in the KTR(+) group responded to vaccination, with a median antibody titer of 540 (351–752) AU/ml. The postvaccination S‑antibody titer was more than 6‑fold higher than in KTR(–) responders but almost 4‑fold lower than in previously infected controls (Kruskal–Wallis H test; P <0.001). In 42 patients from the KTR(+) group (91.3%), the titer was above 200 AU/ml.
All individuals from the CONTROL(+) group (n = 15) responded to the vaccine, with a median (IQR) antibody titer of 2060 (1250–3230) AU/ml (Supplementary material, Table S2). The kinetics of S‑antibody IgG titer in all groups are presented in Figure 1.
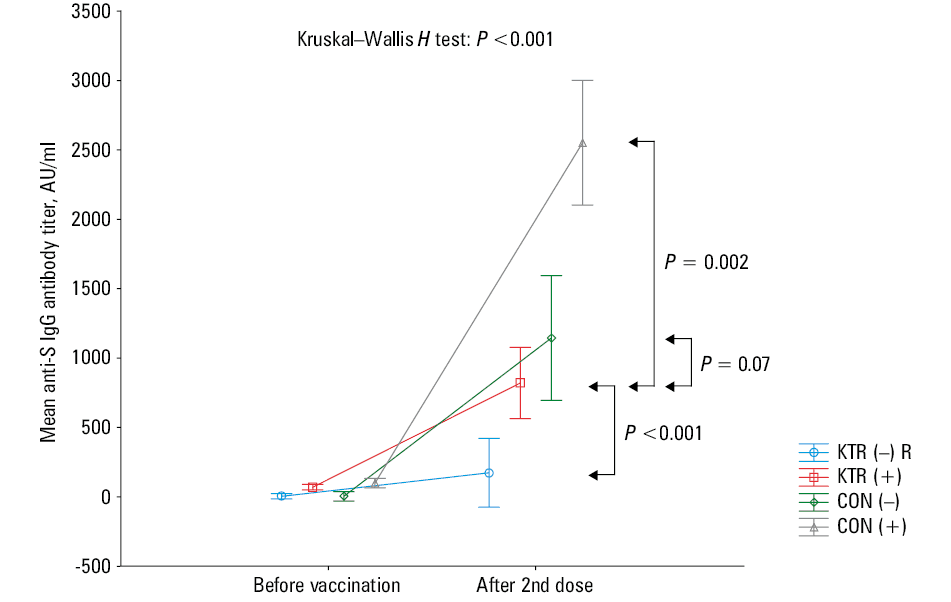
Abbreviations: CON(–), infection‑naive controls; CON(+), previously infected controls; KTR(–), infection‑naive kidney transplant recipients; KTR(+), previously infected kidney transplant recipients; R, responders
Discussion
Many questions have been raised after the first reports on low humoral response to vaccination in KTRs without prior exposure to the virus as well as vaccine breakthrough infections in vaccinated KTRs.6,11 Unlike the breakthrough cases reported in the general population, KTRs in a large percentage developed severe COVID‑19 requiring hospitalization and mechanical ventilation.12 Such limited humoral response in COVID‑19–naïve patients seems an obvious consequence of immunosuppressive therapy, and impaired antibody response after vaccinations in KTRs is a well‑known fact.3 The potential strategies for improving vaccine immunogenicity in KTRs include: 1) alternative vaccination regimens, with an additional third dose of the vaccine;13 and 2) modulation of immunosuppression (antiproliferative agents correlate with the lack of an antibody response).6 Better humoral response to vaccination in KTRs with a history of COVID‑19 was observed by Firket et al14 in a small‑size study. The seroconversion was obtained in 1 out of 10 KTRs without a history of infection and 10 out of 10 previously infected KTRs. The magnitude of serological response was not different between the KTR(+) and CONTROL(+) groups. To shed more light on this issue, we carried out a longitudinal study in a cohort of KTRs vaccinated with BNT162b2 and respective controls. We confirmed a weak humoral response after vaccination in COVID‑19–naïve individuals, among whom only 47.6% achieved seroconversion. Moreover, the magnitude of response to vaccination was much lower as compared with immunocompetent controls. We noticed an approximately 10% higher seroconversion rate than that reported by Grupper et al,6 who demonstrated that over 60% of KTRs did not respond to vaccination. Our results resemble those achieved by heart and liver transplant recipients vaccinated with BNT162b2,7 and also those published by Boyarsky et al5 and Benotmane et al13 in KTRs vaccinated with BNT162b2 or mRNA‑1273.
The kinetics of humoral response in COVID‑19 convalescents in our study presented a different picture. The median antibody titer before vaccination in the KTR(+) group did not differ from that observed in the CONTROL(+) group, and all previously infected KTRs responded to the vaccine with a significant increase in antibody titer. The increase was more than 6‑fold higher than in the KTR(–) responders. Moreover, 91.3% of individuals in the KTR(+) group developed a strong humoral response, with an antibody titer above 200 AU/ml. The data presented previously by Firket et al14 and confirmed by us, show that natural exposure to the virus seems to be a stronger stimulus than vaccination in terms of the formation of immunological memory and production of antibodies upon repeated contact with the antigen (reaction to vaccination). A longer follow‑up is needed to investigate further kinetics of humoral response among all strata of patients. It is also unknown whether naturally gained immunity surpasses that achieved after vaccination.
The results of our study also point to a practical aspect in selecting a vaccine for KTRs. The vaccines which are actually used in SOTRs are recombinant protein vaccines and sometimes vector‑based vaccines. Because the recombinant protein vaccines use only a protein fragment of RBD as the antigen, this type of vaccine may have lower immunoreactivity than the whole‑pathogen vaccine candidates such as VLA2001 or CoronaVac. Development of new types of vaccines could lead to a highly potent neutralizing antibody response, as well as the cross‑protection against other strains of SARS.
The limitation of our study is the small sample size, which did not allow for stratified analyses to identify factors of a better response other than preimmunization by the virus itself, such as comorbidity and particular immunosuppressive protocols. Performing only a humoral analysis does not allow for a full description of the immunological response to both the disease and vaccination. Simultaneous analysis of cellular immunity mostly affected by immunosuppression could shed more light on predicting the risk of disease in patients without a desirable response to vaccination, and may allow individualized management. It is unknown if seronegative patients develop a sufficient cellular response that could offer a certain grade of protection against SARS‑CoV‑2. Cucchiari et al15 studied simultaneously humoral and cellular response in KTRs and kidney‑pancreas recipients after mRNA‑1273, and observed that the rate of naïve patients who finally developed either humoral or cellular response was 65%, of whom 29.9% developed either IgG or IgM and 35%, S‑enzyme–linked immunospot positivity. This finding highlights the fact that patients may be protected against SARS‑CoV‑2 despite the absence of antibodies since a strong T‑cell response is part of the consequences of SARS‑CoV‑2 infections and seems to play an important role in terms of long‑term immunological memory. To what extent the cellular immunity, in the absence of detectable antibodies, is able to prevent severe infection in KTRs is yet to be determined.
In summary, we would like to underline that only half of KTRs achieved seroconversion after BNT162b2. A history of COVID‑19 in KTRs impacted not only the humoral response to the BNT162b2 vaccination but also its magnitude. The results prove that exposure to the virus (the whole particle of pathogen) is a stronger stimulus than vaccination in terms of the formation of immunological memory and production of antibodies upon repeated contact with the antigen. The weak response to mRNA vaccine, as compared with SARS‑CoV‑2 infection, suggests that other types of already accessible vaccines, or a different schedule of vaccination, should be taken into consideration in this patient population.
- Azzi Y, Bartash R, Scalea J, et al. COVID‑19 and solid organ transplantation: a review article. Transplantation. 2021; 105: 37‑55. | Crossref
- Kędzierska‑Kapuza K, Zielińska D, Matejak‑Górska M, et al. The course of SARS‑CoV‑2 in a patient after a recent kidney transplant: a literature review on COVID‑19 therapy. Transplant Proc. 2021; 53: 1194‑1201. | Crossref
- Chadban SJ, Ahn C, Axelrod DA, et al. KDIGO clinical practice guideline on the evaluation and management of candidates for kidney transplantation. Transplantation. 2020; 104: S11‑S103. | Crossref
- Benotmane I, Gautier‑Vargas G, Cognard N, et al. Weak anti‑SARS‑CoV‑2 antibody response after the first injection of an mRNA COVID‑19 vaccine in kidney transplant recipients. Kidney Int. 2021; 99: 1487‑1489. | Crossref
- Boyarsky BJ, Werbel WA, Avery RK, et al. Immunogenicity of a single dose of SARS‑CoV‑2 messenger RNA vaccine in solid organ transplant recipients. JAMA. 2021; 325: 1784‑1786. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION