Current applications and outcomes of venoarterial extracorporeal membrane oxygenation based on 6 years of experience: risk factors for in‑hospital mortality
Key words: cardiogenic shock, extracorporeal membrane oxygenation, heart failure, mechanical circulatory support



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Current applications and outcomes of venoarterial extracorporeal membrane oxygenation based on 6 years of experience: risk factors for in‑hospital mortality
Introduction: Data regarding venoarterial extracorporeal membrane oxygenation (VA ECMO) as a temporary circulatory support in cardiogenic shock (CS) for Central Europe are scarce.
Objectives: The aim of the study was to disclose indications, in‑hospital, and long‑term (1‑year) mortality along with risk factors.
Patients and methods: The study is a retrospective investigation of patients who underwent VA ECMO for CS at a cardiosurgical tertiary center, from January 2013 to June 2018. A broad spectrum of pre- and postimplantation factors was tested using univariable analysis.
Results: A total of 198 patients met the inclusion criteria. The median (interquartile range) duration of support was 207 (91–339) hours, with no significant disparity among hospital survivors and nonsurvivors (P = 0.09). A total of 40.4% of patients died during ECMO support, while the joined in‑hospital and 6‑month mortality progressed to 65.2%, and 1‑year mortality to 67.2%; 9% underwent a subsequent heart transplantation. Main adverse events were bleeding (76%), infection (56%), neurologic injury (15%), and limb ischemia (15%). Multiorgan failure was the most decisive risk factor of in‑hospital mortality (odds ratio, 4.45; P <0.001). Patients with postcardiotomy CS had a significantly lower out‑of‑hospital survival rate than the nonsurgical group (32.3% vs 45%; log‑rank P = 0.037).
Conclusions: The study showed survival benefit, despite frequent complications. The protocol focusing on proper candidate selection and timing can positively impact patient survival. Additional risk reduction can be achieved with a further increase of the team experience with ECMO.
What's new?
What‘s new?
Venoarterial extracorporeal membrane oxygenation (VA ECMO) is increasingly used to provide temporary mechanical circulatory support as a salvage therapy for patients in cardiogenic shock or cardiac arrest refractory to usual medical treatment. However, data about the frequency of VA ECMO in Poland are scarce. We analyzed the real‑life use of VA ECMO therapy, based on 6 years of experience of a Polish cardiosurgical tertiary center, and demonstrated satisfactory outcomes.
Introduction
Venoarterial extracorporeal membrane oxygenation (VA ECMO) is an applicable treatment option in the setting of refractory cardiogenic shock (CS), a condition related to soaring rates of mortality. The trend to use VA ECMO as acute cardiopulmonary life support is progressing worldwide. However, due to the remarkably challenging clinical scenarios, the available data regarding its applicability, complications, and outcome are insufficient. Therefore, according to the European Society of Cardiology guidelines, its use could be considered (class IIb recommendation) with the lowest possible level of evidence (C).1 The need for more robust data is even more apparent for the Central and Eastern European population, as most evidence for guidance in the ECMO therapy originates from population‑based studies performed in Western European and North American hospitals. As the differences in healthcare organization and budgets are undeniable, epidemiology and outcomes in patients with CS, particularly in such a costly and resource‑intensive technology as VA ECMO, should be provided separately for the Central and Eastern European population. To our knowledge, we present results of the largest retrospective VA ECMO study based in Central and Eastern Europe.
Objectives
This study aimed to identify the frequency of use of ECMO in patients of our cardiac and cardiosurgical tertiary center in Poland. We focused on providing the clinical characterization of hospital survivors versus nonsurvivors among patients undergoing VA ECMO at our center, the feasibility of therapy, the occurrence of significant adverse events, and the outcome (in‑hospital and long‑term [12 months after ECMO implantation] mortality).
Patients and methods
The study was conducted after the approval by the local ethics committee. The project was a single‑center, retrospective study. We included all consecutive patients who underwent VA ECMO support for refractory CS at the National Institute of Cardiology, Warsaw, Poland, from January 2013 to June 2018.
There is no clear and unified protocol for ECMO support at our center. Hence, the choice of initiating ECMO is to be made by the Heart Team, including a cardiac surgeon, an anesthesiologist, a cardiologist, and an intensivist on the basis of commonly accepted criteria of recognition and treatment of CS.1 The main decisive factors for the use of VA ECMO include progressing hemodynamic instability (systolic blood pressure <90 mm Hg, pulmonary capillary wedge pressure >20 mm Hg), tissue hypoperfusion (oliguria, cool extremities, altered mental status), and organ damage (rising creatinine and liver transaminases), following decreased cardiac output (cardiac index below 1.8 l/min/m2) despite optimal pharmacological therapy. VA ECMO is also implanted in the case of inability to wean from cardiopulmonary bypass after heart surgery. In any case, VA ECMO is used if later recovery, heart transplantation, or long‑term mechanical circulatory support (MCS) is probable.
Data collection
Data were extracted from medical records and deidentified. The records included patients’ demographic characteristics, pre- and postimplantation clinical parameters, laboratory results, and imaging data.
Definitions
Baseline medical history refers to comorbidities present before the hospitalization during which ECMO was used. The pre‑ECMO data set included the latest laboratory analysis and clinical parameters preceding ECMO implantation. On‑ECMO set contains values gathered approximately 12 to 24 hours after ECMO initiation. Preweaning relates to the last examination before the weaning from ECMO (up to 24 hours). Diagnosis and classification of coronary artery disease, diabetes, heart failure, and the probability of pulmonary hypertension were made in adherence to the corresponding European Society of Cardiology guidelines.2-5 Right ventricular (RV) dysfunction was defined as presence of more than a single parameter from the following: RV fractional area change of less than 35%, tricuspid annular plane systolic excursion of less than 16 mm, and the S’ parameter on tissue Doppler imagining of the tricuspid annulus of less than 10 cm/s with RV muscle hypo-/akinesis on echocardiography.6 Renal impairment was defined as glomerular filtration rate below 50 ml/min and no dialysis. Dialysis was defined as dialysis‑dependency before ECMO implantation, either in chronic (on‑line intermittent renal replacement therapy [RRT]) or acute / acute on chronic kidney disease during the current medical event (continuous RRT). Multiorgan failure was defined as an admission to the intensive care unit and requirement for the support of 2 or more organ systems, with or without mechanical ventilation. Cardiopulmonary resuscitation (CPR) was defined as the need for a minimum of 1 minute of chest compressions for sudden cardiac arrest (SCA) that occurred up to 12 hours before ECMO initiation. Bleeding complications were assessed according to the Bleeding Academic Research Consortium definitions.7 The implementation of the ECMO circuit was either peripheral or central. Peripheral cannulation was performed via the femoral or subclavian artery, in most cases with surgical exposure of the cannulated vessels and additional placement of a distal cannula into the superficial femoral artery or graft anastomosis to the common femoral artery for ischemia prevention on the side of the cannulated leg. Central cannulation was performed surgically via sternotomy with graft anastomosis to the ascending aorta and inflow cannula deriving blood from the right atrium. Hybrid cannulation was defined as a central positioning of the outflow cannula and peripheral inflow placement.
Anticoagulation is routinely initiated in the first 12 to 24 hours after ECMO implantation in the absence of life‑threatening bleeding complications. Normally, continuous unfractionated heparin infusion rate ranges from 10 to 50 U/kg/h and is adjusted every 6 to 8 hours according to the activated partial thromboplastin time measurement to target in between 50 and 90 seconds. In addition, fibrinogen and D‑dimer levels as well as platelet counts are analyzed at least once daily, while anti–factor Xa and antithrombin III levels are measured occasionally for detailed assessment of the patient’s coagulation. The anticoagulation regimen and anticoagulation monitoring range are individualized in every case, following the patient’s estimated thrombotic and bleeding risk profile.
Statistical analysis
Descriptive analysis was conducted to provide pre‑ECMO, on‑ECMO, and post‑ECMO variables and to detect disparities between hospital survivors and nonsurvivors. Categorical variables were given as numbers and percentages, and further analyzed with the Pearson χ2 test. Continuous variables were expressed as medians and interquartile ranges (IQRs) according to their distribution and examined with the Mann–Whitney test. Univariable logistic regression was used to assess the impact of specific pre‑ECMO, on‑ECMO, and post‑ECMO variables on the probability of in‑hospital mortality. Statistical significance was set at 0.05 for hypotheses tested. Cumulative survival curves for 1‑year follow‑up were created using the Kaplan–Meier method. The surgical and nonsurgical groups were compared using the log‑rank test. Data collection was managed with the Microsoft Excel software. For statistical analyses, IBM SPSS Statistics 27 (Chicago, Illinois, United States) was used.
Results
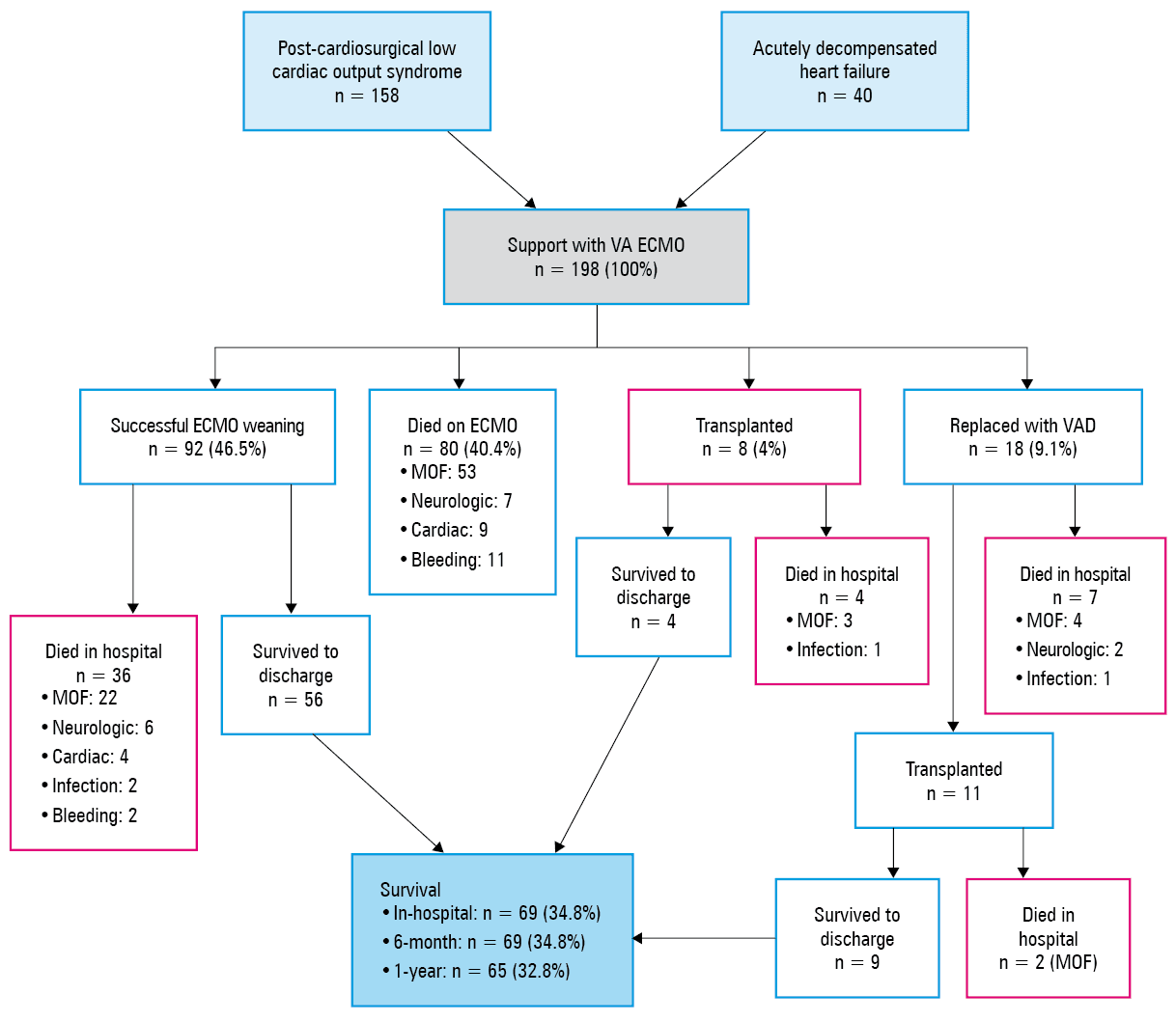
Between 2013 and 2018, 198 patients received venoarterial ECMO support for severe CS refractory to standard pharmacological therapy (Figure 1). No patient was lost to 12‑month follow‑up.
The leading causes of cardiocirculatory pathology were valvular heart disease (39%), ischemic cardiomyopathy (31%), and dilated cardiomyopathy (14%). Over half of patients had a history of arterial hypertension (57%) and dyslipidemia (52%), which were the most common comorbidities among many other noted (Supplementary material, Figure S1).
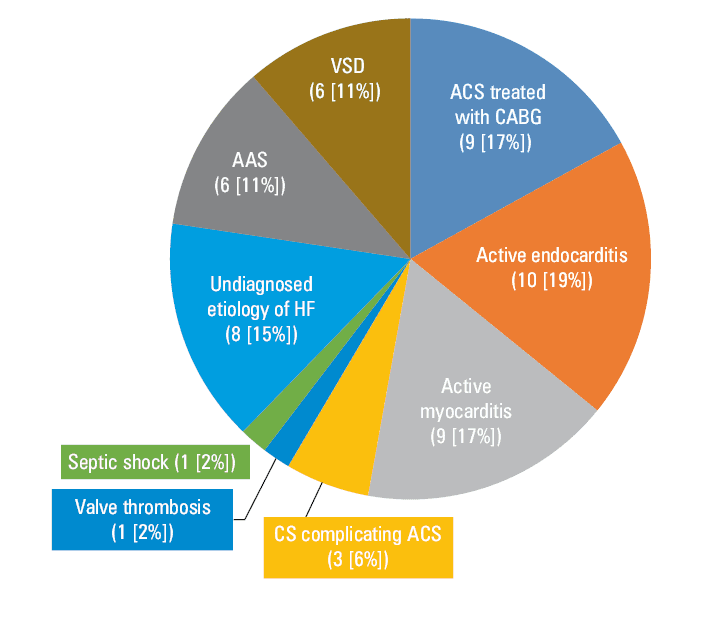
Slightly above one‑fourth (27%) of patients without prior history of cardiovascular pathology required urgent MCS or surgery for de novo injury of the heart or great vessels (Figure 2), and 16% of all patients experienced SCA up to 12 hours before ECMO implantation. The majority of the cohort (79.8%) comprised surgical patients, and one‑fifth (20.2%) underwent ECMO support without preceding cardiac surgery. Specific indications for ECMO implantation are presented in Figure 3. Further meticulous analysis was performed considering in‑hospital survivors and nonsurvivors. Significant pre‑ECMO hospitalization and clinical data in relation to in‑hospital mortality for the entire cohort, with distinction to hospital survivors and hospital nonsurvivors, are provided in Table 1.
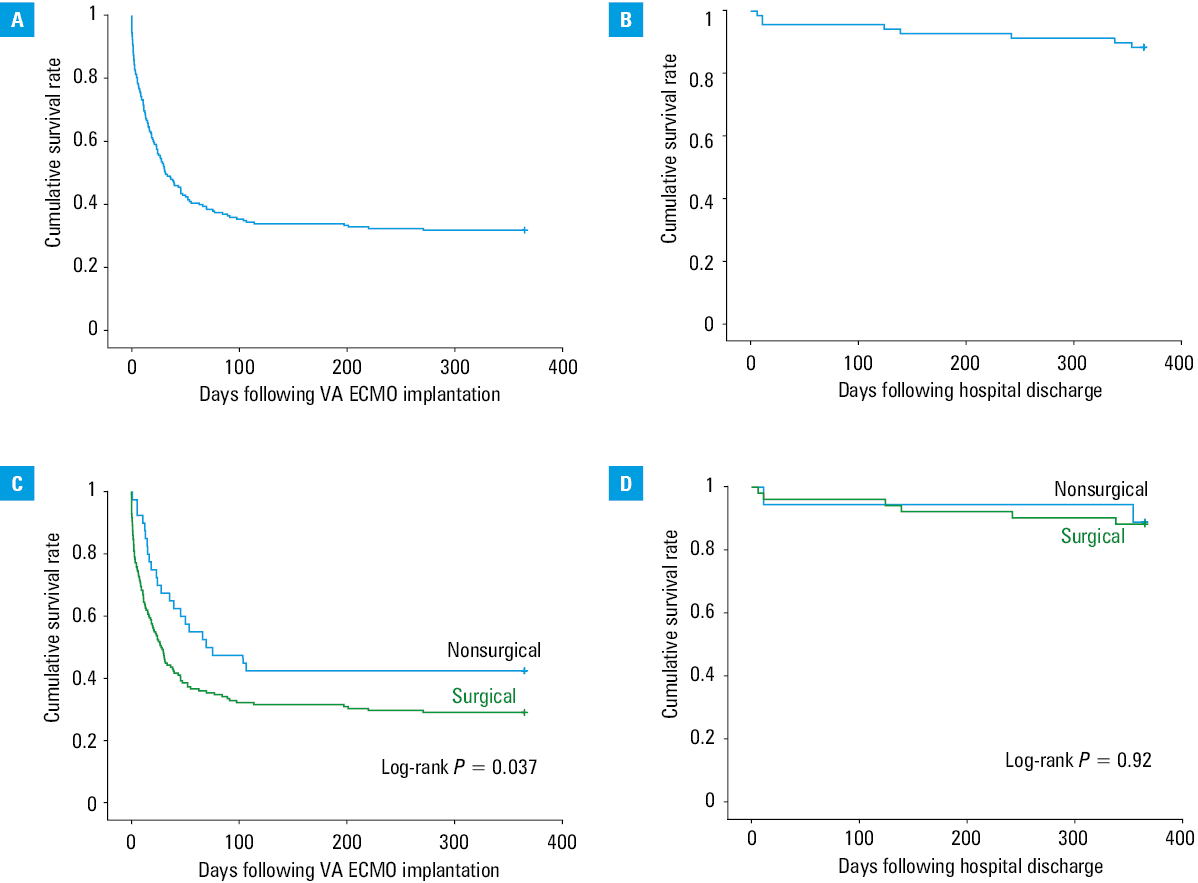
![Kaplan–Meier survival curves for overall survival following ECMO implantation (A) and hospital discharge (B). Mortality was the highest following ECMO implantation during hospitalization (survival rate, 34.8%), while survival remained stable following discharge to one-year follow up (survival rate, 94.2%). C, D – Kaplan–Meier survival curves stratified according to groups of indication (postcardiotomy [C] vs cardiogenic shock [D]). Patients with postcardiotomy cardiogenic shock had a significantly lower out-of-hospital survival rate than those with decompensated heart failure (32.3% vs 45%, C). No difference in 1-year survival between groups was noted following discharge (D).Abbreviations: see Figure 1](/paim/_next/image/?url=https%3A%2F%2Fpamw.pl%2Fsites%2Fdefault%2Ffiles%2Fjson_zip_files%2Funcompressed%2F16145%2FIMAGES%2FKP_WEB__FIG_03.png&w=3840&q=75)
Variables | MD (%) | All (n = 198) | Survivors (n = 69) | Nonsurvivors (n = 129) | P value | ULR | ||
OR (95% CI) | P value | |||||||
Categorical variables are presented as numbers (percentages) and were compared with the χ2 test. Continuous variables are presented as median (interquartile range; range) and were compared with the Mann–Whitney test.
Abbreviations: CKD, chronic kidney disease; CRRT, continuous renal replacement therapy, IDDM, insulin‑dependent diabetes mellitus; MD, missing data; OR, odds ratio; RRT, renal replacement therapy; SCA, sudden cardiac arrest; ULR, univariable logistic regression; others, see Figure 1 | ||||||||
Age, y | 0 | 58.7 (42.9–65.1; 9.2–84.6) | 56 (34.2–62.8; 9.2–79.8) | 60.3 (50.1–66.8; 12.6–84.6) | 0.007 | 1.025 (1.007–1.044) | 0.007 | |
Male sex | 0 | 131 (66) | 43 (62) | 88 (68) | 0.4 | 1.298 (0.704–2.393) | 0.40 | |
Body weight, kg | 30 | 78 (65–88; 41–125) | 80 (65–90; 41–125) | 75 (65–85.75; 43–120) | 0.16 | 0.983 (0.963–1.004) | 0.11 | |
IDDM | 0 | 12 (6) | 1 (1) | 11 (9) | 0.045 | 6.393 (0.80–50.605) | 0.08 | |
CKD | 0 | 78 (39) | 26 (38) | 52 (40) | 0.003 | 1.117 (0.613–2.037) | 0.72 | |
CRRT | 0 | 15 (8) | 3 (4) | 12 (9) | 0.02 | 2.256 (0.615–8.285) | 0.22 | |
Bleeding diathesis | 0 | 12 (6) | 1 (1) | 11 (9) | 0.045 | 6.393 (0.80–50.605) | 0.08 | |
SCA before ECMO implantation | 0 | 32 (16) | 11 (16) | 21 (16) | 0.95 | 4.454 (2.272–8.732) | <0.001 | |
Admission to ECMO interval, d | 0 | 3.6 (1.7–16.7; 0.1–234) | 2.4 (1.4–7.2; 0.4–184) | 4.2 (1.8–24.8; 0.1–234.9) | 0.003 | 1.02 (0.462–2.273) | 0.95 | |
Surgery to ECMO interval, d | 0 | 0 (0–1.9; 0–63.18) | 0 (0–1.04; 0–4.7) | 0.3 (0–2.21; 0–63.18) | 0.17 | 1.0111 (0.998–1.024) | 0.09 | |
Cannulation | Peripheral | 0 | 91 (46) | 31 (45) | 60 (47) | 0.85 | – | – |
Central | 66 (33) | 20 (29) | 46 (36) | 0.22 | – | – | ||
Hybrid | 41 (21) | 17 (25) | 24 (19) | 0.34 | – | – | ||
Pre‑ECMO stage
The median (IQR) age was 58.7 (42.9–65.1) years, and hospital survivors were younger than nonsurvivors (median [IQR], 55.8 [43.2–62.8] vs 60.3 [50.1–66.8] years; P = 0.007). Among concomitant conditions, insulin‑dependent diabetes mellitus, chronic kidney disease with glomerular filtration rate below 50 ml/min or dialysis dependent, and bleeding diathesis were significantly more frequent among hospital nonsurvivors compared with survivors. The interval from hospital admission to ECMO implantation was significantly shorter in hospital survivors as opposed to nonsurvivors (median [IQR], 2.4 [1.4–7.2] days vs 4.2 [1.8–24.8] days; P = 0.003). When analyzing preimplantation echocardiographic parameters, a significant increase in mortality risk was shown for those with intermediate or high probability of pulmonary hypertension, whereas left ventricular ejection fraction (LVEF) and the prevalence of valvular pathologies were comparable between survivors and nonsurvivors. Of various laboratory parameters examined, nonsurvivors had significantly lower hemoglobin and higher activated partial thromboplastin time values in comparison with survivors. Among various pre‑ECMO variables, 4 were associated with in‑hospital mortality by univariable logistic regression: age, developed multiorgan failure, receiving oral anticoagulants up to 7 days before ECMO initiation, and hemoglobin level. The significant variables preceding ECMO implantation are detailed in Table 1 and Supplementary material, Table S1.
On‑ECMO period
The median duration of mechanical ventilation to first extubation and total mechanical ventilation was significantly longer in nonsurvivors than in survivors. Furthermore, those who died in hospital were significantly less frequently extubated on ECMO, more often needed reintubation and tracheostomy, and had lower Glasgow Coma Scale (GCS) score assessed at extubation compared with survivors. Nonsurvivors significantly more frequently experienced acute kidney injury (AKI) with the need for RRT. With regard to blood tests, low platelet count, elevated international normalized ratio (INR), and lactate levels were important prognostic factors. Unloading of the LV alongside ECMO was implemented in 80 patients (40%) as intra‑aortic balloon counterpulsation (n = 62), LV venting cannula (n = 11), or the Rashkind procedure (n = 7). In univariable logistic regression, a significant association with in‑hospital mortality was further confirmed for lower GCS score at extubation, longer total mechanical ventilation time, the need for reintubation, and AKI with the need for RRT. Significant data related to on‑ECMO period are shown in Table 2.
Variables | MD (%) | All (n = 198) | Survivors (n = 69) | Nonsurvivors (n = 129) | P value | ULR | |
OR (95% CI) | P value | ||||||
Categorical variables are presented as numbers (percentages) and were compared with the χ2 test. Continuous variables are presented as median (interquartile range; range) and were compared with the Mann–Whitney test.
| |||||||
Mechanical ventilation | |||||||
GCS after extubation | 0 | 15 (14–15; 3–15) | 15 (14–15; 12–15) | 14 (14–15; 12–15) | 0.001 | 0.838 (0.689–1.020) | 0.08 |
Extubation on ECMO | 0 | 110 (56) | 60 (87) | 50 (39) | <0.001 | 0.106 (0.048–0.232) | <0.001 |
MV time to extubation, h | 0 | 45 (24–121; 2–918) | 29 (18–51; 6–267) | 65 (29–160; 2–918) | <0.001 | 1.007 (1.003–1.011) | 0.001 |
Total MV time, h | 0 | 68 (29–217; 2–1842) | 35 (19–78; 6–645) | 120 (40–286; 2–1842) | <0.001 | 1.006 (1.003–1.009) | <0.001 |
Re‑intubation on ECMO | 0 | 46 (23) | 12 (17) | 34 (26) | <0.001 | 4.093 (1.870–8.958) | <0.001 |
Tracheostomy | 0 | 15 (8) | 0 | 15 (12) | 0.003 | – | – |
Hemodiafiltration | |||||||
CRRT | 0 | 94 (47) | 24 (35) | 70 (54) | 0.004 | 2.431 (1.321–4.471) | 0.004 |
Unloading LV | |||||||
IABP | 0 | 62 (31) | 28 (41) | 34 (26) | 0.06 | 0.547 (0.294–1.018) | 0.06 |
LV vent | 0 | 11 (6) | 3 (4) | 8 (6) | 0.56 | 1.492 (0.383–5.815) | 0.57 |
Rashkind procedure | 0 | 7 (4) | 4 (6) | 3 (2) | 0.23 | 0.4 (0.087–1.840) | 0.24 |
Echocardiographic parameters | |||||||
LVEF, % | 2 | 15 (10–20; 5–65) | 15 (10–20; 5–60) | 15 (10–20; 5–65) | 0.41 | 0.995 (0.972–1.019) | 0.7 |
RV dysfunction | 4 | 53 (28) | 16 (25) | 37 (29) | 0.723 | 0.877 (0.424–1.813) | 0.72 |
Laboratory parameters | |||||||
Platelet count, × 1000/µl | 3 | 89.5 (67–134; 7.2–455) | 95 (73–146; 25–455) | 85.5 (58–123; 7.2–266) | 0.025 | 0.994 (0.989–0.999) | 0.026 |
Lactate, mmol/l | 10 | 3.3 (2–10.4; 0.33–27.5) | 2.71 (1.7–4.86; 0.33–15.9) | 5 (2.3–11.7; 1–27.5) | 0.001 | 1.125 (1.041–1.216) | 0.003 |
INR | 2 | 1.47 (1.27–1.87; 1.03–6.24) | 1.35 (1.23–1.6; 1.04–3.34) | 1.57 (1.37–1.99; 1.03–6.24) | <0.001 | 3.639 (1.591–8.325) | 0.002 |
Weaning from ECMO
Ninety‑two patients (46.5%) were successfully weaned from ECMO. Patients who later died in hospital had significantly lower LVEF and arterial pH on the last examination before weaning. Nonsurvivors were also identified to have significantly higher values of creatinine, aspartate aminotransferase, INR, and arterial lactate concentrations in the final analysis before ECMO withdrawal. Univariable logistic regression testing confirmed the association of in‑hospital mortality with elevated creatinine, bilirubin, aspartate aminotransferase, INR, and arterial lactate levels, as well as lower values of LVEF and arterial pH. Data from the preweaning analysis are presented in Supplementary material, Table S2.
Complications
The most frequent adverse events associated with ECMO were bleeding (76%), infection (56%), neurologic injury (15%), and limb ischemia (15%). In patients with hemorrhage, the occurrence of life‑threatening or major bleeding7 and the need for the associated resurgery were significantly more frequent in nonsurvivors than in survivors. Moreover, nonsurvivors significantly more often bled from the postsurgical site as well as the ear‑nose‑throat area and gastrointestinal tract, and more often had stroke, intracranial hemorrhage, limb ischemia, and fungal infection compared with survivors. Among complications during the course of ECMO, 8 variables were significantly associated with in‑hospital mortality in univariable logistic regression analysis: episodes of life‑threatening or major bleeding, bleeding from the postcardiosurgical site, ear‑nose‑throat area, or lower respiratory, and gastrointestinal tract, fungal infection, and limb ischemia. Data concerning complications occurring during the ECMO therapy are presented in Table 3.
Variables | All (n = 198) | Survivors (n = 69) | Nonsurvivors (n = 129) | P value | ULR | ||
OR (95% CI) | P value | ||||||
Categorical variables are presented as numbers (percentages) and were compared with the χ2 test. Continuous variables are presented as median (interquartile range; range) and were compared with the Mann–Whitney test.
| |||||||
Bleeding adverse event | |||||||
Bleeding incident type | Overt bleeding episode | 151 (76) | 48 (70) | 103 (80) | 0.105 | 1.733 (0.887–3.385) | 0.11 |
Life‑threatening or disabling bleeding episode | 101 (51) | 24 (35) | 77 (60) | <0.001 | 2.946 (1.599–5.430) | 0.001 | |
Major bleeding | 79 (40) | 18 (26) | 61 (47) | 0.002 | 2.323 (1.260–4.283) | 0.007 | |
Minor bleeding | 76 (38) | 26 (38) | 50 (39) | 0.78 | 1.088 (0.595–1.990) | 0.78 | |
Resurgery due to bleeding | 76 (38) | 23 (33) | 53 (41) | 0.23 | 1.56 (0.864–2.818) | 0.14 | |
Bleeding location | ECMO cannulation site | 88 (44) | 27 (39) | 61 (47) | 0.23 | 1.447 (0.795–2.635) | 0.23 |
Surgical site | 84 (42) | 20 (29) | 64 (50) | 0.003 | 2.529 (1.352–4.732) | 0.004 | |
Tamponade | 39 (20) | 17 (25) | 22 (17) | 0.231 | 0.647 (0.316–1.323) | 0.23 | |
Ear, nose, throat | 26 (13) | 3 (4) | 23 (18) | 0.006 | 4.913 (1.419–17.013) | 0.012 | |
Urinary tract | 11 (6) | 1 (1) | 10 (8) | 0.06 | 5.862 (0.734–46.797) | 0.09 | |
Pleural space | 23 (12) | 8 (12) | 15 (12) | 0.949 | 1.03 (0.413–2.568) | 0.95 | |
Lower respiratory tract | 20 (10) | 2 (3) | 18 (14) | 0.012 | 5.583 (1.255–24.832) | 0.024 | |
Gastrointestinal tract | 24 (12) | 2 (3) | 20 (16) | 0.041 | 3.066 (1.003–9.369) | 0.049 | |
Hemoptysis | 6 (3) | 2 (3) | 4 (3) | 0.915 | 1.098 (0.196–6.154) | 0.92 | |
Neurologic injury | |||||||
Ischemic stroke | 20 (10) | 3 (4) | 17 (13) | 0.044 | 3.431 (0.969–12.155) | 0.06 | |
ICH | 9 (5) | 0 | 9 (7) | 0.023 | – | – | |
Infection | |||||||
Infection | 112 (57) | 38 (55) | 74 (57) | 0.62 | 1.161 (0.642–2.099) | 0.62 | |
Microbiological confirmation | 56 (28) | 17 (25) | 39 (30) | – | – | – | |
Fungal etiology | 14 (7) | 1 (1) | 13 (10) | 0.019 | 8.141 (1.039–63.786) | 0.046 | |
Localization of infection | Most common etiology | ||||||
Blood bacteriemia | 39 (20) | Staphylococcus spp, Klebsiella spp | |||||
Pneumonia | 19 (10) | Klebsiella spp, Staphylococcus spp, Pseudomonas spp | |||||
ECMO insertion site | 7 (4) | Klebsiella spp, Enterococcus spp | |||||
Postsurgical site | 7 (4) | Staphylococcus spp, Enterococcus spp | |||||
Diarrhea | 4 (2) | Clostridium difficile | |||||
Urinary tract | 3 (2) | Escherichia spp, Enterococcus spp | |||||
Peripheral ischemic adverse events | |||||||
Limb ischemia | 30 (15) | 3 (4) | 27 (21) | 0.001 | 6.061 (1.766–20.798) | 0.004 | |
Limb amputation | 5 (3) | 1 (1) | 4 (3) | 0.46 | 2.248 (0.246–20.519) | 0.47 | |
Peripheral thrombosis / embolization | 6 (3) | 3 (4) | 3 (2) | 0.44 | 0.533 (0.105–2.715) | 0.45 | |
Outcome
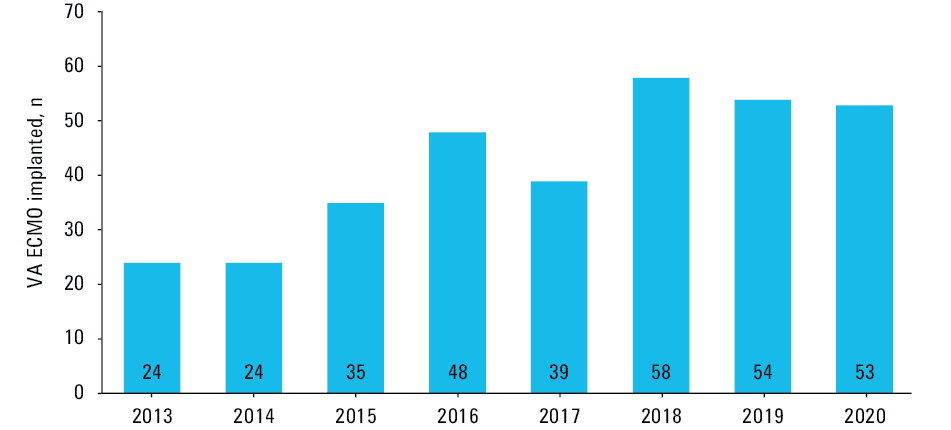
No patient was lost to 12‑month follow‑up. In‑hospital mortality was 65.2% (129 patients). As many as 80 patients (40.4%) died during ECMO, and 36 (18%) after the weaning from ECMO. Multiorgan failure was the most frequent cause of death (64%), followed by insufficient cardiac regeneration (12%), neurologic impairment (11%), fatal bleeding (10%), and infection (3%). The median (IQR) duration of ECMO was 207.2 (91.1–339.4) hours, with no significant disparity in the length of support among the 2 subgroups (P = 0.09). A total of 92 patients (46%) were successfully weaned from ECMO, 8 (4%) were directly bridged to heart transplantation, and 18 (9.1%) to the implantation of ventricular assist device (Figure 1). A total of 69 patients (34.8%) survived until hospital discharge. The survival curve remained at plateau at 6‑month follow‑up (34.8%) and only slightly decreased at 1 year following ECMO implantation (32.8%). The log‑rank test showed a difference in one‑year survival following ECMO implantation between the surgical and nonsurgical ECMO groups (P = 0.037). However, no such relation was observed at 1 year following hospital discharge (P = 0.92) (Figure 4). In the follow‑up lasting up to 2020, the median (IQR) for the annual volume of ECMO implantation in our center was 43.5 (32.25–53.25) (Figure 5).
Discussion
Indications for ECMO
Persistent exceptionally high mortality rates among ECMO recipients are a clear indicator of the need for improvement in patient selection and device therapy management by clinicians. Randomized, double‑blind studies are particularly challenging to execute in this high‑risk population, and the primary evidence currently needs to be drawn mainly from registries and patient outcome analysis.1,8
This study analyzed the real‑world use of ECMO at a high‑volume cardiosurgical reference center, reinforcing the complexity and difficulty of patient selection and management dilemmas in MCS therapy. The median (IQR) for the annual volume of ECMO implantation in our center in years 2013 to 2020 was 43.5 (32.25–53.25), which was more than twice the number of the median for the annual center volume from the recent 2020 European Extracorporeal Life Support Organization annual report (18 cases per center).8
The majority of patients with refractory CS simply die if left untreated, and ECMO is a plausible treatment option concerning speed, circulatory support potency, and cost‑effectiveness.9 Therefore, it is the preferred method of MCS in an acute setting at our institution. The implanted ECMO circuit is selected to serve as a bridge to cardiac recovery, durable left ventricular assist device implantation, heart transplantation or, in the case of uncertainty, allows further evaluation and diagnostic tests before ensuing therapeutic decisions.9,10
Preimplantation risk factors
The population of patients who required ECMO support has been previously characterized as high‑risk, with a high prevalence of underlying chronic cardiac, pulmonary and kidney diseases,8,11-13 which were likewise widespread in our cohort (Table 1 and Supplementary material, Figure S1).
Earlier studies identified several significant predictors of in‑hospital mortality among preimplantation factors. A recent analysis by Salna et al,13 including 355 patients treated with VA ECMO, found that age over 72 years was an independent predictor of mortality, associated with a higher prevalence of comorbidities, including coronary disease, previous strokes, and chronic kidney disease. Our findings confirmed previous reports that older age was an independent risk factor for increased in‑hospital mortality (OR, 1.02; P = 0.007). Chronic conditions such as diabetes and kidney disease were significantly more frequent among nonsurvivors, but with only a strong trend for poorer survival in univariable logistic regression analysis. We additionally found that the overall critical preimplantation status with multiorgan failure was a stronger predictor of in‑hospital death than age (OR, 4.45; P <0.001). Nevertheless, no particular risk factor related to the latter (mechanical ventilation, intra‑aortic balloon counterpulsation, or CPR prior to ECMO implantation) was individually associated with in‑hospital mortality (Supplementary material, Table S1). The results underscore the difficulty and inconsistency in identifying unique constant preimplantation mortality risk factors within such a heterogeneous population of ECMO candidates.
There is an increasing number of reports of ECMO use in urgent clinical conditions such as SCA and CS. In a recent metanalysis of 3098 patients treated for SCA by Ouweneel et al,14 it was associated with an increased survival rate and an increase in a favorable neurological outcome. In our study, as many as 32 patients who experienced SCA and another 53 who were admitted to the hospital with acute cardiac injury (Figure 3) required prompt cardiocirculatory revival and bridging with ECMO. Moreover, SCA treated with ECMO in our series was not associated with increased in‑hospital mortality (OR, 1.02; P = 0.95), showing a satisfactory survival‑to‑discharge rate of 34%, comparable to previous studies of in‑hospital SCA in which the reported values ranged from 19% to 60%.15-17 On the contrary, in a large meta‑analysis of in‑hospital SCA with conventional resuscitation conducted by Girotra et al,18 the overall survival rate to discharge was 17% (14 357/84 625). Extracorporeal CPR is hoped to offer better outcomes than conventional CPR for in‑hospital SCA. However, randomized studies are needed.
Postimplantation management and risk factors
Respiratory complications are a well‑known detrimental factor of prolonged hospitalizations and increased in‑hospital mortality for postsurgical patients and those with heart failure.19-24 At our center, we prioritize early extubation after ECMO implantation, which is executed after the weaning from sedation, if the patient has no signs of altered mental status, and the process of weaning from the ventilator is uncomplicated. The summary of the “Awake ECMO” strategy by Langer et al25 describes several benefits of reduced mechanical ventilation time, with the key being the prevention of ventilator‑induced diaphragm dysfunction and ventilator‑associated pneumonia. Recently, Youn et al26 reported in‑hospital mortality rates for deferred extubation (>48 hours) and early extubation (≤48 hours) in ECMO patients, as 24.4% and 8.3%, respectively. In our study, the median time of mechanical ventilation to first extubation of all patients was 45 (2–918) hours, and 28% were extubated in less than 24 hours after ECMO implantation, which supports the adherence to the early extubation protocol, whenever possible. However, in line with the study by Youn et al,26 the occurrences of respiratory complications were found to confer risk for in‑hospital mortality among our patients. Those who required a longer time of mechanical ventilation to the first extubation and longer total time of mechanical ventilation, as well as those requiring reintubation or tracheostomy, were less likely to survive (Table 2). Pneumonia complicated the clinical course in 10% of patients, with Klebsiella and Staphylococcus species being responsible for most of the positive cultures obtained (Table 3).
An important prognostic factor for in‑hospital mortality was AKI requiring RRT (OR, 2.4; P <0.004). Continuous RRT is the preferred method for hemodynamically unstable patients.27 Initiation of dialysis was individualized based on the fluid overload level and development of metabolic disorders associated with AKI. A couple of studies analyzed the incidence and outcomes of AKI and RRT during ECMO, providing differing results. The occurrence of AKI among ECMO recipients was reported between 30% and 70%.28-31 The need for concomitant RRT and ECMO in our study was 47%. In an analysis of 135 critically ill adults treated with ECMO, Antonucci et al32 also reported the use of RRT in 47%, while no association with increased mortality was confirmed. However, in line with our observations, several studies28-30 noted higher mortality in patients receiving joint RRT and ECMO than those on ECMO alone. The heterogeneous structure of these studies must be considered, along with the possible overall higher disease severity in those presenting with acute renal failure. It can be assumed that, rather than the use of RRT alone, AKI itself is a substantial risk factor of mortality.
Weaning from ECMO
Nearly half (46.5%) of all our patients were successfully weaned from ECMO, which is in line with previous studies reporting successful weaning rates of 28% to 63%.10,33-35 Rastan et al11 assessed 517 adult patients receiving ECMO support for postcardiotomy CS and reported a high successful weaning rate of 63.3%. However, over half of the weaned patients died during hospitalization, and less than one‑third (24.8%) was discharged from the hospital. We confirmed a slightly lower but persistently high death rate among ECMO‑weaned patients during hospitalization, reaching 39%. The leading cause of death were: multiorgan failure, neurologic complications, insufficient cardiac recovery, infection, and bleeding complications (Figure 1). As shown in Supplementary material, Table S2, several preweaning risk factors were identified to significantly influence hospital mortality. Elevated creatinine, bilirubin, INR, and lactate levels are markers of the severity of multiorgan impairment, which are usually present simultaneously and represent internal interrelationship between organs, generating an additive harmful effect on clinical status. The abovementioned parameters are well‑known risk factors of decreased survival in intensive care patients.36,37
We also noticed that myocardial recovery assessed by the measurement of preweaning LVEF was an additional significant factor of successful weaning and survival to hospital discharge after ECMO explantation (Supplementary material, Table S2). In our series, preweaning LVEF of hospital survivors was 35% versus 20% in those who died during hospitalization (P = 0.049). Fiser et al34 reported that patients with LVEF below 30% were significantly less likely to be weaned from ECMO than those with LVEF above 30%. LVEF measurement, as a fundamental echocardiographic parameter, is a standard step in the different weaning algorithms already described.34,38-40
Complications
In our experience, similarly to previous reports, ECMO therapy is associated with a myriad of possible complications8,9,11,12 (Table 3). Bleeding was the most common adverse event in our study, with an incidence of 76%. Such a high rate may be explained by a high proportion of postcardiotomy patients (79.7%). Postoperative bleeding is widespread in the abovementioned cohort, ranging from 3% to 79% in previous studies,12,41,42 influenced by surgical trauma and varying severity of acquired postsurgical coagulopathy, on top of hepatic and kidney dysfunction arising in CS. Additionally, ECMO itself has been associated with the induction of specific coagulopathy due to hemolysis, thrombocytopenia, acquired von Willebrand syndrome, and disseminated intravascular coagulopathy.8,9,41,43 In our patients, hemorrhages mainly occurred from cannulation and surgical sites (Table 3). Life‑threatening and major bleeds7 were strong, single univariable risk factors of hospital mortality (OR, 2.95 and OR, 2.66, respectively; Table 3). Notably, 85% of those most hazardous bleeding complications affected the postcardiotomy group, and bleeding from the postsurgical site significantly impacted hospital mortality (OR, 2.53; Table 3). As many as 38% of all patients required resurgery due to uncontrollable bleeding, with most of them (88%) being postsurgical patients. Our results are comparable with the single‑center report by Rastan et al11 in which 58% of patients required reintervention because of excessive bleeding, as well as to the recent meta‑analysis of 20 studies (including 1866 patients) reporting 41% patients with major or pronounced bleeding and 42% requiring thoracotomy for bleeding or tamponade.44
A broad spectrum of neurologic complications in ECMO patients is well reported, comprising different levels of cognitive impairments, strokes, and intracerebral hemorrhages.8,11,12,33,35,37,41,44 The most frequent cerebrovascular disorder in our series was ischemic stroke affecting 1 in 10 patients receiving the ECMO therapy. Ischemic stroke significantly influenced hospital mortality in our study and is a well‑known risk factor for cognitive impairment and deteriorated quality of life in the long‑term follow‑up. Intracerebral hemorrhage with an overall incidence of 4.5% was the most catastrophic adverse event among our patients with 100% hospital mortality.
Outcomes
Approximately 20 055 patients have been treated for cardiac support, with survival‑to‑discharge rates of 45% for adults, according to the 2020 Extracorporeal Life Support Organization registry report.8 Comparably with other studies,8,34,45 our in‑hospital, 6‑month, and 1‑year mortality rates were 65.2%, 65.2%, and 67.2%, respectively.
The study cohort comprised mixed etiologies of cardiocirculatory instability, surgical (79.8%) and nonsurgical (20.2%). Patients with postcardiotomy CS had a significantly lower out‑of‑hospital survival rate of 32.3% than those with decompensated heart failure (45%; log‑rank P = 0.037) (Figure 4). Keeping in mind the modest size of the latter group (40 patients) and the possible selection bias, it adds to the limited available data regarding a series of unselected patients with acutely decompensated heart failure treated with VA ECMO, where survival to hospital discharge varies from 40% to 50%34,46,47
Nearly half of all patients (92 [46.5%]) were successfully weaned from ECMO, but more than one third (36 [39%]) of the weaned patients died during hospitalization. These data underscore the significant overall morbidity and mortality within this population, enduring after treating the acute cardiovascular incident with VA ECMO. The association of mortality with the coexisting multiple organ injury is apparent, as the majority of patients (61%) died owing to multiorgan failure after ECMO withdrawal.
In approximately 1 in 10 patients, ECMO was a bridge to heart transplantation, either after direct bridging or following an ECMO period of ventricular assist device support (Figure 1). Posttransplantation survival to discharge in cardiac graft recipients with pretransplant ECMO was 68%, and all of the discharged patients were alive 6 and 12 months postimplantation. Our results are comparable with previous reports, in which hospital survival of heart transplant recipients with pretransplant ECMO varied from 40% to 91.2%.48-50 Such survival rates in patients initially treated for prognostically fatal CS are appealing and endorse further use of this therapy line in all eligible candidates.
Limitations of the study
The main limitation of the study is its retrospective design. Although the study population was matched quite well to the assessed issue, the outcomes and conclusions are related to a single‑center experience and should be viewed in this context and treated with caution.
Conclusion
While no particular preimplantation organ damage was prognostic for hospital mortality, a coexisting multiple organ injury resulted in poor prognosis at any stage of treatment. No predictive value was found in the duration of VA ECMO. An increasing bleeding complication rate significantly influenced morbidity and mortality. Nevertheless, the survival benefit of ECMO therapy in the population of patients with CS endorses its future use, despite the associated interferences.
- Ponikowski P, Voors AA, Anker SD, et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur J Heart Fail. 2016; 18: 891‑975. | Crossref
- Thygesen K, Alpert JS, Jaffe AS, et al. Fourth universal definition of myocardial infarction (2018). J Am Coll Cardiol. 2018; 72: 2231‑2264.
- Knuuti J, Wijns W, Saraste A, et al. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes. Eur Heart J. 2020; 41: 407‑477.
- Cosentino F, Grant PJ, Aboyans V, et al. 2019 ESC Guidelines on diabetes, pre‑diabetes, and cardiovascular diseases developed in collaboration with the EASD. Eur Heart J. 2020; 4: 255‑323.
- Galiè N, Humbert M, Vachiery JL, et al. 2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension: the Joint Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS): Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC), International Society for Heart and Lung Transplantation (ISHLT). Eur Heart J. 2016; 37: 67‑119. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION