A case of vaccine‑induced immune thrombotic thrombocytopenia in a 43‑year old female patient



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
A case of vaccine‑induced immune thrombotic thrombocytopenia in a 43‑year old female patient
Vaccine‑induced immune thrombotic thrombocytopenia (VITT) has become a new diagnostic and therapeutic challenge in the era of COVID‑19 prevention. The vast majority of reported VITT cases have occurred following adenoviral vector‑based vaccination with ChAdO × 1 nCoV‑19 (Oxford / AstraZeneca)1 or Ad26.COV2.S (Janssen; Johnson & Johnson).2 The pathophysiology of this syndrome involves the presence of immunoglobulin (Ig) G antibodies; these identify platelet factor 4 (PF4), resulting in platelet activation and a broad spectrum of thrombotic complications.3
A 43‑year‑old woman was referred to the emergency department due to severe abdominal pain and bloody diarrhea that started several hours previously. Her medical history included a gastric ulcer several years ago, smoking, chronic obstructive pulmonary disease, and Ad26.COV2.S vaccination 9 days before hospitalization. Complete blood count (CBC) revealed severe thrombocytopenia (platelets, 7 G/l; reference range, 150–400 G/l); the hemoglobin level (125 g/l; reference range, 112–150 g/l) and leukocyte count (9.2 G/l; reference range, 4.4–11.3 G/l) were within the reference ranges. Prothrombin time (PT) and activated partial thromboplastin time (APTT) were normal. A high concentration of C‑reactive protein (102 mg/l; reference range, 0–5 mg/l) was observed. Rectal examination revealed bloody stools. Control CBC showed a drop in the hemoglobin level to 103 g/l. The patient received 5 units of platelet concentrate to stop the ongoing lower gastrointestinal bleeding, which led to an increase in platelet count to 104 G/l.
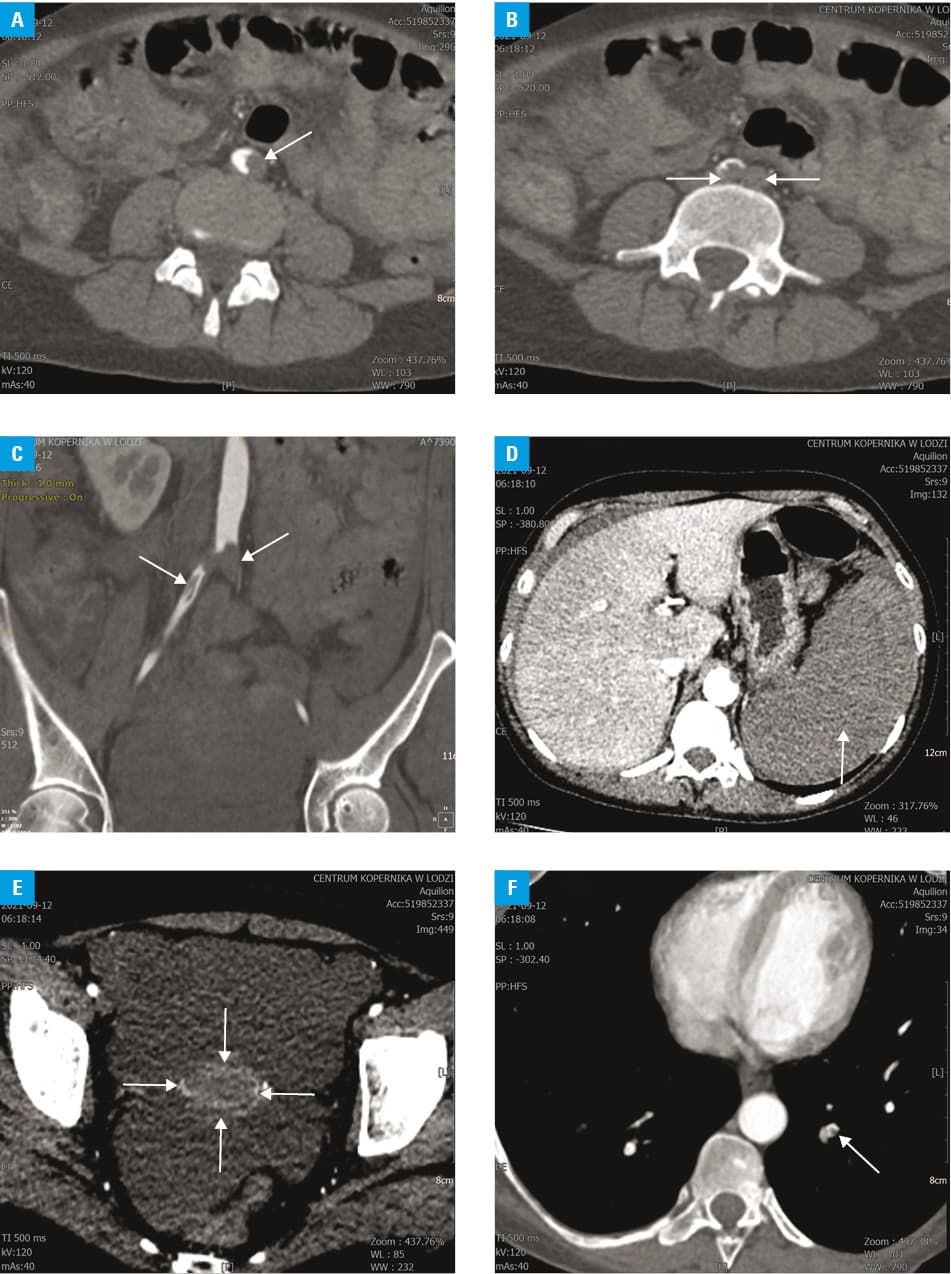
After consultation, the patient was transferred to the Department of Hematology with a suspicion of immune thrombocytopenia / VITT. On admission, she presented with severe abdominal pain. Laboratory tests showed profound thrombocytopenia (14 G/l), anemia (hemoglobin, 90 g/l), hypofibrinogenemia (1.42 g/l; reference range, 2–3.9 g/l), an increased D‑dimer concentration (62.64 mg/l fibrinogen equivalent units; reference range, 0–0.5 mg/l fibrinogen equivalent units), and normal PT and APTT. The lower gastrointestinal bleeding continued. Two hours after admission, the patient developed severe lower left limb pain. Computed tomography angiography of the abdomen and lower limbs showed abdominal aortic thrombosis, common left and right iliac artery thrombosis (saddle embolus), swollen walls of the transverse, ascending colon, and cecum, splenic infarction, and a massive amount of free intraperitoneal fluid (fluid depth up to 5 cm) (Figure 1A–1E). Pulmonary angiography revealed signs of segmental pulmonary artery embolism (Figure 1F).
Due to critical left limb ischemia, threatening amputation, the patient required emergency vascular surgery. Considering the substantial probability of VITT, intravenous immunoglobulins (1 g/kg of body weight) and intravenous steroids (dexamethasone, 40 mg) were administered. In preparation for vascular surgery, the patient received 6 units of platelet concentrate. Despite intensive treatment, her condition worsened dramatically, leading to death 12 hours after admission. The autopsy confirmed thrombosis of the common iliac artery, pulmonary embolism, necrotic lesions in the colon, splenic rupture, and a gastric ulcer. A strongly positive result of anti‑PF4 IgG antibodies by enzyme‑linked immunosorbent assay (optical density, 3.8; optical density >0.4 is considered a positive result) confirmed the diagnosis of VITT.
In the presented case, a combination of bleeding and multiple‑site thrombosis (arterial and venous) was observed. The extent of thrombotic complications suggests that the patient may also have had congenital or acquired thrombophilia. In addition, it cannot be excluded that the platelet transfusions administered to control the bleeding and before the surgery contributed to the development and progression of thrombosis, predominantly in the arterial bed.
- Schultz NH, Sørvoll IH, Michelsen AE, et al. Thrombosis and thrombocytopenia after ChAdO × 1 nCoV‑19 vaccination. N Engl J Med. 2021; 384: 2124‑2130. | Crossref
- See I, Su JR, Lale A, et al. US case reports of cerebral venous sinus thrombosis with thrombocytopenia after Ad26.COV2.S vaccination, March 2 to April 21, 2021. JAMA. 2021; 325: 2448‑2456. | Crossref
- Franchini M, Liumbruno GM, Pezzo M. COVID‑19 vaccine‑associated immune thrombosis and thrombocytopenia (VITT): diagnostic and therapeutic recommendations for a new syndrome. Euro J Haematology. 2021; 107: 173‑180. | Crossref
ARTICLE INFORMATION