The effect of atrial fibrillation on the safety and efficacy of mechanical thrombectomy in patients with stroke
Key words: atrial fibrillation, stroke, thrombectomy



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
The effect of atrial fibrillation on the safety and efficacy of mechanical thrombectomy in patients with stroke
Introduction: The association between atrial fibrillation (AF) and the outcome of mechanical thrombectomy (MT) in patients with stroke has not been determined so far.
Objectives: We aimed to evaluate the effect of AF on the efficacy and safety of MT in patients with stroke and to investigate the association between prior anticoagulation and symptomatic intracranial bleeding (ICB).
Patients and methods: Patients who underwent MT for stroke were enrolled. The effect of AF on the safety and efficacy of MT was assessed. Clinical data of patients were retrospectively collected. Neurologic status was evaluated on day 1 and 2 after stroke using the National Institute of Health Stroke Scale. Functional status was assessed at 10, 30, and 90 days using the modified Rankin Scale.
Results: We enrolled 417 patients with stroke (mean age, 70 years), including 108 patients (25.89%) with AF. Patients with AF were older than those without AF (mean [SD] age, 73.77 [8.97] years and 65.70 [18.88] years, respectively; P <0.01). The percentage of patients with poor functional status at 10, 30, and 90 days after stroke was higher among patients with AF than among those without AF. There were no significant differences between groups in the rate of ICB or death. Age, neurologic status, and the Thrombolysis in Cerebral Infarction score had the strongest effect on the functional status. The use of nticoagulant therapy before stroke did not significantly increase the risk of symptomatic ICB after MT, also in patients with an international normalized ratio in the therapeutic range.
Conclusions: Atrial fibrillation does not affect MT outcomes in patients with acute stroke. Age, the degree of postinterventional reperfusion, and neurologic status in ultra‑acute stroke are the strongest predictors of poor functional status.
What's new?
Our study demonstrated that atrial fibrillation (AF) has a neutral effect on the safety and efficacy of mechanical thrombectomy (MT) in the ultra‑acute phase of stroke (≤6 hours from onset). Anticoagulant therapy before stroke does not increase the risk of ICB in stroke patients undergoing MT. The strongest predictors of the functional status in patients with AF‑related stroke at 10, 30, and 90 days after MT included age, the neurologic status at day 1 after stroke, and the result of reperfusion after the procedure (according to the Thrombolysis in Cerebral Infarction score).
Introduction
The inclusion of mechanical thrombectomy (MT) in stroke therapy has been a breakthrough in reducing stroke‑related disability. The meta‑analysis of patient‑level data pooled from 5 randomized trials as part of the Highly Effective Reperfusion Evaluated in Multiple Endovascular Stroke Trials (HERMES) collaboration showed that MT results in the recanalization of more than 80% of arteries subjected to intervention.1 Moreover, 46% of patients returned to full independence within 3 months after stroke due to large‑vessel occlusion.1 However, this means that significant neurologic deficit is present in half of the patients after stroke, including some of those with a favorable angiographic outcome of MT. The predictors of unfavorable prognosis in the subpopulation of patients treated by endovascular therapy for stroke include older age, diabetes mellitus, poor neurologic status on the first day of stroke, and low Alberta Stroke Program Early CT Score (ASPECTS).2-5
The association between atrial fibrillation (AF) and thrombectomy outcome has not been fully determined to date, and the results of available studies are inconsistent.2,6-11 Atrial fibrillation affects 28% to 50% of stroke patients undergoing MT.6,12 The disease is an independent predictor of a worse functional status and increased mortality within the first year after stroke.13-16 Patients with AF‑related stroke tend to be older and have multiple comorbidities.13,17 Stroke in AF patients more often involves the anterior intracranial vascular supply than in patients without AF. Moreover, it is more extensive due to the occlusion of a large artery. The clinical profile of patients with AF and stroke indicates a worse prognosis, which is not only due to AF itself but also due to comorbidities.
The effect of AF on the outcome of reperfusion therapy has not been clearly defined either for intravenous thrombolysis (using recombinant tissue plasminogen activator [rtPA]) or for MT. Previous studies, including our own research, showed that AF seems to predict patient‑related outcomes.17-22 However, some investigators suggested that AF has no significant impact in this setting.23 A lower recanalization rate after rtPA therapy in AF patients was previously reported.19 This may be due to the size of the occlusion or the morphology and composition of cardiac thrombus. Research indicated a higher fibrin content in an arterio‑arterial embolism and a higher content of red blood cells in cardiogenic embolism.24 It is unknown whether the histological structure of a thrombus affects the outcome of MT, although it is possible that the composition of a thrombus facilitates its retrieval. Similarly, it remains to be determined whether the presence of AF is relevant for the final outcome of MT. One of the subanalyses in the MR CLEAN study (Multicenter Randomized Clinical Trial of Endovascular Treatment for Acute Ischemic Stroke in the Netherlands) demonstrated a nonsignificant trend toward fewer benefits of MT in AF patients.25 However, this was not confirmed by another meta‑analysis from HERMES collaborators, which showed no negative effect of AF on MT efficacy.11 Other studies reported that AF adversely affects the functional status of patients undergoing MT in the course of stroke.6,10
The aim of our study was to evaluate the effect of AF on the safety and efficacy of MT in the acute and chronic phases of stroke in patients with acute stroke due to large‑vessel occlusion. We hypothesized that AF does not worsen the clinical outcome of MT in stroke patients with arrhythmia compared with those without arrhythmia. The hypothesis was based on the fact that the high lability of a cardiac thrombus facilitates its removal. It was also supported by our previous research showing a neutral effect of AF on the outcome of another reperfusion therapy (ie, intravenous thrombolysis) in patients with stroke. Additionally, we aimed to investigate the association between prior anticoagulation and symptomatic intracranial bleeding (ICB) in patients undergoing MT.
Patients and methods
This retrospective study included patients who underwent endovascular therapy for stroke at the Upper‑Silesian Medical Center of the Medical University of Silesia in Katowice, Poland, between 2019 and 2020. All patients treated with MT during this 24‑month period were initially enrolled in the study. The following data were collected: patient age at first‑ever stroke; comorbidities such as AF, arterial hypertension, coronary heart disease, diabetes mellitus, lipid disorders, and >70% atherosclerotic carotid artery stenosis (ipsilateral to the acute ischemic brain lesion); neurologic status on the first and second day of stroke, evaluated using the National Institute of Health Stroke Scale (NIHSS)26; and functional status on days 10, 30, and 90 after stroke, evaluated using the modified Rankin Scale (mRS).27
Paroxysmal, persistent, or chronic AF was diagnosed on the basis of previous medical records or electrocardiography, or on the basis of 24‑hour electrocardiographic monitoring performed during stroke‑related hospitalization (≤14 days after onset). Hypertension was diagnosed on the basis of the European Society of Cardiology (ESC) guidelines. Diabetes was diagnosed according to the Diabetes Association criteria. Dyslipidemia was defined according to the 2019 ESC and European Atherosclerosis Society guidelines on the management of dyslipidemias. The degree of the common carotid artery stenosis and / or internal carotid artery stenosis was assessed according to the North American Symptomatic Carotid Endarterectomy Trial criteria.28 Finally, hemorrhagic lesions were evaluated based on head computed tomography performed 24 hours after MT and the ECASS study (European Cooperative Acute Stroke Study).29
Mechanical thrombectomy
Mechanical thrombectomy procedures were performed at the Department of Interventional Neuroradiology in Upper‑Silesian Medical Center of the Silesian Medical University in Katowice, using the state‑of‑the‑art equipment, namely, Axiom Artis Zee Bi‑Plane (Siemens Medical Solutions USA, Inc, Malvern, Pennsylvania, United States). In case this angiosuite was not available, the procedure could also be performed at the vascular surgery or interventional cardiology catheterization laboratories equipped with the appropriate monoplane machines. A total of 307 patients (73.3%) were treated using a biplane machine. Based on individual preferences and the clinical status of the patient, general anesthesia or conscious sedation was used. In each case, an anesthesiologist was involved in the procedure. The MT was performed by a single operator out of a large multidisciplinary team including 2 neuroradiologists, 3 vascular surgeons, and 4 interventional cardiologists. Neurologists were responsible for the referral of patients for the procedure, logistics of the procedure, and postoperative care. Most MT procedures were performed using stent retrievers (Trevo, Catch, Soliter, Tiger) and an 8F FlowGate2 Balloon Guide Catheter. For the remaining procedures, distal aspiration (Penumbra, Sofia, Cathalist) or combined stent retrievers and distal aspiration are used.
As the study was not a medical experiment, the approval of the Bioethics Committee was not required.
Statistical analysis
Patients were divided into 2 groups according to the presence of AF. Demographic, clinical, radiologic, biochemical, and echocardiographic parameters were assessed and compared between groups.
Univariable analyses of the differences in binary variables between groups with and without AF were performed using the Pearson χ2 test. Continuous variables were compared between male and female patients using the Welch analysis of variance or the Kruskal–Wallis test, as appropriate. P values were corrected for multiple testing using the Benjamini–Hochberg false discovery rate.
Multivariable models were built using ordinal logistic regression for ordinal outcomes. Variable selection for the model included automatic selection (stepwise, forward, and backward) based on Akaike and Bayesian information criterion. To evaluate the accuracy of model predictions, the leave‑one‑out procedure and the multiclass AUC estimator were used. All statistical analyses were performed using R version 3.6.1 (the R Foundation for Statistical Computing, Vienna, Austria).
The following parameters were assessed in the logistic regression model: age, sex, AF, hypertension, coronary heart disease, diabetes, lipid disorders, >70% carotid artery stenosis, smoking, Thrombolysis in Cerebral Infarction (TICI) score, ICB after the intervention (including symptomatic ICB), NIHSS score, rtPA therapy, anticoagulant and antiplatelet therapy at least 1 month before stroke onset, reduced ejection fraction (<50%), enlarged left atrium (>40 mm), and hemicraniectomy.
Results
We enrolled 421 patients with stroke (mean age, 70 years [range, 20–92]; women, 47.7%), who were hospitalized between 2019 and 2020 and who underwent MT for ultra‑acute stroke (within ≤6 hours since onset). Participants constituted 30.17% of all patients with ischemic stroke treated at the Upper‑Silesian Medical Center during the study period (a total of 1382 patients with stroke). Four patients who underwent MT were excluded because of insufficient medical records. Of the 417 patients included in the study, 254 (61.2%) were treated with both rtPA and MT (Figure 1). The demographic and clinical data of patients are presented in Table 1.
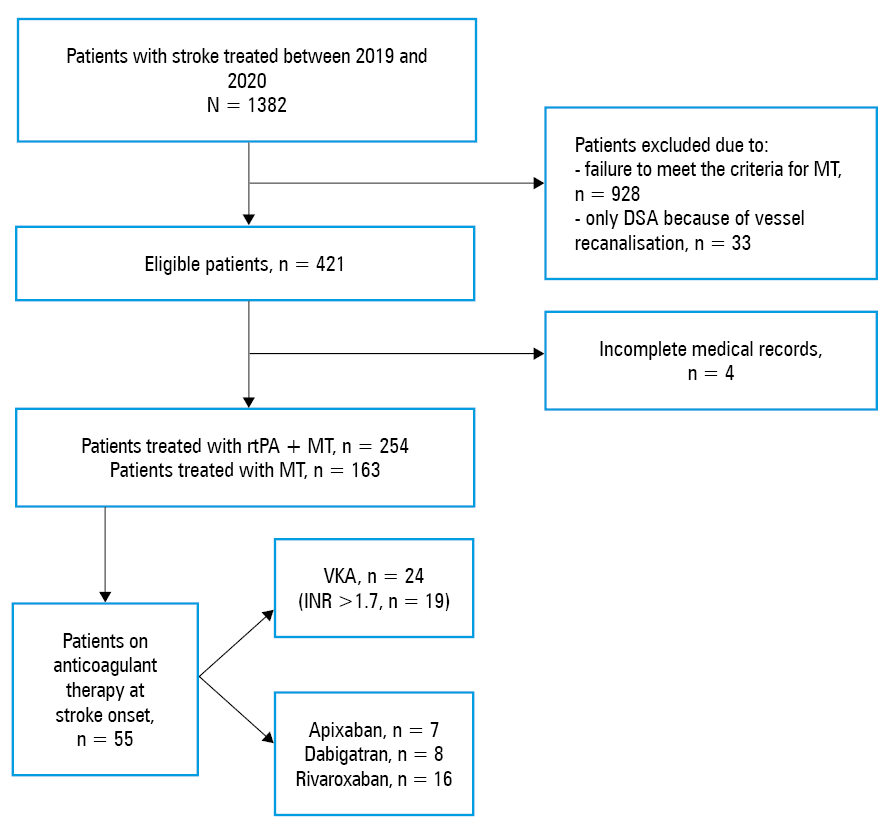
Abbreviations: DSA, digital subtraction angiography; INR, international normalized ratio; MT, mechanical thrombetomy; rtPA, recombinant tissue plasminogen activator; VKA, vitamin K antagonist
Parameter | Value |
Data are presented as number (percentage) of patients unless otherwise indicated.
Abbreviations: AF, atrial fibrillation; CAS, carotid artery stenosis; EF, ejection fraction; ICA, internal carotid artery; ICB, intracranial bleeding; LA, left atrium; mRS, modified Rankin Scale; NIHSS, National Institutes of Health Stroke Scale; TICI, Thrombolysis in Cerebral Infarction; others, see Figure 1 | |
Age, y, mean (SD); median (min–max) | 67.8 (13.2); 70 (20–92) |
Female sex | 199 (47.7) |
AF | 108 (26.0) |
AF diagnosis before stroke | 72 (17.2) |
Paroxysmal AF | 65 (15.6) |
Persistent AF | 43 (10.3) |
Arterial hypertension | 315 (75.5) |
Diabetes mellitus | 105 (25.3) |
Coronary heart disease (data for n = 408) | 221 (52.9) |
Lipid disorders | 168 (40.4) |
CAS (ipsilateral ICA ≥50%) | 51 (12.1) |
Smoking (data for n = 310) | 115 (37.1) |
EF <50% (data for n = 259) | 51 (19.7) |
LA diameter >40 mm (data for n = 259) | 47 (18.1) |
High troponin levels (data for n = 374) | 202 (54.0) |
Thrombocytopenia (data for n = 412) | 27 (6.6) |
Antiplatelet therapy before MT | 134 (32.1) |
Anticoagulation before MT | 55 (13.2) |
INR out of the therapeutic range (in treated patients) | 39 (70.9) |
NIHSS score at 1 day after stroke; points, mean (SD); median (range) | 12.8 (5.6); 12 (0–43) |
NIHSS score at 2 days after stroke; points, mean (SD); median (range) | 12.5 (6.5); 12 (0–40) |
mRS at 10 days after stroke; points, mean (SD); median (range) | 3.87 (1.75); 4 (0–6) |
mRS at 30 days after stroke; points, mean (SD); median (range) | 3.32 (1.69); 4 (0–6) |
mRS at 90 days after stroke; points, mean (SD); median (range) | 3.12 (1.71); 3 (0–6) |
TICI grade 2b or 3 | 274 (65.7) |
Hemicraniectomy | 23 (5.5) |
Intravenous rtPA | 254 (61.2) |
ICB | 95 (22.7) |
Symptomatic ICB | 21 (5) |
Of the 417 patients, 274 (65.7%) were referred to our hospital from another institution (drip‑and‑ship model). We assessed data on MT therapy collected from all patients included in the study. The following parameters were determined: a mean (SD) time from onset to the first arrival at the hospital of 162 (12.2) minutes (range, 36–240); a mean (SD) time from onset to the first head computed tomography scan of 198 (7.8) minutes (range, 119–315); a mean (SD) time from onset to starting MT (groin puncture) of 242 (12.3) minutes (range, 80–368); and a mean (SD) duration of MT of 111 (14.5) minutes (range, 24–199).
The study group included 108 patients with AF (25.89%), typically paroxysmal AF (65 patients; 60.18% of all patients with AF). Of the 72 patients with a previous diagnosis of AF, 55 (76.3%) used anticoagulant therapy for at least 1 month before MT (Figure 1). International normalized ratio (INR) within the therapeutic range (2.5–3.2) was observed in 16 patients (66.6% of all patients on warfarin). The mean age of patients with AF was higher (false discovery rate [FDR]–adjusted P <0.01) than that of patients without AF (mean [SD], 73.77 [8.97]; median [IQR], 75 [68.75–81] years vs mean (SD), 65.70 (18.88); median (IQR), 68 [56.5–76] years, respectively). Patients with AF more often showed reduced ejection fraction (24 [33%] vs 27 [15%]; FDR‑adjusted P <0.01) and left atrial enlargement (22 [30%] vs 25 [13%]; FDR‑adjusted P <0.012). The rate of hemicraniectomy was similar in patients with and without AF (22 [7%] vs 1 [1%]; FDR‑adjusted P = 0.06). The percentage of patients with poor functional status at 10, 30, and 90 days was also similar in both groups. There were no differences between patients with AF and those without AF in the percentage of symptomatic bleeding according to ECASS criteria (26 [24%] and 69 [22%], respectively; FDR‑adjusted P = 0.88) as well as in the percentage of patients with TICI grade 2b/3 (72 [67%] and 202 [66%], respectively; FDR‑adjusted P = 0.93). The incidence of symptomatic ICB was also similar in patients with and without AF (7 [6.48%] and 15 [4.85%], respectively; FDR‑adjusted P = 0.69). The incidence of symptomatic ICB was similar in patients on vitamin K anticoagulants (VKAs) with the INR within the therapeutic range and in those with AF and the INR outside the therapeutic range treated with VKAs and direct oral anticoagulants (DOACs; 2 [12.51%] vs 5 [12.82%], respectively; FDR‑adjusted P = 0.91). The rate of death did not differ between patients with and those without AF. A detailed comparison between groups is presented in Table 2.
Parameter | Patients with AF (n = 108) | Patients without AF (n = 309) | FDR‑adjusted P value | |
Data are presented as number (percentage) of patients unless otherwise indicated.
Abbreviations: FDR, false discovery rate; IQR, interquartile range; others, see Table 1 | ||||
Age, y, median (Q1; Q3) | 75 (68.75; 81) | 68 (56.5; 76) | <0.01 | |
Sex | Female | 59 (55) | 140 (45) | 0.19 |
Male | 49 (45) | 169 (55) | ||
NIHSS score, points, mean (SD); median (range) | 13.99 (5.36); 13 (1–27) | 12.17 (6.53); 12 (0–43) | 0.14 | |
LA diameter >40 mm | 22 (30) | 25 (13) | <0.01 | |
EF <55% | 24 (33) | 27 (15) | <0.01 | |
Hemicraniectomy | 22 (7) | 1 (1) | 0.06 | |
TICI grade 2b or 3 | 72 (67) | 202 (66) | 0.93 | |
Antithrombotic therapy before stroke | 77 (71) | 57 (19) | <0.01 | |
ICB | 26 (24) | 69 (22) | 0.88 | |
Symptomatic ICB | 7 (6.4) | 15 (4.8) | 0.73 | |
mRS score at 10 days, median (Q1; Q3) | 4 (3; 5) | 4 (3; 5) | 0.83 | |
mRS of 0–2 at 10 days | 25 (32.1) | 70 (23) | >0.99 | |
mRS of 6 at 10 days (death) | 18 (16.7) | 53 (17.4) | 0.98 | |
mRS score at 30 days, median (Q1; Q3) | 4 (2; 5) | 4 (2; 5) | 0.35 | |
mRS of 0–2 at 30 days | 25 (27.2) | 80 (31.5) | 0.35 | |
mRS of 6 at 30 days (death) | 7 (7.6) | 10 (3.9) | 0.27 | |
mRS score at 90 days, median (Q1; Q3) | 4 (2; 5) | 3 (2; 5) | 0.35 | |
mRS of 0–2 at 90 days | 28 (32.5) | 89 (36.2) | 0.63 | |
mRS of 6 at 90 days (death) | 5 (5.8) | 9 (3.7) | 0.59 | |
In the multivariable analysis, parameters with the strongest effect on the functional status (mRS) at 10 days were as follows: age, NIHSS score on the first day of stroke, diabetes, and TICI grade (Table 3, Figure 2); at 30 days: age, NIHSS score on the first day of stroke, and lipid disorders (Table 3, Figure 3), and at 90 days: age, NIHSS score on the first day of stroke, and TICI grade (Table 4, Figure 4).
Coefficient | OR | 95% CI | P value |
Abbreviations: OR, odds ratio; others, see Table 1 | |||
mRS at discharge | |||
Age | 1.034 | (1.009–1.06) | <0.01 |
NIHSS at day 1 after stroke | 1.103 | (1.039–1.174) | <0.01 |
Diabetes mellitus | 1.827 | (0.884–3.93) | 0.11 |
TICI grade | 0.506 | (0.255–0.976) | 0.04 |
mRS at day 30 | |||
Age | 1.048 | (1.015–1.086) | <0.01 |
NIHSS score | 1.166 | (1.077–1.275) | <0.001 |
Lipid disorders | 0.554 | (0.265–1.126) | 0.1 |
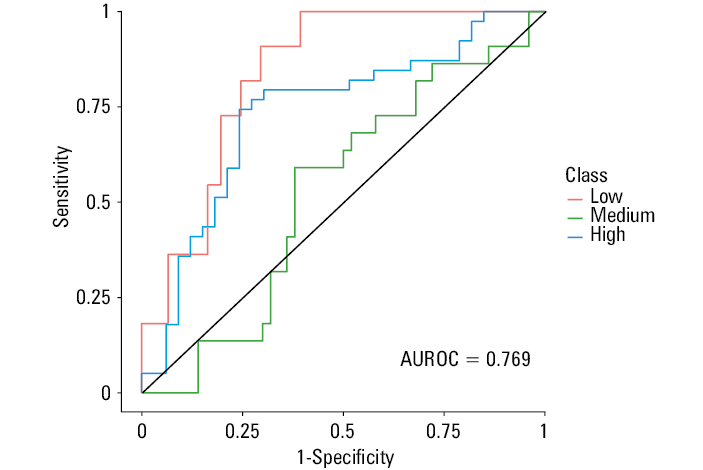
Abbreviations: AUROC, area under the receiver operating characteristic curve
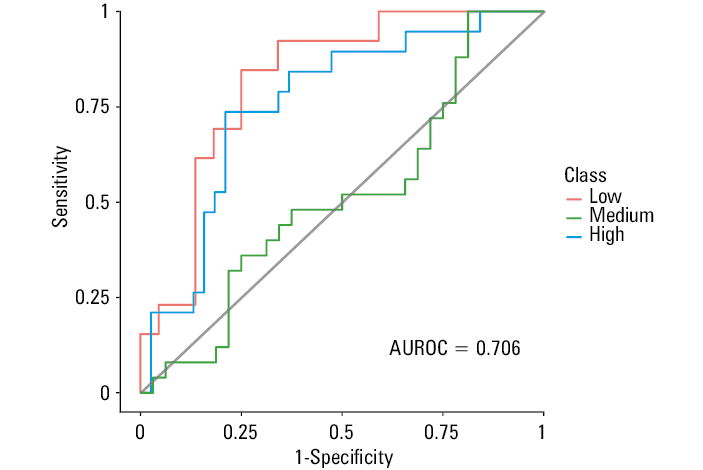
Abbreviations: see Figure 2
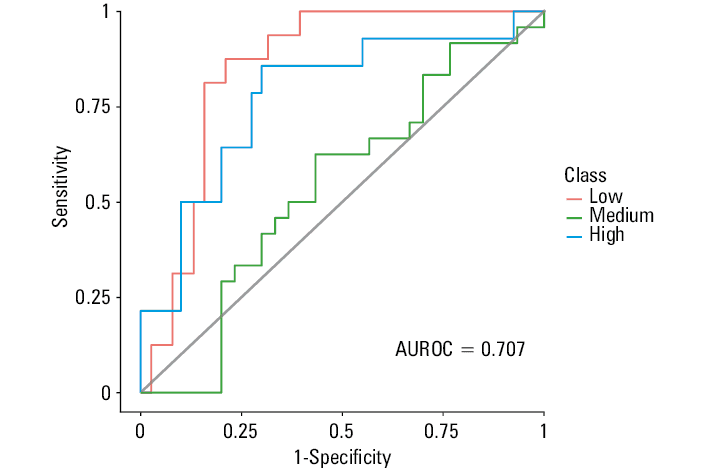
Abbreviations: see Figure 2
Discussion
Our study showed that AF does not affect the degree of reperfusion, the risk of ICB, or the functional status of patients who underwent thrombectomy for stroke. Moreover, AF was shown to have a neutral effect on the status of patients both in the subacute (day 30) and chronic (day 90) phase of stroke. Older age, NIHSS score in the ultra‑acute phase of stroke, and the degree of reperfusion after MT (based on TICI grade) were significant predictors of the functional status of all patients after MT. In our study, patients with AF constituted more than one‑fourth of all patients eligible for MT. The percentage of stroke patients with AF undergoing MT was reported to range from 25% to 50%.6-9,11 Patients with an INR higher than 3 were previously considered ineligible for MT in some centers. However, this is no longer a threshold for performing MT according to current guidelines, which resulted in an increased percentage of AF patients eligible for the procedure.
In our study, more than half of AF patients undergoing MT had a history of intravenous thrombolysis. According to the literature, 26% to 80% of patients with AF treated with endovascular therapy undergo thrombolysis, and this percentage is lower than that reported for patients without AF treated with MT.6,9,11 The primary exclusion criterion for rtPA threrapy is prior anticoagulation. Although three‑fourths of our patients received anticoagulation before the onset of stroke, more than 30% of those treated with VKAs did not achieve a therapeutic INR. Our results are in line with previous studies.6,9 To date, numerous investigators demonstrated that AF‑related stroke is associated with greater morphological damage to the neural tissue, a higher risk of hemorrhagic transformation, a more severe clinical course, and a poorer functional status of patients with higher mortality in the acute period and at 12‑month follow‑up.4-16,22,30,31 In our study, patients with AF were older and more often had poor functional status at all follow‑up time points than patients without AF. In addition, they more often underwent hemicraniectomy because of clinical deterioration and poor neuroimaging findings. Finally, they significantly more often presented with structural and functional cardiac abnormalities than patients without arrhythmia.
Previous studies reported inconsistent results for the effect of AF on the outcome of reperfusion therapy, but they more often evaluated links with rtPA. As for the association between AF and MT outcome, only a few studies are available and their results are also conflicting.32,33 The subanalysis of the MR CLEAN trial did not confirm a significant effect of AF on MT outcome.11,22 Several individual retrospective studies reported a negative effect of AF on the functional status of patients undergoing endovascular therapy for stroke.8 In addition, the STAR (Stroke Thrombectomy and Aneurysm Registry) registry of data from more than 4000 patients undergoing MT showed no negative effect of AF on MT outcome.8 These results are consistent with our study. Akbik et al8 identified several independent factors for unfavorable prognosis in patients with AF, including advanced age, lower ASPECTS score, and higher NIHSS score.8 On the other hand, patients with AF showed a shorter time to arterial occlusion, a higher rate of first pass success, and fewer passes than those free from AF. This can be explained by the structure of a cardiac embolism (lower fibrin content than in an arterio‑arterial embolism) possibly facilitating the manipulation of the thrombus during the procedure. Another possible explanation could be the exposure of thrombus to anticoagulant therapy. Interestingly, 40% of our patients (including 46% of those with AF) did not receive rtPA before MT, while rtPA can potentially modify the outcome of MT. This may explain the discrepancies between studies.
According to the literature, at least half of the patients with AF receive antithrombotic therapy before MT. This affects the rate of hemorrhagic stroke transformation in those undergoing reperfusion therapy during stroke. In this study, we evaluated the potential effect of prior anticoagulant therapy. However, no significant associations between study parameters were revealed. In our patients, previous thrombolytic therapy had no effect on the outcome of MT. In line with our results, Akbik et al8 reported no increase in the rate of ICB after MT in AF patients.8 On the other hand, Huang et al6 described a significant increase in ICB rates in AF patients after MT compared with those without AF. However, it did not have any significant effect on their functional status or mortality at 3 months after stroke. Patients taking VKAs have an increased risk of symptomatic ICB and mortality after MT compared with those receiving DOACs.34 However, this excess risk was associated neither with an INR value by the time thrombectomy was performed nor with a worse functional outcome or mortality at 3 months.35 An improved selection might be advisable in patients using VKAs. It is known that in selected patients with ischemic stroke receiving DOACs, rtPA has a safety profile similar to that in patients on subtherapeutic VKA treatment and in those without previous anticoagulation.36 This is important for the optimal selection of patients with AF and stroke for reperfusion therapy, also during anticoagulation. Of note, there are other risk factors for hemorrhage in patients on thrombolysis, regardless of the previous exposure to anticoagulation.37 In general, MT is considered to be safe in terms of the risk of increased ICB in patients on anticoagulant therapy.38-45 Its safety and efficacy was reported in anticoagulated patients ineligible for thrombolysis, with observed hemorrhage rates similar to those in patients who did not receive anticoagulant therapy.45 An analysis from the German Stroke Registry revealed no effect of the anticoagulation status on favorable outcome at 3 months.46 This finding has importantant implications for the safety of anticoagulant therapy in patients with AF.47
Leker et al9 reported that the safety and efficacy of MT did not differ depending on whether AF was diagnosed before stroke or whether it was detected during the causative diagnosis of stroke. This indicates that anticoagulation does not affect the final outcome of endovascular therapy. Previous studies revealed that patients treated with warfarin derived greater benefits from stroke treatment.48,49 However, this refers to a heterogeneous group of patients in terms of the arterial occlusion site and the therapeutic modalities in the acute phase of stroke.
It is possible that MT suppresses the unfavorable effects of AF, but this issue requires further research. As mentioned above, in addition to increasing the risk of stroke, AF is associated with a more severe course of the disease and a higher risk of recurrence and death. One of the causes of severe stroke in these patients is a large cardiac thrombus occluding the lumen of a large artery, which results in significant brain damage. The limited available data suggest that, with thrombectomy, it is easier to remove a cardiac thrombus than to remove a thrombus on the surface of athrosclerotic plaque. The use of rtPA before MT can additionally alter the thrombus structure, thus facilitating its mechanical removal. Therefore, further research is needed to investigate whether rtPA should be routinely used before MT, including cases when endovascular treatment can be started earlier (eg, in the mothership model of a stroke network). In patients on anticoagulant therapy, with large vessel occlusion, the decision on intravenous thrombolysis should not delay thrombectomy. Precision medicine using a tailored approach to both the clinical and radiological information (including the penumbra and vessel status), oral anticoagulation and the use of specific reversal agents—only if necessary—seems a reasonable option. According to the latest research, patients who receive combined reperfusion therapy (rtPA with MT) have better clinical outcomes than those who receive MT alone. This finding may demonstrate a true benefit of rtPA use before MT.50 The results of ongoing studies are anticipated, as they may bring some changes to patient selection for thrombectomy, which is also related to some of the issues presented in this paper.
Our study has several limitations, including a single‑center, retrospective design, the lack of some data for all patients, and no assessment of MT outcomes in relation to the type of thrombectomy.
In conclusion, AF does not affect the outcome of MT in patients with acute stroke. Age, the degree of postinterventional reperfusion, and the neurologic status in the ultra‑acute phase of stroke have the strongest effect on the functional status of patients undergoing MT. The use of anticoagulant therapy before stroke does not increase the risk of symptomatic ICB after MT in these patients.
- Goyal M, Menon BK, van Zwam WH, et al. Endovascular thrombectomy after large‑vessel ischaemic stroke: a meta‑analysis of individual patient data from five randomised trials. Lancet. 2016; 387: 1723‑1731. | Crossref
- Zhang YH, Shi MC, Wang ZX, et al. Factors associated with poor outcomes in patients undergoing endovascular therapy for acute ischemic stroke due to large‑vessel occlusion in acute anterior circulation: a retrospective study. World Neurosurg. 2021; 149: 128‑134. | Crossref
- Kim JT, Liebeskind DS, Jahan R, et al. Impact of hyperglycemia according to the collateral status on outcomes in mechanical thrombectomy. Stroke. 2018; 49: 2706‑2714. | Crossref
- Goyal N, Tsivgoulis G, Pandhi A, et al. Admission hyperglycemia and outcomes in large vessel occlusion strokes treated with mechanical thrombectomy. J Neurointerv Surg. 2018; 10: 112‑117. | Crossref
- Broocks G, Kemmling A, Aberle J, et al. Elevated blood glucose is associated with aggravated brain edema in acute stroke. J Neurol. 2020; 267: 440‑448. | Crossref
ARTICLE INFORMATION