Contrast‑enhanced computed tomography features of a rare case of cystic primary hepatic angiosarcoma



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Contrast‑enhanced computed tomography features of a rare case of cystic primary hepatic angiosarcoma
A 70‑year‑old man presented to the hospital with recurring right upper abdominal pain and abdominal distension with no apparent cause. Except for hypertension, his medical history was unremarkable. He denied any known exposure to carcinogens. Physical examination showed that the lower liver boundary was 3 cm below the costal area. Assessment of tumor markers showed elevated levels of carbohydrate antigen (CA) 19‑9 (77.16 U/ml; reference range, 0–37 U/ml) and interleukin 6 (219.5 pg/ml; reference range, 0–7 pg/ml). In liver function tests, levels of total protein, albumin, and alkaline phosphatase were 63.7 g/l (reference range, 65–85 g/l), 32.5 g/l (reference range, 40–55 g/l), and 187 U/l (reference range, 45–125 U/l), respectively, and other liver function indices were normal. On admission, the patient underwent imaging examinations (Figure 1A–1F), including contrast‑enhanced ultrasound (CEUS), magnetic resonance imaging (MRI), and contrast‑enhanced computed tomography (CECT). Imaging studies demonstrated an enlarged liver containing multiple cysts and solid masses which were considered malignant. Subsequently, the patient underwent a resection of the largest tumor localized in the right lobe of the liver (Figure 1G–1H). The tumor was round, with solid and cystic components, and it was invading the diaphragm. Pathological examination showed that it was a malignant spindle cell tumor, with no capsule formation. Immunohistochemistry showed that tumor cells were positive for CD31, CD34, F8, CD99, and the Ki‑67 percentage score was over 50%, which supported the diagnosis of hepatic angiosarcoma. The patient was lost to follow‑up as he did not return to the hospital after tumor resection.
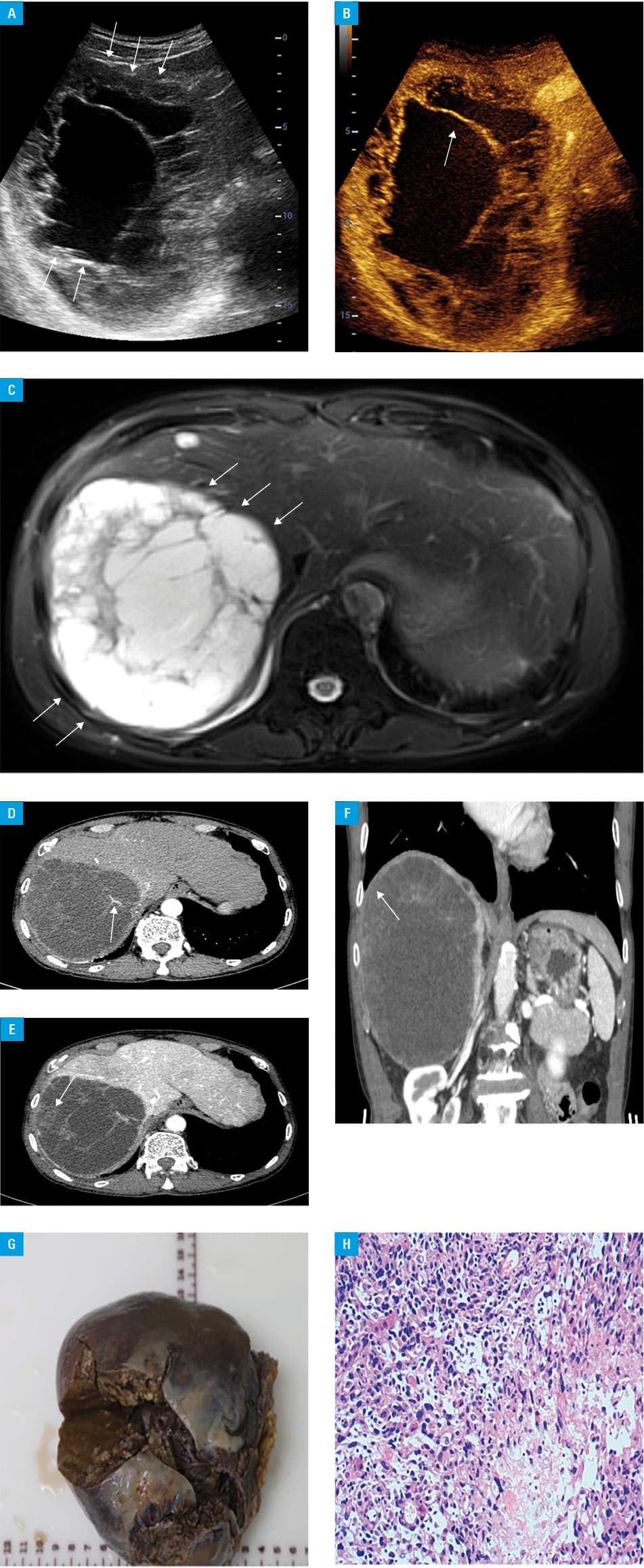
Due to the absence of specific clinical manifestations and laboratory findings indicating primary hepatic angiosarcoma (PHA), the diagnostic value of imaging studies is reasonably emphasized.1 To our knowledge, the current study represents the second published case of cystic PHA, following that reported by Cano‑García et al,2 and the first case to describe the imaging features of cystic PHA in detail. We suggest PHA should be included in the differential diagnosis of hepatic tumors. Benign lesions such as cystic hepatic echinococcosis have thin and uniform cyst walls without any contrast enhancement on scans. In addition, they can be distinguished from cystic PHA by unique imaging features such as the floating band sign. In our patient, based on CECT, the largest mass was located in the right liver lobe and showed uneven thickness and progressive enhancement of the capsule wall, with blood vessels traversing through it. Additionally, CECT showed an unclear boundary between the largest mass and the diaphragm. The above findings may be used as differential characteristics to distinguish PHA from other diseases. Rademaker et al3 suggested that the combined use of common hepatic angiography and dual‑phase helical CT can lead to more accurate identification of PHA. CECT, MRI, and CEUS have a similar diagnostic accuracy in evaluating the malignant degree of focal liver lesions.4 However, unlike CEUS, CECT can provide detailed visualization of the liver and the entire abdomen. Compared with MRI, CECT examination takes less time and is better tolerated by patients. For this disease, CECT may be a useful imaging modality, but more experimental data are required.
- Zhu YP, Chen YM, Matro E, et al. Primary hepatic angiosarcoma: a report of two cases and literature review. World J Gastroenterol. 2015; 21: 6088‑6096. | Crossref
- Cano‑García F, Athie‑Athie AJ, García‑Gómez JI, et al. Cystic angiosarcoma of the liver. A previously undescribed neoplasm. Ann Hepatol. 2016; 15: 283‑286.
- Rademaker J, Widjaja A, Galanski M. Hepatic hemangiosarcoma: imaging findings and differential diagnosis. Eur Radiol. 2000; 10: 129‑133. | Crossref
- Burrowes DP, Medellin A, Harris AC, et al. Characterization of focal liver masses: a multicenter comparison of contrast‑enhanced ultrasound, computed tomography, and magnetic resonance imaging. J Ultrasound Med. 2021, 40: 2581‑2593. | Crossref
ARTICLE INFORMATION