Acute-on-chronic pulmonary embolism and concomitant paradoxical embolism: two diseases, one intervention



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Acute-on-chronic pulmonary embolism and concomitant paradoxical embolism: two diseases, one intervention
Pulmonary embolism (PE) is one of the most common cardiovascular diseases.1 Interventional PE therapies are indicated in patients with contraindications to systemic thrombolysis.2 We report on the successful interventional treatment of acute PE on top of chronic thromboembolic pulmonary hypertension (CTEPH).
A 56‑year‑old woman was admitted to a peripheral hospital with ischemic stroke, which was treated conservatively. Following the admission, acute heart failure suddenly developed (oxygen saturation, 67%; tachycardia with a rate of 120 bpm; blood pressure, 75/40 mm Hg, despite dobutamine and noradrenaline support). The patient was intubated and transferred to the intensive care unit. Pulmonary embolism was suspected. Computed tomography revealed massive emboli in the pulmonary arteries and a thrombus in the descending aorta. High‑risk PE was diagnosed and the local PE Response Team (PERT) was activated. An interdisciplinary teleconsultation including a treating physician, interventional cardiologists, an intensive care specialist, and a cardiothoracic surgeon was performed within 30 minutes. Considering the critical state and contraindications to systemic thrombolysis, the patient was qualified for percutaneous therapy and transported to the PE reference center.3
Bedside echocardiography at admission demonstrated right ventricle dilatation (49 mm); moderate tricuspid regurgitation (tricuspid regurgitation peak velocity, 3.5 m/s); dilated vena cava (26 mm) without collapse; increased estimated systolic pulmonary artery pressure (64 mm Hg); dilated pulmonary trunk (28 mm); and patent foramen ovale with a right‑to‑left shunt. Pulmonary angiography showed dilated and tortuous pulmonary arteries, ring‑like and web‑like thromboembolic lesions, and chronic total occlusions, indicating CTEPH, overlapping with fresh emboli (Figure 1A and 1B). The mean pulmonary artery pressure was 50 mm Hg. Percutaneous mechanical thrombectomy using Cleaner XT Rotational Thrombectomy System (Argon Medical Devices, Plano, Texas, United States) was performed in the branches of the left and right pulmonary arteries. Chronic total occlusions were treated with balloon angioplasty (Figure 1C and 1D), leading to hemodynamic improvement.
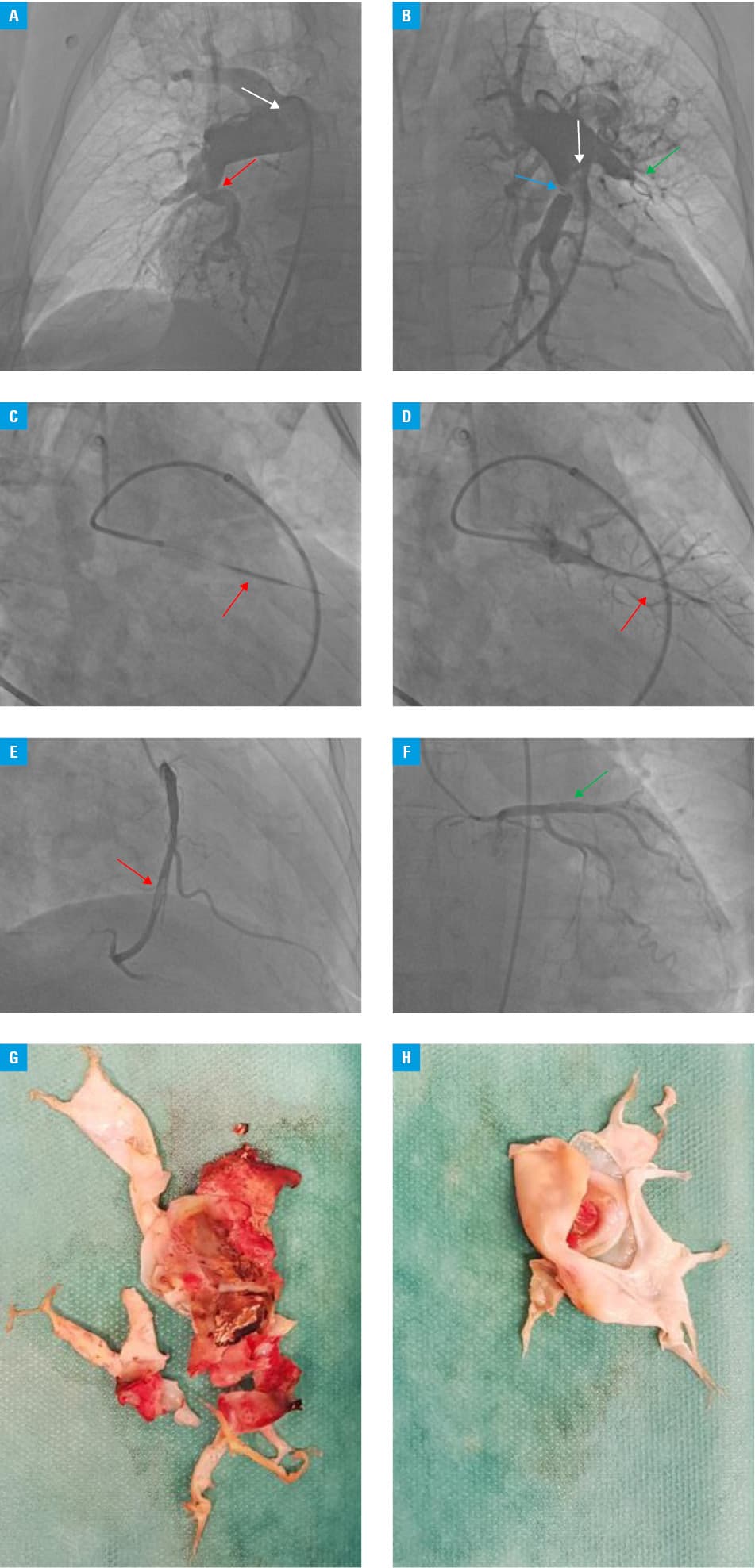
Due to the suspicion of paradoxical embolism as the cause of stroke and the thrombus in the descending aorta, coronary angiography was performed, showing an organized thrombus in the right coronary artery (RCA; Figure 1E) and a patent stent in the left anterior descending artery (Figure 1F). Since there were no signs of acute inferior wall ischemia on electrocardiography and no regional wall motion abnormalities on echocardiography, no intervention was undertaken. Three days later, the patient was extubated. Control echocardiography demonstrated normal left ventricular ejection fraction, persistent right ventricle dilatation (45 mm), and estimated systolic pulmonary artery pressure of 60 mm Hg. Following the in‑hospital rehabilitation, the patient presented with only mild motor impairment of the left arm. Single‑photon emission computed tomography showed reversible ischemia of the inferior wall, corresponding to the RCA supply region. Prior to the hospital discharge, the patient was qualified for elective surgical embolectomy, patent foramen ovale closure, and RCA bypass grafting by PERT. Considering the planned surgical treatment, she received anticoagulation with a therapeutic dose of enoxaparin. Elective surgical embolectomy, which was performed 3 months later, enabled the extraction of the well‑organized thrombi from pulmonary arteries (Figure 1G and 1H).
In summary, we present therapeutic challenges in a patient with acute PE on top of CTEPH and probable paradoxical embolism, based on the right‑to‑left shunt visible on echocardiography and RCA thrombus. We emphasize the role of PERT in treatment implementation in such patients.4
- Turetz M, Sideris AT, Friedman OA, et al. Pulmonary embolism: epidemiology, pathophysiology, and natural history of pulmonary embolism. Semin Intervent Radiol. 2018; 35: 92‑98. | Crossref
- Kurzyna M, Pietrasik A, Opolski G, et al. Contemporary methods for the treatment of pulmonary embolism: is it prime‑time for percutaneous interventions? Kardiol Pol. 2017; 75: 1161‑1170. | Crossref
- Konstantinides SV, Meyer G, Becattini C, et al. 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS) the Task Force for the diagnosis and management of acute pulmonary embolism of the European Society of Cardiology (ESC). Eur Heart J. 2020; 41: 543‑603.
- Araszkiewicz A, Kurzyna M, Kopeć G, et al. Expert opinion on the creating and operating of the regional Pulmonary Embolism Response Teams (PERT). Polish PERT Initiative. Cardiol J. 2019; 26: 623‑632. | Crossref
ARTICLE INFORMATION