Profound neutropenia related to consolidation durvalumab treatment following concurrent radiochemotherapy in a patient with stage III non–small‑cell lung cancer



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Profound neutropenia related to consolidation durvalumab treatment following concurrent radiochemotherapy in a patient with stage III non–small‑cell lung cancer
With the development of novel techniques of concurrent radiochemotherapy, the expected 5‑year overall survival of patients with stage III non–small‑cell lung cancer is about 30%, with local and regional control up to 80% and 90%, respectively.1 Since 40% to 50% of patients fail at distant sites, many options for consolidation systemic treatment have been investigated. Durvalumab is a selective human monoclonal antibody blocking programmed cell death ligand 1, enhancing host immune response against cancer. The pivotal PACIFIC study showed a 3‑year overall survival of 57% and 44% for durvalumab and placebo, respectively.2 However, activation of the immune system by immune checkpoint inhibitors (ICIs) may induce a broad spectrum of immune‑related adverse events (irAEs). The most frequently affected organs are the skin, lungs, intestines, endocrine glands, and liver.3 As opposed to chemotherapy, hematotoxicity of ICIs is anecdotal.
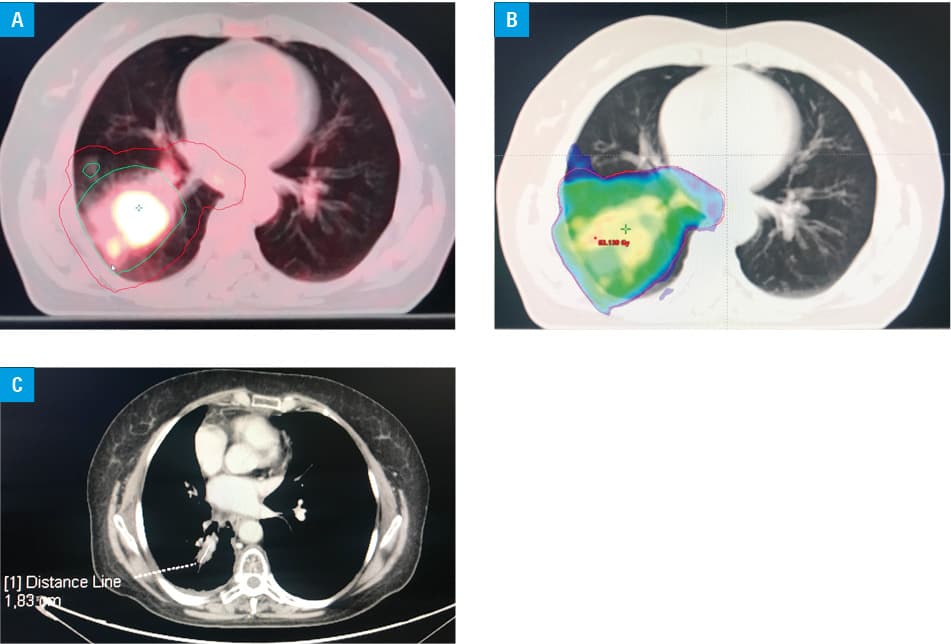
We present a case of a 60‑year‑old woman diagnosed with cT3N2M0 squamous cell carcinoma of the right lung in March 2018. She was administered intensity‑modulated radiotherapy (dose, 60 Gy/30 fractions) concurrently with cisplatin and etoposide (Figure 1A and 1B). Due to esophageal mucositis after the first cycle of chemotherapy, radiotherapy was interrupted for 1 week. After completion of radiochemotherapy, the patient received 16 cycles of consolidation durvalumab (10 mg/kg every 2 weeks; Supplementary material, Table S1).2 Treatment was complicated by profound neutropenia resulting in neutropenic fever. In view of the normal neutrophil count before treatment, neutropenia was considered an irAE. The patient was prescribed prednisone (1 mg/kg), antibiotics (amoxicillin / clavulanic acid, clarithromycin), and granulocyte colony‑stimulating factor (G‑CSF). Bone marrow biopsy showed all hematopoietic cell lines without significant dysplasia, cellularity between 25% and 30%, absent fibrosis, plasma cell level of 3%, and no cancer infiltration. After immunosuppressive treatment and 2 weeks of G‑CSF therapy, the absolute neutrophil count increased, enabling slow tapering of prednisone. Chest computed tomography showed partial regression of the tumor (Figure 1C). After 2 years of follow‑up, the patient is doing well, without cancer progression or persistent neutropenia.
Postulated mechanisms of ICI‑induced neutropenia include T‑cytotoxic cells infiltration, hematopoietic dysfunction, and autoimmunization.4 Differential diagnosis of possible causes of neutropenia include medications, sepsis, rheumatologic disorders, bone marrow malignancies, vitamin deficiency, autoimmunization, and viral infections (parvovirus B19, Ebstein–Barr Virus, cytomegalovirus, HIV, hepatitis).5 In our case, baseline autoimmune diseases, HIV and hepatitis B and C infections, as well as potentially myelotoxic drugs were excluded.
Hematologic irAEs of ICIs have been reported occasionally (incidence of 1%), but may be fatal.3,4 The primary management of ICI‑induced neutropenia includes ICI discontinuation and immunosuppression with steroids as a backbone. Salvage options include immunosuppressive agents (eg, tocilizumab or cyclosporine) and intravenous immunoglobulins.4 Since febrile neutropenia could lead to fatal bacterial or fungal infections, essential elements of treatment are prompt antimicrobial therapy and G‑CSF support.3,4
To our knowledge, this is the first reported case of profound neutropenia after consolidative treatment with durvalumab. In the PACIFIC trial, drug‑induced neutropenia did not occur in any of the 473 patients taking durvalumab.2 The incidence of immune‑related neutropenia may increase in the future due to the sharply rising use of durvalumab and other ICIs.
- Łazar‑Poniatowska M, Bandura A, Dziadziuszko R, Jassem J. Concurrent chemoradiotherapy for stage III non‑small‑cell lung cancer: recent progress and future perspectives (a narrative review). Transl Lung Cancer Res. 2021; 10: 2018‑2031. | Crossref
- Gray JE, Villegas A, Daniel D, et al. Three‑year overall survival with durvalumab after chemoradiotherapy in stage III NSCLC – update from PACIFIC. J Thorac Oncol. 2020; 15: 288‑293. | Crossref
- Haanen JBAG, Carbonnel F, Robert C, et al. Management of toxicities from immunotherapy: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow‑up. Ann Oncol. 2017; 28 (Suppl 4): iv119‑iv142. | Crossref
- Finkel I, Sternschuss M, Wollner M, et al. Immune‑related neutropenia following treatment with immune checkpoint inhibitors. J Immunother. 2020; 43: 67‑74. | Crossref
- Rogers BB, Zawislak C, Wong V. Management of hematologic adverse events associated with immune checkpoint inhibitors. J Adv Pract Oncol. 2021; 12: 392‑404. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION