Catamenial pneumothorax: estrogen receptors staining may prompt a diagnosis. A case study



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Catamenial pneumothorax: estrogen receptors staining may prompt a diagnosis. A case study
Catamenial pneumothorax (CPTX) is a recurrent, usually right‑sided pneumothorax (PTX) which occurs spontaneously up to 24 hours before, or up to 72 hours from the onset of menses.1 Studies in women of reproductive age show that CPTX is diagnosed in 7.3% to 36.7% of PTX cases.2 CTPX is most commonly, yet not exclusively, associated with endometriosis, and is its most frequent thoracic manifestation.1 Four main possible mechanisms of CPTX pathogenesis have been proposed: i) menses‑dependent passage of the air from the genital tract through diaphragmatic fenestrations (both congenital and acquired), including those produced by endometrial implants; ii) infiltration of visceral pleura by endometrial tissue; iii) alveolar or bleb rupture caused by bronchiolar constriction in response to menses‑dependent prostaglandin rise; and iv) bronchiolar constriction induced by an endometrial implant.1 Recently, a possible fifth mechanism has been postulated; namely, sloughing of endometrial cells in lung parenchyma promoting bullae formation,3 which was based on histopathological results of the specimens acquired during thoracoscopy in 3 patients with CTPX and apical bullae. No overt endometrial cells were revealed; however, some of the epithelial and stromal cells stained positively for estrogen (ER) and progesterone receptors. No other features characteristic of endometriosis were found in these patients, yet there was no CTPX recurrence after hormonal therapy. In light of the above, a retrospective case analysis of 6 CTPX patients who were repeatedly admitted to University Clinical Center in Gdańsk was performed. None of the patients had a confirmed pelvic endometriosis. No patient had alpha‑1 antitripsin deficiency. One individual was excluded due to the lack of biological material (the patient refused surgery); nonetheless, no apical bullae were visible radiologically. Of the remaining 5 patients, only 1 had a pathological confirmation of thoracic endometriosis. It was diagnosed during thoracoscopy by histopathological examination of diaphragmatic nodules showing typical features of endometriosis, that is, both endometrial stroma and glandular epithelium.
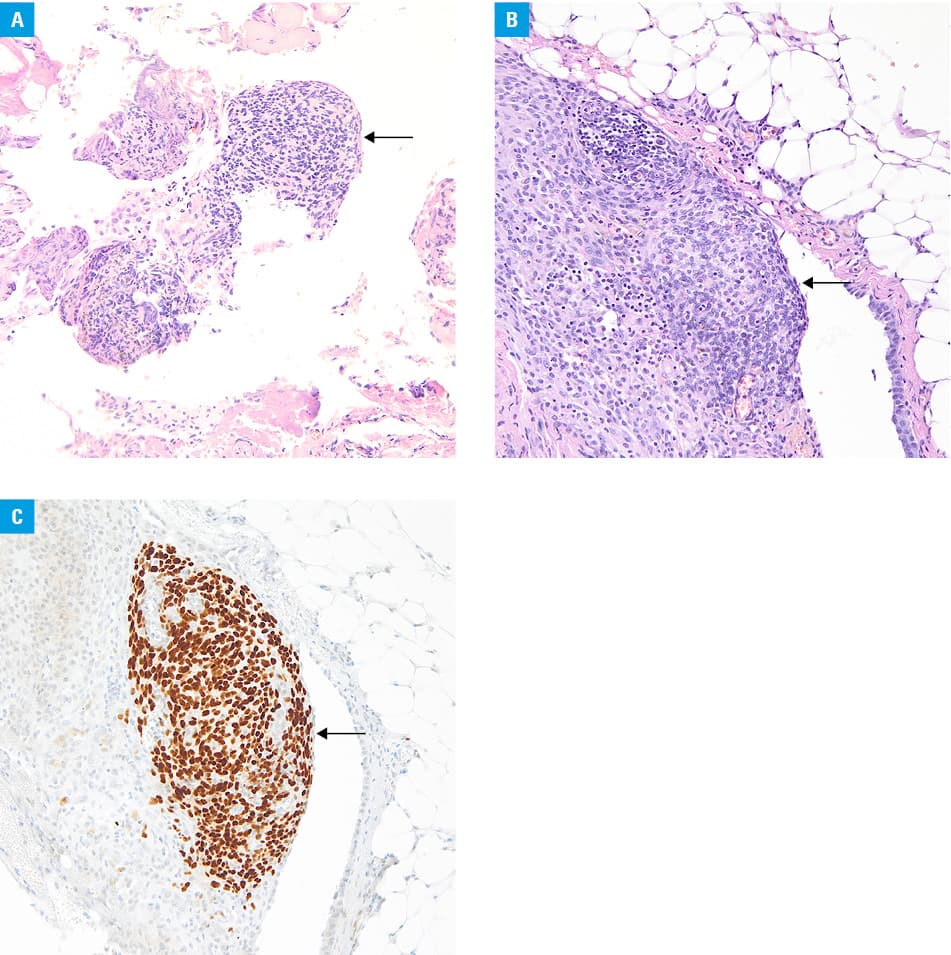
In the present analysis, the aforementioned bullae specimens were retrospectively evaluated with immunohistochemical staining for ER. ER staining was positive in 2 out of 5 patients. It was particularly important in the patient in whom a positive ER status of the visceral pleura chronologically preceded a later detection of diaphragmatic nodules during subsequent thoracoscopy, as mentioned above. In the other patient, positive ER staining of parietal pleura was the only evidence of thoracic endometriosis, and thus provided an explanation for previous positive response to hormonal treatment (Figure 1).
Our report supports the suggestion that thoracic endometriosis can be diagnosed by positive staining for ER in patients with CTPX, which was also postulated by other authors.4 Early diagnosis allows for timely introduction of hormonal treatment and may prevent further, often invasive, diagnostic procedures. Moreover, our findings add to the notion that apical bullae might be treated as one of the manifestations of thoracic endometriosis, as suggested in the past.5
- Bricelj K, Srpčič M, Ražem A, et al. Catamenial pneumothorax since introduction of video‑assisted thoracoscopic surgery. Wien Klin Wochenschr. 2017; 129: 717‑726. | Crossref
- Gil Y, Tulandi T. Diagnosis and treatment of catamenial pneumothorax: a systematic review. J Minim Invasive Gynecol. 2020; 27: 48‑53. | Crossref
- Kawaguchi Y, Fujita T, Hanaoka J. Catamenial pneumothorax with bullae. Ann Thorac Surg. 2015; 99: 1075‑1078. | Crossref
- Alifano M. Catamenial pneumothorax. Curr Opin Pulm Med. 2010; 16: 381‑386. | Crossref
- Kovarik JL, Toll GD. Thoracic endometriosis with recurrent spontaneous pneumothorax. JAMA. 1966; 196: 595‑597. | Crossref
ARTICLE INFORMATION