A 70‑year‑old man was referred to the Department of Neurology due to a 5‑year history of episodes of unpredictable weakness followed by dizziness, mainly when rising. The patient reported anosmia, recurrent diarrhea, and complained of “cold feet” and sleep disturbances (violent moving during nightmares; sometimes he had accidentally injured his wife during such episodes). Medical history of the patient included chronic ischemic heart disease, hypercholesterolemia, impaired fasting glycemia, gout, intestinal diverticulosis, and sleep apnea.
During the initial diagnostic work‑up, performed by endocrinologists and cardiologists, orthostatic hypotension (OH) was diagnosed, along with a slightly impaired baroreflex function during the tilt test. Holter monitoring, echocardiography, and diagnostic coronary angiography did not reveal any abnormalities.
Upon admission to the Department of Neurology, no abnormalities were found on neurological examination. Magnetic resonance imaging of the head (T2‑weighted image) showed limited, bilateral, subcortical white matter hyperintensities, presumably of vascular origin. Neuropsychological tests were unremarkable, while laboratory tests only revealed normocytic anemia (hemoglobin level, 12.2 g/dl; reference range, 14.0–18.0 g/dl; hematocrit, 36.4%; reference range, 40%–54%; mean corpuscular volume, 87.9 fl; reference range, 80.0–96.0 fl).
Given the dysautonomic nature of the chief symptoms, we performed a comprehensive autonomic system evaluation, including standard cardiovascular autonomic tests (deep breathing, Valsalva maneuver, head‑up tilt) with continuous R‑R interval and blood pressure monitoring (TaskForce Monitor; CNSystems Medizintechnik GmbH, Graz, Austria), and sympathetic skin response assessment (VikingQuest; Natus, San Carlos, California, United States).1 The results showed severe autonomic, primarily sympathetic dysfunction (Figure 1A–1D).1 Peripheral neuropathy and myopathies were excluded, as was transthyretin‑related familial amyloid polyneuropathy.
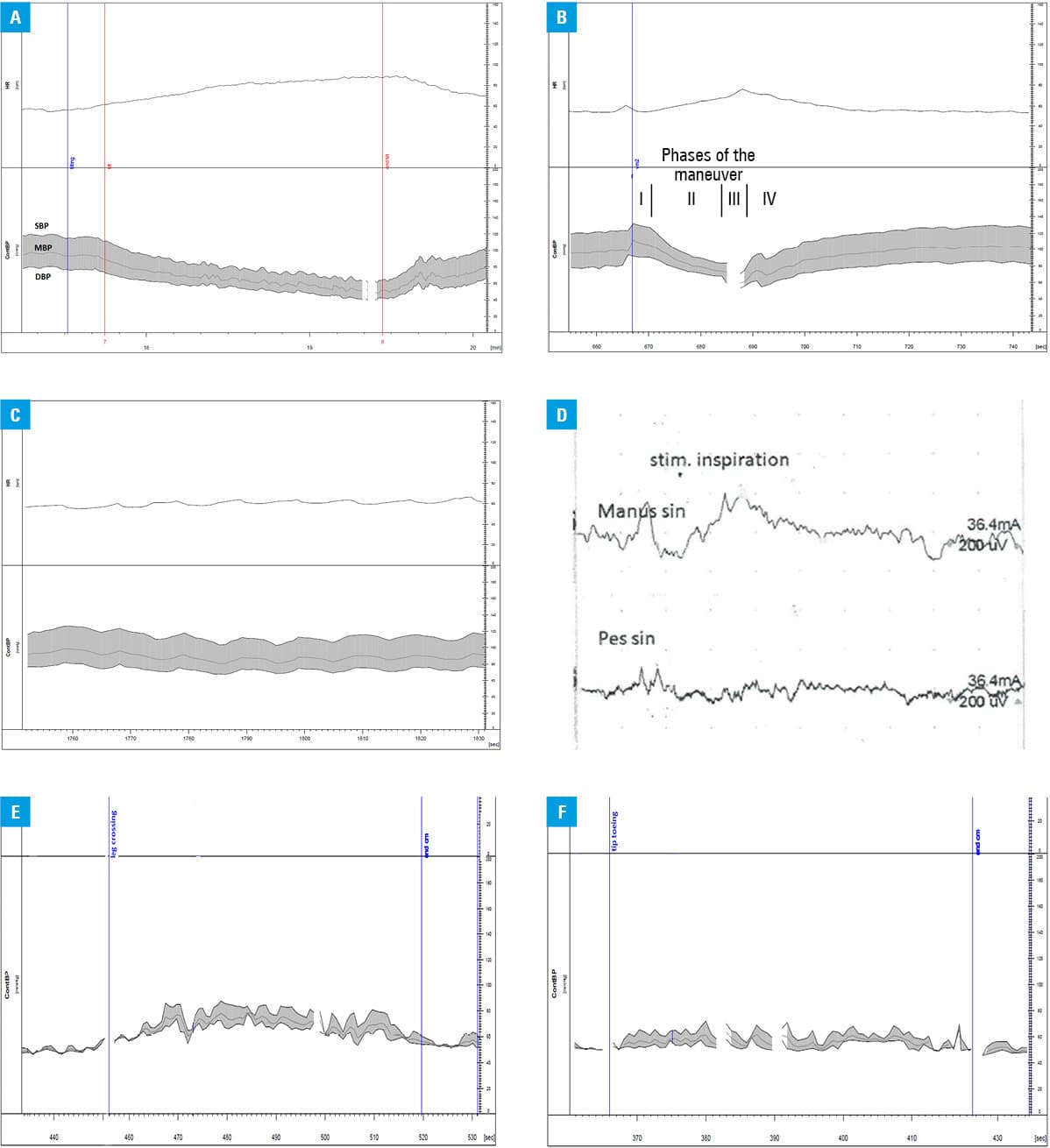
In light of all the findings, pure autonomic failure (PAF) was suspected. A liquid diet high in sodium was introduced together with midodrine (5 mg twice daily), fludrocortisone (0.1 mg/d), and pyridostigmine (20 mg thrice daily to avoid supine hypertension) treatment, which led to improvement of the patient’s condition. In addition, physical counter‑maneuvers were applied (Figure 1E–1F).2
PAF is a rare, sporadic neurodegenerative disorder with noradrenergic nerve fiber loss that gives rise to a postganglionic pattern of autonomic denervation due to cytoplasmic inclusions of α-synucleins termed Lewy bodies in the neurons. The disease is more prevalent in men. The diagnosis is based on the presence of OH, usually with the evidence of widespread failure; approximately half of patients have concomitant supine hypertension. Autonomic failure may lead to genitourinary, bowel, and thermoregulatory dysfunctions.3 More than 80% of patients have anosmia.4 There is no evidence of central nervous system dysfunction, although REM sleep behavior disorder occurs in 72% of cases.4 Subtle parkinsonian syndrome may be found and is indicative of a possible subsequent neurodegenerative conversion.5 Systemic involvement, for example, anemia, arterial hypertension, increased arterial stiffness, and renal dysfunction with mild proteinuria may be encountered.4
PAF should be considered in patients presenting with subacute to chronic OH without parkinsonism, dementia, neuropathy, or valvular heart disease, congestive heart failure, and chronic kidney disease. The diagnosis may be supported by imaging studies, that is, cardiac functional imaging with 123I‑metaiodobenylguanidine myocardial single‑photon emission computed tomography and 6-[18F]-fluorodopamine positron emission tomography, usually demonstrating decreased cardiac sympathetic innervation. Laboratory data may include low supine norepinephrine levels with minimal to no increase on standing.3 In the absence of neurologic symptoms, patients initially present to cardiologists, endocrinologists, gastroenterologists, or urologists, warranting multidisciplinary approaches. To date, PAF is incurable; clinical improvement may be achieved with nonpharmacologic and pharmacologic measures to control blood pressure fluctuations (Figure 1E–1F).2
- Ziegler D, Laux G, Dannehl K, et al. Assessment of cardiovascular autonomic function: age‑related normal ranges and reproducibility of spectral analysis, vector analysis, and standard tests of heart rate variation and blood pressure responses. Diabet Med. 1992; 9: 166‑175. | Crossref
- Wieling W, Colman N, Krediet CT, Freeman R. Nonpharmacological treatment of reflex syncope. Clin Auton Res. 2004; 14 (Suppl 1): 62‑70. | Crossref
- Coon EA, Singer W, Low PA. Pure autonomic failure. Mayo Clin Proc. 2019; 94: 2087‑2098. | Crossref
- Kaufmann H, Norcliffe‑Kaufmann L, Palma JA, et al. Natural history of pure autonomic failure: a United States prospective cohort. Autonomic Disorders Consortium. Ann Neurol. 2017; 81: 287‑297. | Crossref
- Coon EA, Mandrekar JN, Berini SE, et al. Predicting phenoconversion in pure autonomic failure. Neurology. 2020; 95: e889‑e897. | Crossref
ARTICLE INFORMATION