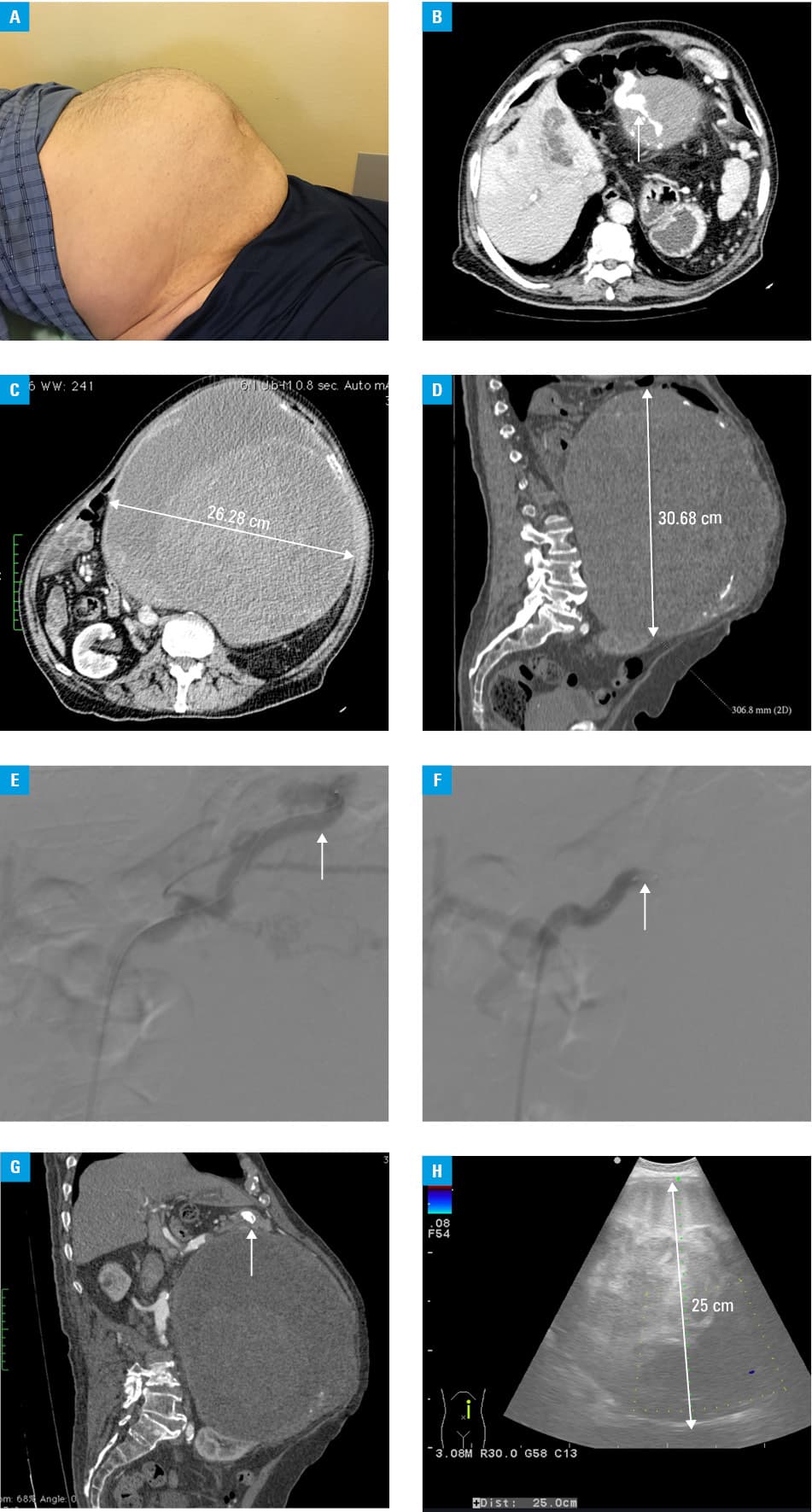
Splenic artery aneurysms (SAAs) are the most common, accounting for 60%–70% of all visceral artery aneurysms.1,2 A normal diameter of the splenic artery is approximately 0.5 cm. The splenic artery is considered aneurysmal when its diameter exceeds 1 cm.3 In true SAAs, the aneurysm involves all 3 layers of the vessel wall.2,3 Small SAAs (≤2 cm) are asymptomatic, and they are diagnosed incidentally when imaging is performed for another condition.2 Contrary to that, most giant SAAs (>5 cm) are symptomatic.2 The most common presenting symptom is left upper quadrant abdominal pain that may radiate toward the left shoulder.2 SAAs greater than 2 cm in diameter may be complicated by a rupture in 2%–10% of cases, resulting in life‑threatening intraabdominal bleeding.2,3 Therefore, for SAAs greater than 2 cm in diameter, surgical intervention rather than watchful waiting is advised.3 Giant splenic artery aneurysms are rare but the risk of rupture is as high as 28%.2 The management options for giant SAAs are open surgery, endovascular treatment, and laparoscopic surgery.3 There are only a few cases of giant SAAs, larger than 25 cm in diameter, reported in the literature.2,4 Herein, we present the case of a successful endovascular treatment of a giant (>26 cm) SSA. In August 2019, a 75‑year‑old male patient presented to the General Surgery Department of Wolski Hospital in Warsaw, Poland, with a 2‑week history of upper abdominal pain and significant enlargement of abdominal girth (Figure 1A). Computed tomography (CT) revealed a giant, 26 cm in diameter, aneurysm of the splenic artery (Figure 1B–1D). The patient’s comorbidities included persistent atrial fibrillation, hypertension, chronic obstructive pulmonary disease, hyperuricemia, obesity, and medical history of stroke. As the risk of open aneurysmectomy was high due to age, comorbidities, and size of the aneurysm, the patient was scheduled for endovascular closure of the splenic artery (Figure 1E). The splenic artery was successfully occluded with a 14‑mm vascular plug (Figure 1F). Follow‑up examination with Doppler ultrasonography (US) 3 and 6 months after the embolization revealed no flow in the aneurysmal sac (Figure 1G). Additionally, repeated US showed good blood perfusion of the spleen. Although the diameter of the aneurysm did not decrease (Figure 1H), embolization reduced the risk of rupture and relieved the patient’s pain. He returned to his daily activities. Follow‑up CT angiography performed in January 2021 confirmed no progression of the aneurysm in size and successful embolization with no blood flow in the aneurysmal sac. Embolization of the splenic artery proved to be an excellent, minimally invasive option. In this case, collateral vascular supply via the short gastric arteries to the spleen was preserved. Treatment of such large SAAs is challenging. In the past, open surgical intervention was considered a gold standard approach to SAA repair.4 Resection of an aneurysm can be combined with splenectomy.4 Preservation of the spleen is encouraged when possible but splenectomy should be performed if adequate hemostasis is impossible to achieve otherwise.5 Endovascular intervention has gained much popularity recently in managing SAAs. Techniques vary according to the type, size, and location of an aneurysm. Both management options have pros and cons. Open surgery offers excellent long‑term results but high perioperative mortality.3 Endovascular procedure shows low short‑term morbidity and mortality but higher reintervention rate due to long‑term complications.3 In our case, embolization of the splenic artery provided an excellent treatment result with a minimally invasive approach. The spleen, which has a good collateral vascular supply via the short gastric arteries, was preserved. Minimally invasive endovascular approaches would probably represent the ideal therapy for such aneurysms.
- Hosn MA, Xu J, Sharafuddin M, Corson JD. Visceral artery aneurysms: decision making and treatment options in the new era of minimally invasive and endovascular surgery. Int J Angiol. 2019; 28: 11‑16. | Crossref
- Akbulut S, Otan E. Management of giant splenic artery aneurysm: comprehensive literature review. Medicine (Baltimore). 2015; 94: e1016. | Crossref
- Hogendoorn W, Lavida A, Hunink MG, et al. Open repair, endovascular repair, and conservative management of true splenic artery aneurysms. J Vasc Surg. 2014; 60: 1667‑1676. | Crossref
- Pescarus R, Montreuil B, Bendavid Y. Giant splenic artery aneurysms: case report and review of the literature. J Vasc Surg. 2005; 42: 344‑347. | Crossref
- Aday U, Bozdağ E, Gündeş E, et al. Spleen‑preserving surgery in splenic artery aneurysm. Case Rep Surg. 2017; 2 017: 8716962. | Crossref
ARTICLE INFORMATION