Prevalence of self‑reported heart failure in the adult Polish population: results of the NATPOL 2011 study
Key words: heart failure, NT-proBNP level, NYHA scale, prevalence



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Prevalence of self‑reported heart failure in the adult Polish population: results of the NATPOL 2011 study
Introduction: Chronic heart failure (CHF) is a growing medical and economic problem, especially in Central and Eastern Europe. However, only a few studies analyzed the prevalence of CHF in this region.
Objectives: The aim of the study was to assess the prevalence of CHF in a representative sample of adult Poles.
Patients and methods: The NATPOL 2011 project was a cross‑sectional study of a representative sample of the adult Polish population that included 2413 individuals (1245 women, 1168 men) aged 18 to 79 years (mean [SD] age, 45.8 [16.7] years). All participants completed a detailed questionnaire and underwent laboratory tests. We evaluated the prevalence of CHF based on self‑reported symptoms, Polish National Health Fund database, and the N‑terminal pro–B‑type natriuretic peptide (NT‑proBNP) level.
Results: The proportion of patients that reported the diagnosis of CHF was 4.3% (95% CI, 3.6%–5.2%). Only 0.2% of people aged under 40 years reported CHF, compared with 3.2% of those aged 40 to 59 years and 13.2% of those aged 60 to 79 years. The distribution of NT‑proBNP levels in the patients with CHF was markedly skewed to the right, with the median value of 181 pg/ml (interquartile range, 90.8–531). Among the 104 individuals who declared having CHF, almost 56% had a record of at least 1 outpatient visit or hospitalization related to the ICD‑10 I50 code in the National Health Fund database, which translates to 2.4% of confirmed diagnoses of CHF in all Polish adults.
Conclusions: The results of our study indicated that the proportion of inhabitants of Poland aged 18 to 79 years with heart failure was somewhere between 2.4% and 4.3%. This corresponds to 720 000 to 1 200 000 of diagnosed CHF cases in Poland.
What's new?
The growing epidemic of chronic heart failure (CHF) has been highlighted by the World Health Organization and the European Society of Cardiology. There are only a few studies assessing the epidemiology of CHF in Europe and there are no such studies for the general population of Poland, which is one of the countries representing Central and Eastern Europe—a region of high cardiovascular risk. In this paper, we used the NATPOL 2011 study population to assess the current prevalence of heart failure in Poland based on a self‑reported previous diagnosis of heart failure, available medical records, data from the health care payer database (Narodowy Fundusz Zdrowia [NFZ], and the level of N‑terminal pro–B‑type natriuretic peptide. Previous diagnosis of CHF was reported by 4.3% of the NATPOL 2011 study participants, and in 2.4% of cases the diagnosis was confirmed in the NFZ database. These results are higher than the previous estimates of CHF prevalence. Obtaining reliable data on the number of patients with heart failure condition in Poland is necessary for an adequate health care planning.
Introduction
Chronic heart failure (CHF) is currently a major clinical problem, both in Poland and worldwide. However, while registries for other diseases, such as cancer, have been established, there is no national CHF registry. Previously, it was estimated that there are about 600 000 to 700 000 patients with CHF in Poland.1,2 Experts believe, however, that these Figures are likely underestimated, and the actual number of patients may be even twice as high and will continue to increase. Reasons for this include aging of the society along with an increasing access to interventional treatment of acute myocardial infarction and advances in drug therapy that have led to a longer survival of patients with CHF.
According to the most recent European Society of Cardiology (ESC) guidelines, the diagnosis of CHF should be made based on symptoms and imaging studies.3 The 2016 ESC guidelines introduced a diagnostic algorithm for CHF and highlighted the role of natriuretic peptides in the initial assessment. Increased blood levels of natriuretic peptides indicate an activation of a compensatory mechanism that precedes the development of clinical manifestations of heart failure (HF).4
The aim of the present study was to evaluate the prevalence of previously diagnosed CHF, determine the clinical characteristics of patients aware of their CHF diagnosis, and evaluate the distribution of N‑terminal pro–B‑type natriuretic peptide (NT‑proBNP) levels in this group, based on a representative sample of the Polish population.
Patients and methods
The NATPOL 2011 project was performed on a representative, random sample of the adult Polish population as of 2010 (women and men aged 18–79 years). Each noninstitutionalized Polish citizen had an approximately the same probability of being sampled. Sampling, study methodology as well as the protocol of blood sample collection, storage, and transport to the central laboratory were described in detail in a previous publication.5
In brief, a 3‑stage, stratified and clustering sampling procedure was employed. First, 61 territorial strata were defined by dividing all municipalities in each of the 16 Polish provinces into 4 classes: 1) rural, 2) urban with up to 50 000 inhabitants, 3) urban with 50 000 to 200 000 inhabitants, and 4) urban with more than 200 000 inhabitants. As the fourth category was lacking in some of the provinces, the final number of strata was 61. Then, for each stratum, the final number of study respondents was defined, proportionally to its population size. Next, in each stratum independently, municipalities were randomly chosen (248 municipalities in total) from the list of all municipalities in the stratum, proportionally to its population size. Then, in each of the urban and rural municipalities, streets and villages were drawn, respectively. The last stage was sampling of individual respondents living in the chosen streets and villages. The respondents were drawn from the Polish registry of citizens (the PESEL database) run by the Polish Ministry of Digital Affairs. The number of individuals drawn in each of the 12 demographic categories was proportional to the size of these categories within each territorial stratum. The categories were defined based on gender (male or female) and age (6 categories: 18–24, 25–34, 35–44, 45–54, 55–64, and 65–79 years). For each of the 2400 sampled study respondents, several reserve participants were drawn, and they were contacted only if the primary respondent was inaccessible for any reason or refused to take part in the study. The patients who refused or could not be contacted were later included in the denominator during calculation of the response rate. An attempt was made to contact 3634 drawn persons (excluding those for whom erroneous contact data were obtained). Ultimately, the study sample included 2413 individuals (1168 men, 1245 women), yielding a response rate of over 66%.
Blood samples were collected under fasting conditions in the respondents’ respective places of residence. The samples were centrifuged at local laboratories; plasma was frozen and transported to the central laboratory where biochemical testing was performed, including NT‑proBNP level measurements. Natriuretic peptide levels were measured with the immunochemiluminescence method using the Immulite 1000 system (Siemens Healthcare Diagnostics, Erlangen, Germany). The NT‑proBNP level was measured in 2258 participants. A cutoff level for plasma NT‑proBNP was defined as greater than 125 pg/ml, as per the current ESC guidelines.4
The patients with CHF were identified based on self‑declaration in response to the question: “Have you been diagnosed with CHF by a physician?” followed by verification using available medical records (diagnoses listed in hospital discharge documentation). All patients who answered “Yes” to the question or were able to provide medical documentation with a diagnosis of CHF were classified as those with CHF.
Due to the limitations of the questionnaire‑based approach, the prevalence of CHF in the study sample was also determined based on the health care payer (National Health Fund, Narodowy Fundusz Zdrowia [NFZ]) database. For this purpose, after the collection of data we requested information from the Section of Monitoring and Reporting at the NFZ about the patients in the NATPOL 2011 study sample who received health care services for CHF (outpatient visits to a cardiologist or a hypertension specialist and hospitalizations with the I50 code according to the International Classification of Diseases, 10th Revision [ICD‑10]) before the end of 2011 (registered before December 2011). Unfortunately, it was possible to match the data of only 1988 study participants (82.4%) with records from the NFZ database. This was caused by the fact that the merging of data was done using the participant’s date of birth, first name, and surname, while the unique national personal identification numbers (PESEL) of the study respondents were not available to the research team due to legal limitations.
The severity of CHF symptoms was assessed using the New York Heart Association (NYHA) classification. A questionnaire was used to evaluate the presence of ischemic heart disease (including previous myocardial infarction), atrial fibrillation, and chronic obstructive pulmonary disease. The patients were also asked about their smoking status and all medications taken. Hypertension was diagnosed if blood pressure was equal or greater than 140/90 mm Hg at 2 separate visits, and in patients who declared taking antihypertensive medications.6 Diabetes was diagnosed based on patient declaration or when the fasting plasma glucose level was equal or greater than 7 mmol/l (single measurement).7 Chronic kidney disease was diagnosed in participants with a reduced estimated glomerular filtration rate (eGFR <60 ml/min/1.73 m2) or eGFR ≥60 ml/min/1.73 m2 with concomitant albuminuria (albumin‑to‑creatinine ratio ≥30 mg/g).8
The NATPOL 2011 study was approved by the Bioethics Committee of the Medical University of Gdansk. Prior to recruitment, each participant gave informed consent to participate.
Statistical analysis
Continuous variables were shown as mean (SD) or median and interquartile range (IQR) for skewed distribution of data. Categorical data were shown as numbers (frequencies) and percentages. The Shapiro–Wilk test was used to check whether a variable was normally distributed. Quantitative variables were compared between the groups with the t test or the Mann–Whitney test, and qualitative variables were compared with the χ2 test or the Fisher test.
Age distribution was significantly different between the groups of patients with and without CHF. To control the age difference, the exact matching approach was used. Each patient with CHF was matched to a randomly assigned patient of the same age and sex from the non‑CHF group.
All statistical analyses were performed using the R package, version 3.2.3 (the R Foundation for Statistical Computing, Vienna, Austria). A P value below than 0.05 was considered significant.
Results
The characteristics of the study group are shown in Table 1. The study included participants aged 18 to 79 years (mean [SD] age, 45.8 [16.7] years; men, 44.9 [16.0] years; women, 46.7 [17.2] years). The level of NT‑proBNP was measured in 2258 individuals. The range of the NT‑proBNP level was 20.0–5717.0 pg/ml, and the median level was 64.5 pg/ml (IQR, 38.2–119). A previous diagnosis of HF was reported by 4.3% of the participants (95% CI, 3.6%–5.2%). The mean (SD) age of patients with CHF was 66.2 (9.9) years (men, 64.9 [9.7] years; women, 67.3 [10.0] years).
Parameter | NATPOL 2011 (n = 2413) | CHF (n = 104) | |
Data are presented as number (percentage) of patients unless indicated otherwise.
a Data available for 2258 patients from the NATPOL 2011 group and 95 patients from the CHF subgroup
Abbreviations: BMI, body mass index; CHF, chronic heart failure; IQR, interquartile range; NT‑proBNP, N‑terminal pro–B‑type natriuretic peptide | |||
Sex | Female | 1245 (51.6) | 56 (53.8) |
Male | 1168 (48.4) | 48 (46.2) | |
Age, y | Mean (SD) | 45.81 (16.67) | 66.2 (9.9) |
18–39 | 748 (31) | 1 (1) | |
40–59 | 829 (34.4) | 12 (11.5) | |
60–79 | 836 (34.6) | 91 (87.5) | |
BMI, kg/m2 | Mean (SD) | 26.6 (5.1) | 30.2 (5.7) |
<25 | 975 (40.7) | 18 (17.3) | |
25–29.9 | 866 (36.2) | 38 (36.5) | |
≥30 | 552 (23.1) | 48 (46.2) | |
Current smoker | 637 (26.4) | 19 (18.3) | |
Past smoker | 633 (26.2) | 40 (38.5) | |
NT‑proBNP >125 pg/mla | 467 (21.6) | 60 (63.2) | |
NT‑proBNP, pg/ml, median (IQR) | 45 (38.2–119) | 181 (90.8–531) | |
The prevalence of CHF increased with age in both men and women, from 0.2% in the age group of 18 to 39 years (corresponding to about 26 000 patients in Poland at the time when the NATPOL survey was conducted) to 3.2% in the age group of 40 to 59 years (341 500 patients in Poland) and 13.2% in the age group of 60 to 79 years (832 500 patients in Poland) (Figure 1). There were significant differences between the groups (P <0.001).
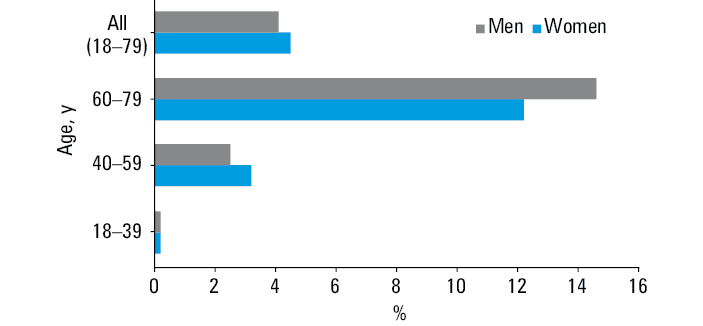
Overall, the above rates corresponded to 1 200 000 individuals with CHF in the age group of 18 to 79 years. No significant differences in the rates of CHF were found between genders (4.5% in women vs 4.1% in men; P = 0.44).
The prevalence of CHF was higher in overweight (4.4%) and obese (9.2%) individuals, than in patients with a body mass index lower than 25 kg/m2 (1.5%) (P <0.001).
NT‑proBNP levels above the diagnostic cutoff (>125 pg/ml) in the group with self‑reported CHF were found in 63.2% of patients, and the median NT‑proBNP level was 181 pg/ml (IQR, 90.8–531). In the study population, the proportion of patients with the NT‑proBNP level greater than 125 pg/ml was 21.6%, and the median NT‑proBNP level was 64.5 pg/ml (IQR, 38.2–119).
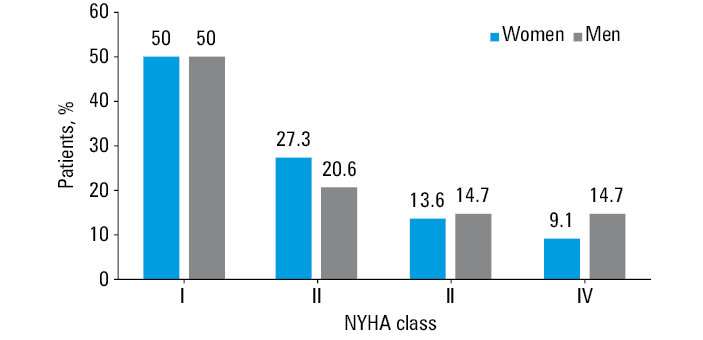
The distribution of CHF symptom severity by the NYHA class is shown in Figure 2. In the group with diagnosed HF, half of the patients reported NYHA class I symptoms, 1 in 4 patients reported limited exercise tolerance corresponding to NYHA class II, 14% of patients reported symptoms during routine daily activities (NYHA class III), and 1 in 10 patients reported resting symptoms (NYHA class IV). Leg edema was reported by 34% of the participants.
The prevalence of CHF based on the NFZ data was 3.0%. These data also showed an increase in the CHF prevalence with age, as was the case when CHF was diagnosed based on the questionnaire and medical records (Table 2).
Parameter | NFZ database | NATPOL 2011 | |
Abbreviations, see Table 1 | |||
Prevalence of CHF, % | 3.0 | 4.3 (95% CI, 3.6%–5.2%) | |
Mean age, y | 64.8 | 66.8 | |
Age group, y, % | 18–39 | 0.4 | 0.1 |
40–59 | 1.5 | 2.8 | |
60–79 | 10.5 | 13.2 | |
Among the 104 individuals who declared having CHF, 58 (55.8%) had a record of at least 1 outpatient visit or hospitalization related to the ICD‑10 I50 code in the NFZ database. The remaining 44.2% were participants who were not matched due to incomplete data merge (as described in the Methods section), individuals who did not use public health care services, and those who possibly incorrectly reported having CHD. Based on the number of concordant diagnoses in both data sources (the NATPOL 2011 study and the NFZ database), a total of 2.4% of the CHF diagnoses in the entire NATPOL 2011 study were confirmed in the NFZ records. Only 2 participants who did not declare having CHF in the NATPOL 2011 study had a record of an I50‑related service in the NFZ database.
The rates of concomitant chronic diseases in the patients with CHF compared with the general population are shown in Table 3. Among the patients with diagnosed CHF, chronic conditions were more prevalent than in the age‑matched general population. The prevalence of ischemic heart disease, previous myocardial infarction, atrial fibrillation, chronic kidney disease, and elevated NT‑proBNP levels was higher among the CHF patients (P <0.001).
Parameter | Without CHF (n = 104) | With CHF (n = 104) | P value |
Data are presented as percentages.
Abbreviations: eGFR, estimated glomerular filtration rate; others, see Table 1 | |||
Arterial hypertension | 76.9 | 70.9 | 0.41 |
Diabetes | 15.4 | 26.9 | 0.06 |
Coronary artery disease (self‑reported) | 23.1 | 57.7 | <0.001 |
Previous myocardial infarction | 7.7 | 29.8 | <0.001 |
Chronic kidney disease (self‑reported and / or eGFR<60 ml/min) | 5.8 | 12.8 | 0.02 |
Atrial fibrillation (self‑reported) | 10.6 | 36.5 | <0.001 |
Chronic obstructive pulmonary disease | 6.8 | 7.9 | 0.39 |
The analysis of guideline‑based pharmacotherapy for CHF showed that nearly 60% of individuals reporting a previous diagnosis of CHF were taking β-blockers and angiotensin‑converting enzyme inhibitors (ACEIs) or angiotensin receptor blockers, but only 1 in 3 patients was taking a loop diuretic. Triple therapy (ACEI, β-blocker, loop diuretic) was reported by 1 in 4 patients, while 6% of the patients were not taking any medications recommended for pharmacological treatment of CHF.
Discussion
In our study, the prevalence of self‑reported CHF in Poland was estimated at 4.3%, representing 1 200 000 individuals. This number may overestimate the real prevalence of diagnosed cases of CHF in Poland, as we were able to confirm the diagnosis in 55.8% of cases, which translated into 2.4% of confirmed diagnoses of CHF in Polish adults.
The prevalence of CHF increased with age. There were no significant differences in the rates of CHF in men and women. Participants who self‑reported CHF much often declared having coronary heart disease, previous myocardial infarction, and atrial fibrillation, and had higher NT‑proBNP levels.
Heart failure is a major medical and social problem. Thus, obtaining reliable data on the number of patients with this condition in Poland is necessary for an adequate health care planning. However, based on nationwide representative studies, the evaluation of CHF prevalence is much more complicated than, for example, the assessment of the prevalence of hypertension.9 The challenge is due to a complex diagnostic algorithm of CHF, which involves imaging studies. Full echocardiographic evaluation takes on average 30 to 45 minutes, and requires costly equipment and expertise of the examiner. In addition, ultrasound examination is virtually impossible at home and requires participants’ attendance at a diagnostic unit. This may be particularly difficult in the elderly, as the severity of symptoms often makes the patient unable to leave home, which may result in a significant selection bias. Also of note, echocardiography is relatively expensive and may be unfeasible in a population study for economic reasons. Our study was performed using a representative population sampling approach throughout the whole country at almost 250 locations. Thus, we decided to evaluate the number of patients with a previous diagnosis of HF based on a questionnaire and available medical records. In addition, the plasma NT‑proBNP level was measured.
Previous studies on the prevalence of chronic heart failure
For reasons specified above, studies evaluating the prevalence of HF using echocardiography were performed only in local or at most regional populations in Western Europe and the United States.10 In the Rotterdam Heart Study,11 performed in the early 1990s, a questionnaire was administered at home to 7983 participants above 50 years of age, and in those reporting symptoms of HF, the diagnosis was verified by means of echocardiography. Based on this approach, the prevalence of HF in Rotterdam was estimated at 3.9% (95% CI, 3.0%–4.75%), without significant differences with respect to gender. The only representative study in the general population undertaken in the primary care practice settings was the Portuguese EPICA (Epidemiologia da Insuficiência Cardiaca e Aprendizagem) study12 performed in the late 1990s, with a sample size similar to that of the Rotterdam study. In that study, 5434 individuals above 25 years of age were randomly selected from among patients attending primary care physicians. Symptoms and signs of HF were evaluated using the Boston questionnaire, and in the patients who scored 3 points or more, electrocardiography, imaging studies (chest X‑ray and echocardiography), and laboratory tests were performed. Overall, the prevalence of HF was 4.36% and it increased with age up to 16.1% in those above 80 years.12 The results of both these studies were similar to those obtained in the NATPOL 2011 study, which showed that the prevalence of HF in people aged 18 to 79 years was 4.3%. At the time our study was performed, the population of Poland aged 18 to 79 years was 29 975 000, yielding the estimated number of 1 200 000 patients with HF in this age group.
Previous studies in Poland
The present study collected data for the population aged 18 to 79 years, showing a much higher prevalence of HF than previously reported.1,2 Concurrently, the PolSenior project13 was undertaken using the same methodology and recruitment approach in the Polish population, with additional comprehensive geriatric assessment. This project included individuals above 65 years of age and was aimed to estimate the total number of patients with HF in Poland. The diagnosis of HF was based on previous hospitalizations due to this condition. Among individuals older than 80 years the prevalence was 12.3%, corresponding to 167 000 patients in this age group in the general Polish population. Altogether, the estimates from these 2 studies for individuals aged 18 to 79 and over 80 years give a total of 1 367 000 adult patients aware of the diagnosis of HF in Poland. This Figure is twice as high as the previous estimates.1,2
Cross‑sectional surveys, such as the NATPOL 2011 and PolSenior studies, are an attempt to evaluate the epidemiology of HF in representative population samples, and they are a valuable addition to previous outpatient care studies. In 2013, a nationwide study that included randomly selected outpatient care units and hospital wards was performed.14,15 The study recruited 1300 patients from 160 hospital wards and 2006 patients from 390 outpatient care units. It provided data on the clinical characteristics and pharmacotherapy in patients with HF in Poland, which, together with the results of the cross‑sectional NATPOL 2011 and PolSenior studies, enabled to provide a clearer picture of the disease. Until now, however, no analyses of the HF prevalence have been performed in population studies in our country. It may be expected that due to subsequent introduction of interventional treatment and aging of the society, the number of these patients will rise rapidly in Central and Eastern Europe.
Recently, Sierpinski et al16 reported the prevalence of chronic comorbidities among patients with HF in Poland based on 2 ESC registries: the ESC‑HF Pilot Survey (2009–2010) and the ESC‑HF‑LT Registry (2011–2013). In their study, the reported prevalence of arterial hypertension (66%) and coronary heart disease (59%) was similar to our estimates in the HF group. On the other hand, the prevalence of diabetes (43%), chronic kidney disease (42%), and atrial fibrillation (45%) was higher in the registry analyses. One of the possible explanations of this discrepancy may be inclusion of hospitalized patients (with acute HF) in the aforementioned paper. Another reason can be a difference in the definitions of diseases in both studies (diabetes, chronic kidney disease). We cannot, however, exclude the possibility that lower morbidity of chronic diseases in our study was in part due to overreporting of HF.
N‑terminal pro–B‑type natriuretic peptide levels in the representative population sample
An important element of the NATPOL 2011 study were NT‑proBNP level measurements, performed for the first time in a nationwide epidemiological study in adults in Poland. The role of natriuretic peptides in the diagnosis of HF has increased in the last decade. The cutoff value (decision threshold), rather than the reference range, is the most important in the diagnostic algorithm for HF. In the simplified 2012 ESC guidelines,17 the cutoff value for NT‑proBNP, serving as an indication for an imaging study, was above 125 pg/ml. The same threshold was used in the present analysis. Among patients with HF, 1 in 3 (37%) had the NT‑proBNP level below the cutoff value. It should be noted, however, that this cutoff has been recommended in the guidelines to evaluate the likelihood of HF in patients with symptoms (dyspnea or limited exercise tolerance) or other findings suggestive of HF but without a previous HF diagnosis. An NT‑proBNP level below the cutoff value indicates that HF is unlikely (with the probability >90%) in a model situation of an untreated patient with symptoms suggestive of HF. In the NATPOL 2011 study population, this process was extended in time and complex, as the participants had an earlier diagnosis of HF, were at various stages of the disease, were taking drugs, and CHF was compensated in some of them. Compensation of HF can be associated with significant reduction in natriuretic peptide levels.18 Peripheral edema was present in only 1 in 3 patients with HF, so it may be supposed that most of the analyzed patients were in an euvolemic state. In addition, half of the patients reported NYHA class I symptoms, which may also explain a relatively low proportion of patients with elevated NT‑proBNP levels.
Moreover, Dahlström19 showed low levels of natriuretic peptides in patients with preserved ejection fraction (EF), in whom diastolic dysfunction due to impaired relaxation is the predominant mechanism. For this reason, the BNP or NT‑proBNP level in this group was not markedly elevated. On the other hand, it was reported, mostly in patients with reduced EF, that natriuretic peptide levels do not normalize completely despite initiation of treatment reducing volume overload. Among individuals with reduced HF included in the PARADIGM‑HF trial,20 a decrease in NT‑proBNP levels during a therapy with enalapril was observed in only 5% of patients.20
In the NATPOL 2011 study, imaging was not performed and EF was not evaluated, and thus it was not possible to ascertain the type of HF. In addition, the NT‑proBNP level was measured only at a single occasion. Neither the recommended cutoff value nor a single measurement can serve as a measure of treatment effectiveness. Natriuretic peptide levels in a chronic condition depend on multiple factors, including baseline levels and drug treatment used.
New York Heart Association scale
A surprisingly high proportion of CHF patients in our study were in NYHA class I. While we were not able to precisely explain this discrepancy, a few possible reasons could be named. First, there are some literature data showing that patients with chronic diseases underestimate their symptoms. For example, in the COMET (Carvedilol or Metoprolol European Trial) study21 some patients did not rate their major symptoms as they should have according to the NYHA scale.
Another possibility is poor reliability of the questionnaire‑based diagnosis of CHF. Patients answered the questions themselves. In some studies, they assigned their symptoms to a lower NYHA class as compared with clinical assessment. A study by Goode et al22 showed that classification of the severity of symptoms according to the NYHA scale differed between physicians and patients by at least 1 class in 50% of cases.
It is difficult to discuss the prevalence of dyspnea in the study cohort in relation to other studies. The NYHA scale is dedicated to patients with CHF, and the vast majority of studies assessing the severity of symptoms are carried out in patients with confirmed disease.
Drug treatment
The use of ACEIs or sartans and β-blockers has been recommended in the ESC guidelines on the management of HF. Recently introduced treatments, for example, with sodium‑glucose cotransporter 2 inhibitors or neprilysin inhibitors, were not in use at the time of the data collection. The inherent components of the drug therapy are loop diuretics, which do not affect survival but reduce symptoms and improve patient comfort. In the NATPOL 2011 study, β-blockers and ACEIs were used by 60% of the participants with HF, while loop diuretics, by 1 in 3 patients. Triple therapy was used in only 1 in 4 patients. These data indicate that drug treatment of HF is still inadequate; however, this could also be a result of CHF overreporting by the study patients. On the other hand, our results on the use of ACEIs and β-blockers were similar to those reported in another study in CHF patients,23 in which β-blockers were used by less than 70% of participants.
Medication compliance could have affected our estimates, as we took into consideration the drugs really taken by the patients, not just the ones that were prescribed. It is possible that some of our patients reported not taking drugs if they were prescribed by a doctor but not really used. A number of studies suggest that compliance in HF patients can be lower than optimal.24 More recent data indicate an improvement in this regard in Poland, but the issue of treatment adherence requires continuous efforts to educate both the health care personnel and the patients.13,14
Study limitations
A major limitation of our analysis of the data from the NATPOL 2011 study is the fact that the prevalence of HF was evaluated based on self‑reported history of HF and available medical records but without verification by imaging. The effectiveness of such an approach was assessed in the 2005 ARIC (Atherosclerosis Risk in Communities) study.25 It evaluated the sensitivity and specificity of the questionnaire‑based diagnosis of HF. In all respondents who gave an affirmative answer to the question regarding previous diagnosis of HF, the diagnosis was verified with a treating physician. The sensitivity was between 28% and 38% and the specificity was 96% to 97%.25 These results indicate that the prevalence assessed based on a questionnaire only may be largely underestimated. On the other hand, the estimated prevalence of HF in the NATPOL 2011 study was higher than the previous estimates and it seems unlikely that it could still be significantly underestimated. In addition, only 6% of patients with the diagnosis of HF in the NATPOL 2011 study did not take any of the major drugs used in the treatment of HF, although these medications may obviously be taken also for other indications. Clearly, the available data on the epidemiology of HF are still inadequate. Perhaps we would have obtained more objective and detailed data had the authors of the NATPOL 2011 study specified the year of HF diagnosis or the duration of the disease in the questionnaire. Such an approach should be considered when planning further studies.
Another limitation of the study is the number of included individuals. This analysis was based on a relatively small group of 104 patients with CHF from a moderate sample of 2413 people representing adult Poles (ca 30 million people). On the other hand, our sample was carefully designed so that it was representative of the national population, and the sampling error was defined.
The response rate of 66% was lower than what we had achieved in our previous national study,26 even though efforts were made to make this number as high as possible. In a similar study performed in 2002,26 the response rate reached 79%. The problem of a low response rate in survey studies has been recently increasing in Poland (and the whole Europe). Surely, it was a potential source of bias, possibly towards more apparently healthy people in the sample. Nevertheless, we were at least able to control the structure of the final sample in terms of age, sex, and place of residence, partly decreasing this bias. Our sample still seems the least biased source of national‑level data (as compared with health insurance registries and local samples).
Moreover, only 2258 participants had the NT‑proBNP levels measured, including 97 with self‑reported CHF. This group was relatively small; however, to our best knowledge, there is no other nationally representative study in Central Europe assessing the distribution of natriuretic peptides in the general population.
A major strength of the present analysis is the use of 2 alternative approaches in the same study sample: a questionnaire and data retrieval from the healthcare payer database. While the first approach may be biased due to overreporting of CHF by patients resulting in overestimated prevalence, verification of the diagnosis with another source (the NFZ database) made the estimation more reliable. The results obtained with these 2 approaches yield a reasonable range of the CHF prevalence in Poland between 2.4% and 4.3%.
Conclusions
The results of our study indicated that the proportion of inhabitants of Poland aged 18 to 79 years with HF is somewhere between 2.4% and 4.3%. This corresponds to a range of 720 000 to 1 200 000 diagnosed CHF patients in Poland. A more precise assessment of the prevalence of HF would require a representative study combining a clinical evaluation, NT‑proBNP level measurement, and imaging studies.
- Rywik TM, Kolodziej P, Targonski R, et al. Characteristics of the heart failure population in Poland: ZOPAN, a multicentre national programme. Kardiol Pol. 2011; 69: 24‑31.
- Rywik TM, Zielinski T, Piotrowski W, et al. Heart failure patients from hospital settings in Poland: population characteristics and treatment patterns, a multicenter retrospective study. Cardiol J. 2008; 15: 169‑180.
- Ponikowski P, Voors AA, Anker SD, et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur J Heart Fail. 2016; 18: 891‑975. | Crossref
- Nessler J, Straburzyńska‑Migaj E, Windak A, et al. Expert consensus on the usefulness of natriuretic peptides in heart failure. Kardiol Pol. 2018; 76: 215‑224. | Crossref
- Zdrojewski T, Rutkowski M, Bandosz P, et al. Prevalence and control of cardiovascular risk factors in Poland. Assumptions and objectives of the NATPOL 2011 Survey. Kardiol Pol. 2013; 71: 381‑392. | Crossref
ARTICLE INFORMATION