Association of antineutrophil cytoplasmic antibody (ANCA) specificity with demographic and clinical characteristics of patients with ANCA‑associated vasculitides
Key words: ANCA, ANCA-associated vasculitis, antineutrophil cytoplasmic antibodies, myeloperoxidase, proteinase-3



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Association of antineutrophil cytoplasmic antibody (ANCA) specificity with demographic and clinical characteristics of patients with ANCA‑associated vasculitides
Introduction: Antineutrophil cytoplasmic antibody (ANCA)–associated vasculitis (AAV) is characterized by the presence of proteinase‑3 (PR3) or myeloperoxidase (MPO) ANCA. In over 90% of cases, PR3‑ANCA is associated with granulomatosis with polyangiitis (GPA). However, it is also rarely found in microscopic polyangiitis (MPA) and eosinophilic granulomatosis with polyangiitis (EGPA). On the other hand, MPO‑ANCA being characteristic of MPA (>90% of cases), is also found in about 40% of EGPA and 5% of GPA patients. On the ground of this overlap, clinical importance of ANCA specificity identification has been questioned.
Objectives: In this study, we analyzed the clinical and demographic characteristics of AAV subgroups identified by ANCA serotype.
Patients and methods: We conducted a multicenter study of AAV patients (417 GPA, 106 MPA, 102 EGPA; diagnosed between 1990 and 2016), included in the POLVAS registry. The data were systematically collected according to a standardized protocol.
Results: In the ANCA‑positive group (anti‑MPO, anti‑PR3) a male‑to‑female ratio was 1:1, whereas in the ANCA‑negative group it was 1:2, regardless of AAV diagnosis. Anti‑MPO antibodies were present in significantly older patients. Patients with MPO+GPA and MPO+EGPA were older than those with corresponding ANCA‑negative GPA and EGPA as well as PR3+AAV. Moreover, ANCA‑negative AAV was characterized by a low risk of end‑stage kidney disease and death.
Conclusions: The presence and specificity of ANCA in AAV patients are related to sex and age, determine their organ involvement and influence mortality as previously shown. Patients with MPO‑ANCA–positive AAV constitute a clinically homogeneous group, whereas PR3‑ANCA–positive patients are much more clinically heterogeneous. ANCA‑negative AAV patients are characterized by better prognosis. Thus, ANCA identification is an indispensable element and should not be omitted in establishing AAV diagnosis.
What's new?
Antineutrophil cytoplasmic antibodies (ANCA) are a hallmark of ANCA‑associated vasculitides (AAV), but their specificity does not correspond entirely to a given phenotype. Therefore, the clinical role of ANCA detection has been questioned, as opposed to a careful analysis of a clinical phenotype. Our results indicate that ANCA presence and specificity are associated with demographic (mainly age and sex) and—as previously shown—clinical characteristics related to the disease course and outcome. Particularly, the presence and specificity of ANCA in AAV patients heavily influenced organ involvement with a strong association of myeloperoxidase positivity with kidney involvement and the risk of death. Our data presented here support and strengthen the importance of ANCA identification as an indispensable element in establishing proper AAV diagnosis.
Introduction
Antineutrophil cytoplasmic antibody (ANCA)–associated vasculitides (AAV) are a group of systemic diseases involving small to medium sized vessels and the presence of 2 main classes of ANCA, namely, anti–proteinase‑3 (PR3) and anti‑myeloperoxidase (MPO) antibodies. The nomenclature for vasculitides was proposed in 2012,1 but the uniform classification criteria are yet to be developed.
In most cases (>90%), PR3‑ANCA are associated with granulomatosis with polyangiitis (GPA; formerly Wegener granulomatosis). However, they can also be found in about 10% of patients with microscopic polyangiitis (MPA) and in 5% of those with eosinophilic granulomatosis with polyangiitis (EGPA; formerly Churg‑Strauss syndrome). On the other hand, MPO‑ANCA can be detected in over 90% of individuals with MPA, about 40% of those with EGPA, and in only 5% of those with GPA. In general, GPA is associated with higher rates of relapse and more heterogeneous clinical manifestations, while a more uniform clinical presentation and higher mortality rates are typical of MPA.2,3 EGPA differs significantly from both GPA and MPA, with ANCA found only in about 40% of patients. The presence of ANCA (mainly MPO‑ANCA) determines the clinical picture of this AAV phenotype.4,5
Genome‑wide association studies showed a significant association between some genetic variants and the presence of PR3- and MPO‑ANCA. The associations were stronger than those with serological and clinical picture of AAV.6,7 This finding led to the concept of ANCA specificity as a critical prognostic marker in patients with AAV, including organ damage, relapse rate, and mortality.8 However, clinical data indicate that both forms of AAV may have heterogeneous, and sometimes atypical, symptoms,9 frequently with overlapping ANCA specificity, as exemplified by a distinct group of patients with clinically typical GPA and the presence of MPO‑ANCA.10 Thus, considering that a precise clinical classification of AAV based on pathogenesis is still lacking, ANCA specificity or genetic characteristics alone are insufficient to classify patients with AAV. As a consequence, attempts have been made to apply advanced statistical methods to better identify the subphenotypes of AAV.2,11 In this retrospective study, we attempted to look for differences in the clinical and demographic characteristics of AAV subgroups identified by ANCA serotype, and more importantly, to indirectly assess how it affects outcomes in various types of AAV.
Patients and methods
We conducted a multicenter retrospective study of all adult patients diagnosed with AAV by participating centers between 1990 and 2016 (417 GPA, 106 MPA, 102 EGPA). In this group, results of MPO / PR3 tests were available for 536 patients (127 MPO‑positive, 334 PR3‑positive, and 75 ANCA‑negative). Their clinical and laboratory data were collected in the POLVAS registry, between March 2016 and January 2017, by 9 referral centers (14 clinical wards) from 7 voivodships with 22.3 million inhabitants, encompassing 58.2% of the Polish population. Specialties of the centers included rheumatology (10), nephrology (2), metabolic diseases (1), and clinical immunology (1).12 We only included individuals who met the American College of Rheumatology classification criteria for Wegener granulomatosis (presently GPA) or Churg‑Strauss syndrome (presently EGPA), as well as criteria according to the nomenclature of GPA, MPA, and EGPA proposed by the 2012 Chapel Hill Consensus Conference (CHCC 2012),1 regardless of their disease activity at the entry. Specific organ involvement, disease relapse, and disease remission were defined according to the Birmingham Vasculitis Activity Score version 3.13 However, as the data were collected retrospectively, the exact scores for individual patients were not available. We excluded patients (even with a documented diagnosis of AAV) who were lost to follow‑up at the time of the data collection (patients outside of the control of an outpatient clinic or a hospital ward for more than 12 months before the data collection), patients younger than 18 years, and pregnant women.
The data were collected systematically according to a common protocol and included demographic, clinical, laboratory, radiographic, and pathological characteristics as well as treatment details. Hemodialysis was considered permanent if the procedure was still performed at the last follow‑up or temporary if the procedure was stopped at any time due to kidney function recovery and not reinstituted at the time of the last follow‑up. To detect ANCA positivity, an enzyme‑linked immunosorbent assay was used (PR3‑ANCA or MPO‑ANCA) and, if necessary, indirect immunofluorescence. These test results were obtained from medical records of AAV patients.
The study protocol was approved by the Bioethics Committee of the Jagiellonian University (No. 122.6120.25.2016). All patients provided written informed consent to participate in the study.
Statistical analysis
Categorical data were summarized as percentages; significant differences or associations were analyzed using the χ2 test. If the χ2 test was performed in 3 × 2 Table, the pairwise comparison was done for post hoc analysis. Continuous variables are presented as median and interquartile range, the data distribution was not normal, as determined by the Kolmogorov‑Smirnov test. Associations between quantitative data were assessed with the nonparametric Kruskal‑Wallis test followed by a post hoc analysis with the Mann‑Whitney test. A P value below 0.05 was considered significant. The Bonferroni correction for multiple testing was used to control the false discovery rate. Statistical analysis was performed using Statistica 13 software (TIBCO Software, Palo Alto, California, United States).
Results
We retrospectively analyzed a total of 625 patients with AAV included in the POLVAS registry. There were 417 patients (66.7%) with GPA, 106 patients (17.0%) with MPA, and 102 patients (16.3%) with EGPA; MPO/PR3 tests were available for 536 patients (127 MPO‑positive, 334 PR3‑positive, and 75 ANCA‑negative).
Demographic characteristics of patients depending on the clinical phenotype of vasculitis
The associations between ANCA specificity and demographic characteristics of patients with MPA, GPA, and EGPA are presented in Table 1. The groups of AAV identified by the presence and / or specificity of ANCA differed in the age at diagnosis and the male‑to‑female ratio.
Parameter | AAV phenotype | P value | |||
MPA | GPA | EGPA | |||
Data are presented as number (percentage) or median (interquartile range).
a Significant difference for MPA vs GPA
b Significant difference for MPA vs EGPA
c Significant difference after Bonfferoni correction for multiple testing
Abbreviations: AAV, ANCA‑associated vasculitides; ANCA, antineutrophil cytoplasmic antibodies; EGPA, eosinophilic granulomatosis with polyangiitis; GPA, granulomatosis with polyangiitis; MPA, microscopic polyangiitis; MPO, myeloperoxidase; NA, not applicable; PR3, proteinase‑3 | |||||
MPO‑ANCA–positive | |||||
Patients, n | 86 | 18 | 23 | – | |
Age, y | 63.5 (53.0–71.5) | 58.1 (35.7–64.0) | 56.9 (49.1–59.9) | 0.26 | |
Sex, male / female, n | 43/43 | 8/10 | 11/12 | 0.91 | |
Age at diagnosis ≤65 y, n | 49 (57.0) | 12 (66.7) | 17 (73.9) | 0.29 | |
Age at diagnosis >65 y, n | 37 (43.0) | 6 (33.3) | 6 (26.1) | ||
PR3‑ANCA–positive | |||||
Patients, n | 12 | 316 | 6 | – | |
Age, y | 63.4 (58.7–68.9) | 51.4 (39.1–59.8) | 53.0 (49.1–59.9) | 0.02a | |
Sex, male / female, n | 5/7 | 169/147 | 1/5 | 0.15 | |
Age at diagnosis ≤65 y, n | 7 (58.3) | 280 (88.6) | 6 (100) | 0.008a,c | |
Age at diagnosis >65 y, n | 5 (41.7) | 36 (11.4) | 0 | ||
ANCA‑negative | |||||
Patients, n | 2 | 26 | 47 | – | |
Age, y, | 63.4 (NA) | 43.9 (30.4–55.8) | 40.1 (30.7–51.4) | 0.46 | |
Sex, male / female, n | 2/0 | 8/19 | 15/32 | 0.42 | |
Age at diagnosis ≤65 y, n | 1 (50.0) | 25 (96.2) | 46 (97.9) | 0.003a,b,c | |
Age at diagnosis >65 y, n | 1 (50.0) | 1 (3.8) | 1 (2.1) | ||
Antineutrophil cytoplasmic antibodies and age at diagnosis
Patients with MPO‑ANCA–positive GPA and EGPA phenotypes were older at the time of diagnosis than the remaining patients (Table 1), with a substantial percentage of patients diagnosed after the age of 65. The presence of MPO‑ANCA is typical of MPA (the most homogenous AAV phenotype), and these patients had a significantly higher mean age at diagnosis than those with GPA or EGPA (P <0.01 and P <0.001, respectively). Moreover, in the GPA and EGPA groups, MPO‑ANCA–positive patients were older than ANCA‑negative for EGPA patients (P <0.001) and PR3‑ANCA–positive patients for GPA (P <0.01) (Table 1).
The presence of PR3‑ANCA is associated mainly with GPA phenotype. Patients with PR3‑ANCA–positive GPA were younger at the time of diagnosis than those with MPO‑ANCA–positive GPA. On the other hand, patients with PR3‑ANCA–positive MPA were slightly older at diagnosis than their MPO‑ANCA–positive counterparts.
Antineutrophil cytoplasmic antibodies and male‑to‑female ratio
The male‑to‑female ratio in the patients with MPA (54 men, 52 women) and GPA (210 men, 207 women) was about 1:1, which is in line with other European countries.3,14-16 The ratio was similar in MPO‑ANCA–positive group (62 men, 65 women), PR3‑ANCA–positive group (175 men, 159 women), but it was different and amounted to 1:2 in ANCA–negative group (25 men, 51 women). On the other hand, EGPA was diagnosed twice more often in women (n = 64) than in men (n = 32). However, this was not observed in the subgroup of patients with MPO‑ANCA–positive EGPA, where the male‑to‑female ratio was 1:1, as in other MPO‑ANCA–positive phenotypes (Table 1). Interestingly, for the ANCA‑negative GPA phenotype the male‑to‑female ratio was also 1:2. The data on the number of men and women according to the phenotype are presented in Table 1.
Clinical characteristics of patients depending on the phenotype of vasculitis
The clinical characteristics and laboratory parameters of patients with AAV depending on ANCA specificity are shown in Tables 2 and 3.
Parameter | MPO‑ANCA–positive | P value | ||
MPA (n = 86) | GPA (n = 18) | EGPA (n = 23) | ||
Data are presented as number (percentage) or median (interquartile range).
a Significant difference for MPA vs EGPA
b Significant difference for MPA vs GPA
c Significant difference for GPA vs EGPA
d Significant difference after Bonfferoni correction for multiple testing
e Neurological manifestation was referred to the peripheral nervous system involvement
f Creatinine max = maximum creatinine concentration ever
Conversion factors to SI units: to convert creatinine to μmol/l, multiply by 88.4.
Abbreviations: CNS, central nervous system; CRP, C‑reactive protein; others, see Table 1 | ||||
Organ involvement | ||||
General | 65 (75.6) | 15 (83.3) | 19 (82.6) | 0.17 |
Skin | 19 (22.1) | 7 (38.9) | 12 (52.2) | 0.01a,d |
Eye | 3 (3.5) | 4 (22.2) | 5 (21.7) | 0.004a,b,d |
Ear, nose, throat | 14 (16.3) | 13 (72.2) | 18 (78.3) | <0.001a,b,d |
Respiratory | 52 (60.5) | 14 (77.8) | 22 (95.6) | 0.004a,d |
Cardiac | 10 (11.6) | 4 (22.2) | 5 (21.7) | 0.31 |
Gastrointestinal | 10 (11.6) | 2 (11.1) | 5 (21.7) | 0.43 |
Renal | 82 (95.3) | 11 (61.1) | 10 (43.5) | <0.001a,b,d |
Urinary | 3 (3.5) | 0 | 0 | – |
CNS | 2 (2.3) | 1 (5.5) | 2 (8.7) | 0.35 |
Neurologicale | 18 (20.9) | 2 (11.1) | 11 (47.8) | 0.01a,c,d |
Clinical characteristics | ||||
Creatinine maxf, mg/dl | 3.43 (2.0–6.0) | 1.2 (1.0–1.5) | 1.0 (0.8–1.1) | <0.001a,b,d |
CRP at baseline, mg/l | 33.4 (13.4–97.1) | 36 (10.5–91) | 53 (31.5–76) | 0.18 |
No. of organs involved | 2 (2–3) | 3 (2–4) | 4 (3–5) | <0.001a,d |
Relapse | 24 (27.9) | 7 (38.9) | 10 (43.5) | 0.3 |
Dialysis | 30 (34.9) | 4 (22.2) | 0 | 0.3 |
Temporary dialysis | 10 (11.6) | 1 (5.5) | 0 | 0.45 |
Parameter | PR3‑ANCA–positive | P value | ||
MPA (n =12) | GPA (n = 316) | EGPA (n = 6) | ||
Data are presented as number (percentage) or median (interquartile range).
a Significant difference for MPA vs EGPA
b Significant difference for MPA vs GPA
c Significant difference for GPA vs EGPA
d Significant difference after Bonfferoni correction for multiple testing
e Neurological manifestation was referred to the peripheral nervous system involvement
f Creatinine max = maximum creatinine concentration ever
Conversion factors to SI units: see Table 1
| ||||
Organ involvement | ||||
General | 12 (100.0) | 278 (88.0) | 5 (83.3) | 0.8 |
Skin | 2 (16.7) | 109 (34.5) | 2 (33.3) | 0.44 |
Eye | 0 | 86 (27.2) | 0 | – |
Ear, nose, throat | 2 (16.7) | 239 (75.6) | 6 (100) | <0.001a,b,d |
Respiratory | 3 (25) | 247 (78.1) | 6 (100) | <0.001a,b,d |
Cardiac | 1 (8.3) | 38 (12.0) | 3 (50) | 0.02a |
Gastrointestinal | 2 (16.7) | 38 (12.0) | 1 (16.7) | 0.84 |
Renal | 11 (91.7) | 212 (67.1) | 1 (16.7) | 0.006a,c,d |
Urinary | 0 | 7 (2.2) | 0 | – |
CNS | 0 | 36 (11.4) | 0 | – |
Neurologicale | 0 | 59 (18.7) | 3 (50) | 0.054 |
Clinical characteristics | ||||
Creatinine maxf, mg/dl | 4.5 (2.9–6.0) | 1.2 (1.0–3.2) | 1.0 (0.93–1.0) | 0.004a,b,d |
CRP at baseline, mg/l | 41.5 (9.5–70.5) | 47 (14.0–117.0) | 13 (4.8–45.3) | 0.7 |
No. of organs involved | 1.5 (1–2) | 3 (2–4) | 4 (3.25–4) | 0.03a,b |
Relapse | 2 (16.7) | 197 (62.3) | 4 (66.6) | 0.006a,b,d |
Permanent dialysis | 5 (41.7) | 42 (13.3) | 0 | 0.01b,d |
Temporary dialysis | 0 | 27 (8.5) | 0 | – |
As expected, in the MPA group, the characteristics of patients with MPO‑ANCA positivity were similar to those noted for the entire group. A small subgroup of patients with PR3‑ANCA–positive MPA showed a lower mean number of organs involved as compared with patients with classic MPO‑ANCA–positive MPA. Moreover, respiratory involvement was less common in patients with PR3‑ANCA–positive MPA. No other significant differences were noted.
In the GPA group, the clinical manifestations were similar regardless of ANCA specificity.
In the EGPA group, the clinical characteristics were strongly associated with the ANCA status (Table 4). The patients with MPO‑ANCA–positive EGPA less often showed cardiac involvement than those with MPO‑ANCA–negative EGPA, but they had a higher frequency of renal involvement. This is in line with previous studies.4,5
Parameter | EGPA | P value | ||
MPO‑ANCA–positive (n = 23) | PR3‑ANCA–positive (n = 6) | ANCA–negative (n = 47) | ||
Data are presented as number (percentage) or median (interquartile range).
a Significant differences for MPO‑ANCA–positive vs ANCA‑negative
b Significant difference after Bonfferoni correction for multiple testing
c Neurological manifestation was referred to the peripheral nervous system involvement
d Creatinine max = maximum creatinine concentration ever
e Post hoc not significant
Conversion factors to SI units: see Table 1
| ||||
Organ involvement | ||||
General | 19 (82.6) | 5 (83.3) | 46 (97.9) | 0.6 |
Skin | 12 (52.2) | 2 (33.3) | 25 (53.2) | 0.58 |
Eye | 5 (21.7) | 0 | 1 (2.1) | 0.01a,b |
Ear, nose, throat | 18 (78.3) | 6 (100) | 38 (80.8) | 0.84 |
Respiratory | 22 (95.6) | 6 (100) | 47 (100) | 0.34 |
Cardiac | 5 (21.7) | 3 (50) | 25 (53.2) | 0.04a |
Gastrointestinal | 5 (21.7) | 1 (16.7) | 15 (31.9) | 0.55 |
Renal | 10 (43.5) | 1 (16.7) | 10 (21.3) | 0.12 |
Urinary | 0 | 0 | 0 | – |
CNS | 2 (8.7) | 0 | 4 (8.5) | 0.98 |
Neurologicalc | 11 (47.8) | 3 (50) | 24 (51.1) | 0.97 |
Clinical characteristics | ||||
Creatinine maxd, mg/dl | 1.0 (0.8–1.1) | 1.0 (0.93–1.0) | 0.81 (0.7–0.99) | 0.019e |
CRP at baseline, mg/l | 53 (31.5–76) | 13 (4.8–45.3) | 30.5 (12–57) | 0.045e |
No. of organs involved | 4 (3–5) | 4 (3.25–4) | 4 (3–5) | 0.85 |
Relapse | 10 (43.5) | 4 (66.6) | 35 (74.5) | 0.04a |
Permanent dialysis | 0 | 0 | 0 | – |
Temporary dialysis | 0 | 0 | 0 | – |
The clinical characteristics and organ involvement in ANCA‑negative AAV are shown in Supplementary material, Table S1. The patients with ANCA‑negative GPA showed a lower frequency of renal involvement than those with ANCA‑positive GPA (11.5% vs 63.7%; P <0.05) (Supplementary material, Table S1). Moreover, in the patients with ANCA‑negative AAV, renal involvement did not progress to end‑stage renal disease or need for temporary renal replacement therapy.
Discussion
Various attempts have been made to identify parameters that would facilitate the classification of AAV into specific clinical subphenotypes. These parameters include a clinical profile,2,11,17 ANCA serotype,10,16genetic background, and any combination thereof.2,11 However, none of these parameters alone was sufficient to effectively classify AAV into clinical subphenotypes.
While genome‑wide association studies6,7 confirmed the strongest genetic association of AAV with ANCA antigen specificity and not with any specific set of clinical symptoms, the utility of ANCA testing for clinical purposes has been questioned.17 Therefore, we investigated the associations of ANCA specificity with the demographic and clinical characteristics of patients with AAVs based on retrospective data from the POLVAS registry.
The analysis of the POLVAS registry data based on ANCA specificity yielded several interesting findings. First, MPO‑ANCA–positive patients seem to be a rather homogenous group in terms of clinical characteristics. The specific features include older age at disease onset as compared with PR3‑ANCA–positive patients, a male‑to‑female ratio of 1:1 (Figure 1), and a high prevalence of renal involvement. In contrast, the PR3‑ANCA–positive group was clinically much more heterogeneous.
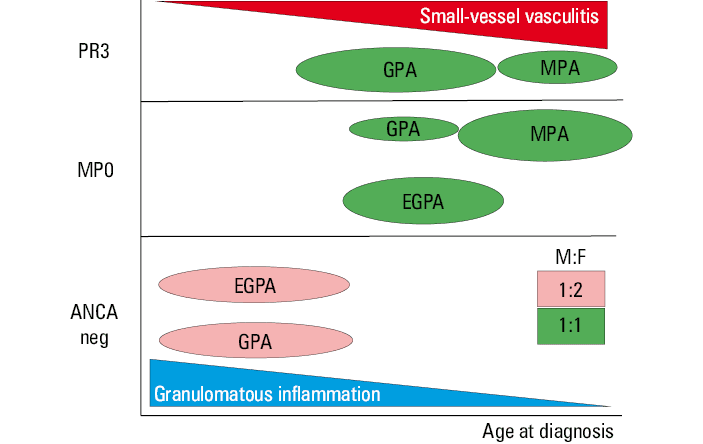
Abbreviations: M:F, male‑to‑female ratio; others, see Table 1
In patients with PR3‑ANCA–positive AAV, clinical disease subphenotypes with different treatment response and outcomes were previously reported.11 In the POLVAS registry, age at diagnosis was one of the critical variables in the subphenotyping of patients with GPA, showing that ANCA specificity is not the only determinant of AAV course.
Interestingly, an analysis of 3 subphenotypes11 of PR3‑ANCA–positive AAV also revealed differences in male‑to‑female ratio, with a ratio of 1:2 in nonsevere AAV with ear, nose, and throat and lung involvement, a ratio of 1:1 in severe PR3‑ANCA–positive AAV, and a ratio of 2:1 in renal nonsevere PR3‑ANCA–positive AAV with multiorgan involvement (renal involvement in 40% of cases, but normal estimated glomerular filtration rate). This indicates that the male‑to‑female ratio may differ depending not only on ANCA specificity but also on AAV subphenotype.
The extent to which the presence and specificity of ANCA affects the clinical phenotype of the disease is best exemplified by EGPA, a phenotypically heterogeneous disease that is included in AAV group even if ANCAs are detected in only 30% to 40% of patients with EGPA.18 In our EGPA group, MPO‑ANCA–positive patients were significantly older (by over 15 years) than their ANCA‑negative counterparts, and the male‑to‑female ratio was 1:1 vs 1:2 in ANCA‑negative patients. This is in line with a Japanese study,19 but in contrast with results reported by a French registry.4 As noted by other investigators,4,5 MPO‑ANCA–positive patients often show a higher frequency of renal involvement, but cardiac involvement is less common. These features are similar to those noted for MPA phenotype. Interestingly, in a distinct subgroup of patients with PR3‑ANCA–positive EGPA, the clinical picture was so close to that of GPA that they were even considered to have a specific form of GPA.20 In our cohort, there were only 6 such patients with PR3‑ANCA–positive EGPA, which is insufficient to make a reliable comparison. On the other hand, it was recently proposed that ANCA‑negative EGPA with no definite features or surrogates of vasculitis constitutes a new entity: hypereosinophilic asthma with systemic manifestations.20 Differences in demographic and clinical characteristics depending on the presence and type of ANCA in all AAV patients also have a prognostic value. These prognosticators are older age (>65 years) and renal involvement, and they are included in the modified Five‑Factor Score as parameters predictive of prognosis in systemic necrotizing vasculitides.15 This refers to MPO‑ANCA–positive EGPA but even more so to other MPO‑ANCA–positive vasculitides, mainly MPA.2,12
Another important aspect of ANCA testing comes from a recently published case report of an atypical AAV resembling peripheral arterial ischemic disease.21 Here, the detection of ANCA was a key point for diagnosis.
We showed some distinct features of a broader group of ANCA‑negative AAV. These patients were significantly younger, their male‑to‑female ratio was close to 1:2, and their prognosis was better than that of patients with ANCA‑positive AAV. Analyzing such a group of ANCA‑negative AAV, Miloslavsky et al10 showed the male‑to‑female ratio similar to that in the POLVAS registry but with no difference in age. Their analysis, however, was based on the data from clinical trials (WGET [Wegener’s Granulomatosis Etanercept Trial] and RAVE [Rituximab for ANCA‑Associated Vasculitis]), thus limited to patients fulfilling the trial entry criteria, contrary to our POLVAS registry including all patients diagnosed with AAV.
These ANCA‑AAV patients belonged to EGPA (n = 47) or GPA (n = 26) group with limited involvement (mainly of the upper respiratory tract), as previously observed by us and other investigators.12,15 Of note, in the Five‑Factor Score, upper respiratory tract involvement is the only factor associated with better prognosis in AAV.15
Analysis of ANCA‑negative AAV group suggests also that granulomatous component of AAV22 seems to be ANCA‑independent and more pronounced in younger individuals, whereas the vasculitic component shows ANCA dependency and increases with age (Figure 1).
Until the pathogenesis of the various forms of AAV is fully elucidated, their classification into different subphenotypes as well as identification of the most relevant markers will remain a challenge. For now, the most appropriate approach seems to be the determination of ANCA specificity with genetic background together with advanced statistical analysis of demographic, laboratory, and clinical characteristics.2,11 This complex workup may also change our approach to treatment. It has been already shown in a post hoc analysis of the RAVE trial that ANCA‑PR3–positive patients treated with rituximab had a 2‑fold higher odds of achieving remission than those treated with cyclophosphamide.8 This was also true for patients with relapsing disease. On the other hand, efficacy of rituximab was not different from cyclophosphamide among MPO‑ANCA–positive patients. The major limitation of the study is the limited number of patients, which is a common problem in studies on rare disorders. The POLVAS registry includes 9 Polish centers involved in the diagnosis and treatment of vasculitides. This enabled structured data collection from a cohort of several hundred patients with AAV. To include more patients, it would be useful to design tools allowing for data collection from different European registries of AAV, such as dedicated software, rules, and legal regulations (as in the recently founded FAIRVASC project; https://fairvasc.eu). This could enable the analysis of data on rare diseases across different national registries in Europe.
In summary, our results indicate that the presence and specificity of ANCA strongly affect the classification of AAV. An association of ANCA presence and specificity with the demographic and clinical characteristics related to the disease course and outcome in patients with AAV was also revealed.
- Jennette JC. Overview of the 2012 Revised International Chapel Hill Consensus Conference Nomenclature of Vasculitides. Clin Exp Nephrol. 2013; 17: 603‑606. | Crossref
- Mahr A, Katsahian S, Varet H, et al. Revisiting the classification of clinical phenotypes of anti‑neutrophil cytoplasmic antibody‑associated vasculitis: a cluster analysis. Ann Rheum Dis. 2013; 72: 1003‑1010. | Crossref
- Solans‑Laqué R, Fraile G, Rodriguez‑Carballeira M, et al. Clinical characteristics and outcome of Spanish patients with ANCA‑associated vasculitides: impact of the vasculitis type, ANCA specificity, and treatment on mortality and morbidity. Medicine (Baltimore). 2017; 96: e6083. | Crossref
- Comarmond C, Pagnoux C, Khellaf M, et al. Eosinophilic granulomatosis with polyangiitis (Churg‑Strauss): clinical characteristics and long‑term followup of the 383 patients enrolled in the French Vasculitis Study Group cohort. Arthritis Rheum. 2013; 65: 270‑281. | Crossref
- Sokolowska BM, Szczeklik WK, Wludarczyk AA, et al. ANCA‑positive and ANCA‑negative phenotypes of eosinophilic granulomatosis with polyangiitis (EGPA): outcome and long‑term follow‑up of 50 patients from a single Polish center. Clin Exp Rheumatol. 2014; 32: S41‑S47.
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION