An 88‑year‑old man was referred to the hospital by a general practitioner because of severe anemia in laboratory workup. The patient reported weakness and loss of appetite during the preceding month but denied any weight loss. He admitted he had not been regularly taking the prescribed medications for multiple cardiovascular diseases, type 2 diabetes mellitus, benign prostate hyperplasia, and hypothyroidism. Of note, he had a history of laparotomy due to gastrointestinal tract obstruction caused by adhesions (2013).
On admission, physical examination revealed pale skin with some bruising, arrhythmia, single crackles at the base of the lungs, and slight swelling of the lower limbs. There was no abdominal pain on palpation, and peristalsis was maintained. Laboratory workup confirmed microcytic anemia (hemoglobin, 6.6 g/dl; reference range, 11.2–15.8 g/dl) associated with acenocoumarol overdose (international normalized ratio [INR], 5.55; reference range, 0.8–1.2), resulting in a subsequent packed red blood cells transfusion (2 units) and INR monitoring. The serum creatinine level was mildly elevated (94 μmol/l; reference range, 37–96 μmol/l).
Shortly after the transfusion, the patient’s blood parameters and well‑being improved. However, on day 4 of hospitalization, his general condition deteriorated and he developed symptoms of lower gastrointestinal obstruction—a short episode of diarrhea, followed by modest abdominal pain with constipation, abdominal flatulence, and a progressive increase in inflammatory parameters despite empirical antibiotic therapy. Subsequent abdominal X‑rays performed in lying and sitting positions showed a dilated large bowel, indicating obstruction (Figure 1A). After repeated consultations with a surgeon and following colonoscopy, a decision was finally made to insert a rectal tube. However, the cause of obstruction still remained undiagnosed. A progressive increase in serum levels of C‑reactive protein and creatinine was observed, reaching 196 mg/l (reference range, 0–5 mg/l) and 467.4 μmol/l, respectively, on day 8, without improvement of the gastrointestinal obstruction. The patient reported frequent passing of small amounts of urine but denied any other lower urinary tract symptoms.
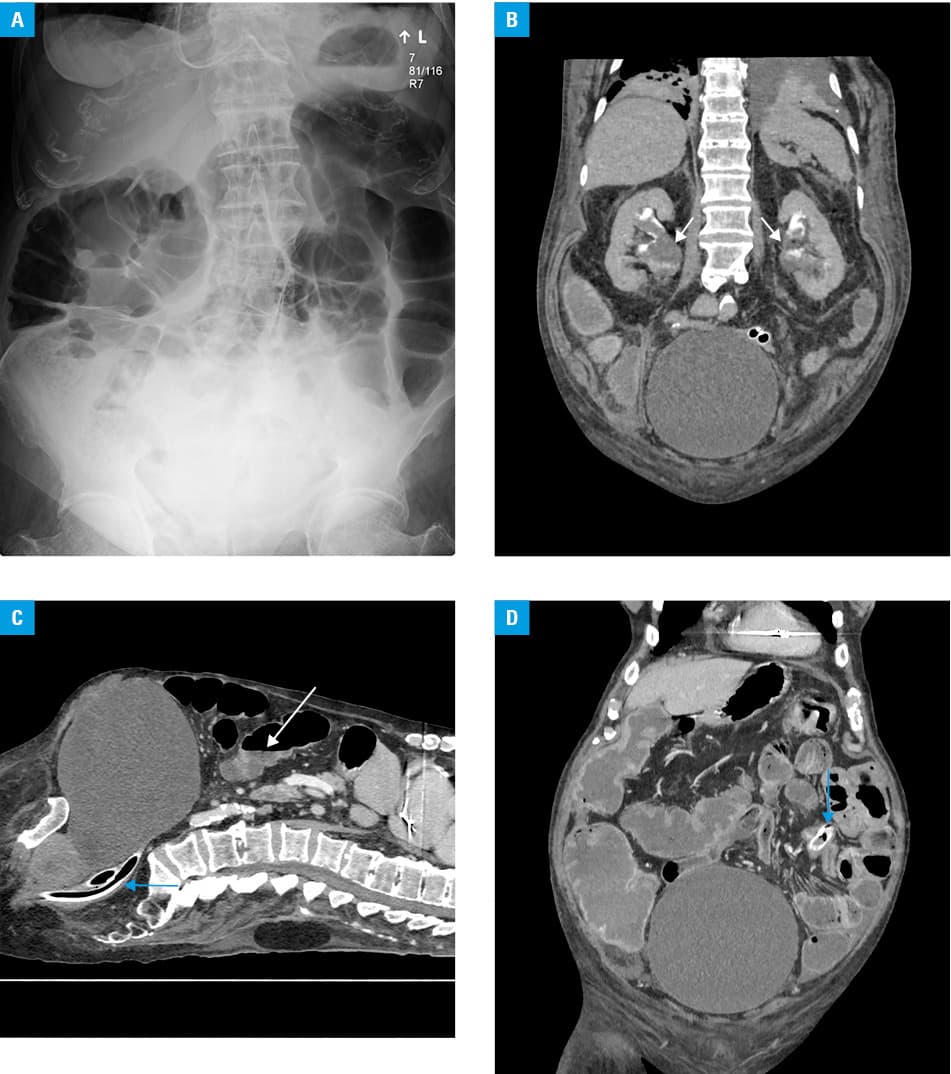
Subsequently, he was transferred to the Surgery Department due to lack of improvement. Before the planned surgery, computed tomography (CT) of the abdomen and pelvis was performed. It revealed an enlarged urinary bladder with diverticula, compressing the rectum against the sacral spine, and dilation of the large and, partially, small bowel loops with fluid levels (Figure 1B–1D). After insertion of a urinary catheter, symptoms of bowel obstruction resolved, and serum levels of both C‑reactive protein and creatinine decreased.
Large bowel obstruction (LBO) is a mechanical blockage of intestinal contents caused predominantly by colonic malignancy (>60%) and entities such as diverticulitis, colonic volvulus, or adhesions. Extrinsic compression is an uncommon cause of LBO (<5%), triggered mainly by abscesses.1
Our case shows an unusual presentation of bowel obstruction caused by a giant bladder with diverticula with supposed atony. In such cases of lower gastrointestinal obstruction, CT imaging proves to be more useful than plain X‑ray. We assume that the primary cause of the gastrointestinal obstruction, bladder enlargement, and bilateral urostasis was oligosymptomatic stage IV benign prostatic hyperplasia.
A similar case was described by Ghebontni et al,2 where bladder atony was associated with long‑standing diabetes mellitus and prostatic disease, as in our patient. A more frequent cause of bowel obstruction is giant vesical diverticula, described in 14 cases in the English medical literature to date. However, in all of them, colonic obstruction was accompanied by complete urinary retention, unlike in our patient, which makes the present case unique.3,4
- Jaffe T, Thompson WM. Large‑bowel obstruction in the adult: classic radiographic and CT findings, etiology, and mimics. Radiology. 2015; 275: 651‑663. | Crossref
- Ghebontni L, el‑Khoury J, Nguyen‑Khaç E, et al. Subacute intestinal obstruction due to bladder distension. J Radiol. 1998; 79: 880‑882.
- Koubaa S, Ben Salah FZ, Miri I, et al. Neurogenic bladder in diabetes mellitus. Tunis Med. 2009; 87: 279‑282.
- Akbulut S, Cakabay B, Sezgin A, et al. Giant vesical diverticulum: a rare cause of defecation disturbance. World J Gastroenterol. 2009; 15: 3957‑3959. | Crossref
ARTICLE INFORMATION