Erdheim‑Chester disease with orbital involvement and progressive impairment of vision



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Erdheim‑Chester disease with orbital involvement and progressive impairment of vision
A 40‑year‑old man was referred to our hospital due to orbitopathy of unknown reason. The patient had had exophthalmos for 2 years with progressive reduction of visual acuity (VA) in both eyes for 3 months preceding the admission. The physical examination revealed xanthelasmata of the eyelids (Figure 1A), asymmetrical proptosis (30 mm and 26 mm of the right and left eye, respectively; norm for Caucasians <20 mm), substantial limitation of the eye motility in all directions, and inconstant double vision. VA decreased as per Snellen Tables (0.4 and 1.0 in the right and left eye, respectively; normal VA, 1.0). Autoimmune thyroid disease was ruled out. Elevated serum C‑reactive protein concentration (24 mg/l; upper limit of normal, 10 mg/l) was found without any significant abnormalities in other laboratory tests (Supplementary material, Tables S1 and S2). Magnetic resonance imaging of the head showed bilateral well delimited infiltrations in the eye sockets (Figure 1B–1D). Computed tomography of the chest and abdominal cavity revealed the aorta surrounded by a soft tissue, approximately 5 mm thick (“coated aorta”). Both kidneys were peripherally infiltrated (“hairy kidneys”) (Figure 1E–1F). Radiographs of the knee joints showed symmetrical, bilateral cortical sclerosis of the long bones (Figure 1G). Immunohistochemical testing of the lesion in the orbits revealed infiltration with histiocytic cells expressing CD68 and CD163; S100 and CD1a were negative. Molecular tests confirmed BRAFV600E mutation. A diagnosis of Erdheim‑Chester disease (ECD) was made.
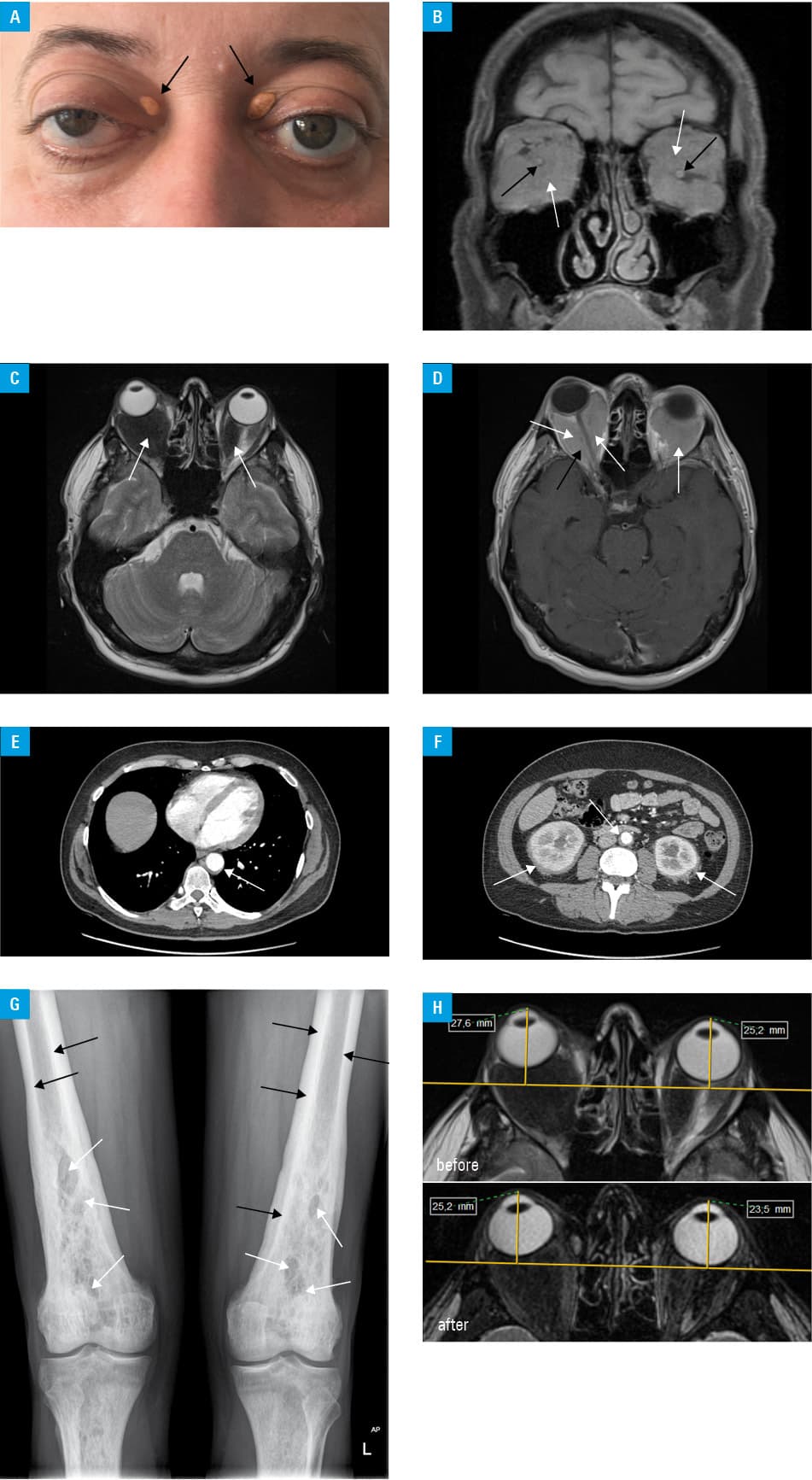
The patient received methylprednisolone in pulses with transient improvement in VA. The therapy with pegylated interferon was started subcutaneously (135 µg per week for 2 months). The treatment was unsuccessful, and cladribine (4 cycles every 28 days, 5 mg/m2, days 1 through 5) was administered. Stabilization of the disease was obtained as assessed by imaging (Figure 1H), the patient declared improvement in VA and no feeling of tension within the orbits. This was confirmed by ophthalmological tests (Supplementary material, Table S3), and xanthelasmata were significantly reduced. The patient undergoes active surveillance. Due to the lack of infiltration, regression, and not achieving normal vision, vemurafenib, a selective BRAF kinase inhibitor is planned to be initiated.
ECD is a non‑Langerhans form of histiocytosis that can involve any organ system, such as the skeleton, central nervous system, orbits, pericardium, retroperitoneum, lungs, kidneys, and skin.1-4 Diagnosis of ECD is often challenging due to its highly variable presentation, multisystem involvement, and the rarity of the disease.1,2 Only 1500 cases have been reported so far, however, the frequency seems highly underestimated. Twenty‑five percent of all reported patients seem to have orbital involvement.1 The disease has a characteristic bone scan and retroperitoneal fibrosis resulting in “hairy kidneys” and “coated aorta.”1-3 It is essential to interpret histopathological features together with clinical, radiographic, and molecular findings to make a correct diagnosis.1,2,4 Interferon-α is the initial treatment of ECD in situations when molecularly targeted drugs, that is, BRAF and MEK inhibitors are unavailable. Other classic options include cladribine, anakinra, methotrexate, tocilizumab, and infliximab.1,2,4
- Haroche J, Cohen‑Aubart F, Amoura Z. Erdheim‑Chester disease. Blood. 2020; 135: 1311‑1318. | Crossref
- Goyal G, Heaney ML, Collin M, et al. Erdheim‑Chester disease: consensus recommendations for evaluation, diagnosis, and treatment in the molecular era. Blood. 2020; 135: 1929‑1945. | Crossref
- Kumar P, Singh A, Gamanagatti S, et al. Imaging findings in Erdheim‑Chester disease: what every radiologist needs to know. Pol J Radiol. 2018; 83: e54‑e62. | Crossref
- Verschelden G, Van Laethem J, Velkeniers B, et al. Significant response to dabrafenib in a patient with Erdheim‑Chester disease with BRAFV600E mutation. Pol Arch Intern Med. 2018; 128: 386‑388. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION