Nationwide data on epidemiology of inflammatory bowel disease in Poland between 2009 and 2020
Key words: epidemiology, inflammatory bowel disease, Poland, population data



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Nationwide data on epidemiology of inflammatory bowel disease in Poland between 2009 and 2020
Introduction: The epidemiology of inflammatory bowel disease (IBD) in Poland has been recognized to only a limited extent.
Objectives: We aimed to estimate the prevalence and incidence of IBD by analyzing data from the National Health Fund, Poland’s sole public health insurer.
Patients and methods: Administrative health claims collected over the 2009–2020 period were used to identify patients with Crohn’s disease (CD) or ulcerative colitis (UC). A definition of a case comprised at least 2 records assigned K50 or K51 codes, plus at least 2 prescriptions for IBD drugs reimbursed, or else intestinal surgery preceding the record. The crude and European age‑standardized rates (EASR) and 95% CIs were calculated for prevalence and incidence. Time trends were also analyzed.
Results: As of 2020, there were 23 574 patients with CD and 73 235 with UC. The CD and UC prevalence was respectively 61.6 (EASR 60.3) and 191.4 (EASR 187.85) per 100 000. The prevalence of CD and UC was higher in men (64.1; EASR 61.3 and 201.4; EASR 202.7, respectively) than in women (59.3; EASR 58.4 and 182.0; EASR 175.5, respectively). The incidence of CD was 4.7 per 100 000 (EASR 4.6), and that of UC 12.5 (EASR 12.3). Through the period 2012–2018, the prevalence of both conditions was rising, even though downward trends were noted for the disease incidence.
Conclusions: The prevalence and incidence of IBD in Poland are presented, with time trends showing a substantial increase in the disease burden over the years 2009–2020.
What's new?
In Poland, there are limited data concerning the epidemiology of inflammatory bowel disease, including Crohn’s disease and ulcerative colitis. However, since 2009 the National Health Fund (Narodowy Fundusz Zdrowia), the sole public health insurer in Poland, has been running an electronic database of health services that comprises individually reported data claimed to the payer by service providers. We therefore drew on that source in this article, in order to estimate the prevalence and incidence of the disease in the cases assigned a K50 or K51 diagnosis under the International Statistical Classification of Diseases and Related Health Problems, Tenth Revision (ICD‑10). Based on this, we demonstrated a substantial increase in the disease burden over the years 2009–2020. We believe these data are of importance at the national level, and may also prove useful as the changing epidemiology of inflammatory bowel disease in Europe is analyzed.
Introduction
The prevalence of inflammatory bowel disease (IBD), that is of both Crohn’s disease (CD) and ulcerative colitis (UC), has increased substantially in many regions of the world in the last few decades.1 The severity and chronicity of the disease have a strong impact on patients’ quality of life, including the role they are able to play in the society, with a substantial burden on health care systems also imposed. Evidence from the research literature points to a changing epidemiology of IBD, with a stable or decreased incidence in North America and Europe, even as the incidence grows in newly‑industrialized countries. However, most studies have originated in high‑income countries, with countries of lower socioeconomic status producing fewer population‑based studies that report on the epidemiology of IBD.1
Poland is a developing country with a high‑income economy, and one that has in fact grown steadily from the time of the fall of communism (in 1989) through to 2019.2 In this period, the epidemiology of IBD in Poland has only been recognized to a limited degree.
A study using population data from the years 2012–2014 showed IBD prevalence of 157 per 100 000 individuals for Poland.3 Furthermore, an analysis of hospitalization rates for IBD in the years 1991–1996 and 2003–2007 showed that the rates for both CD and UC increased each year, though no nationwide data on the incidence of IBD were available.4
As the health care system in Poland is based on universal health insurance, the National Health Fund (Narodowy Fundusz Zdrowia [NFZ]) is the only public health care payer that finances the health care services provided to the insured people and reimburses medicines. Since 2009, NFZ has been running an electronic database of health services that comprises individually reported data claimed to the payer by service providers. We aimed to benefit from that situation by assessing the epidemiology of IBD in Poland in the previous decade on the basis of prevalent and incident cases in the NFZ database assigned a K50 or K51 diagnosis under the International Statistical Classification of Diseases and Related Health Problems, Tenth Revision (ICD‑10).
Patients and methods
Data source
The analysis was performed by reference to details of administrative health claims collected in the NFZ databases. Under the health insurance system in place in Poland, the NFZ is the only state payer that covers the entire population of the country.
To identify patients with CD or UC, we analyzed data from 2 of NFZ electronic databases, that is, those relating to services and prescribed drugs. Data collected in these databases are anonymized but individual patients can be distinguished and matched by their IDs, which are pseudonymized numbers in the Polish Resident Identification Number (PESEL) system.
The NFZ electronic database on services comprises individually reported data based around claims submitted to the payer by service providers. For the purposes of the work described here, we used data from 2009 through to 2020. These include a detailed description of the service, patient demographic data, and information about the provider. Each service claimed to the NFZ is reported along with the date of admission, date of discharge, and a list of procedures performed. Each service is reported obligatorily, along with the ICD‑10 code assigned to it by a health care professional.
The NFZ electronic database on drugs comprises information on all prescriptions for reimbursed medicines filled and billed after 2012, the year in which the database was launched. It specifically includes the information on the prescribed medicines (their trade names, active ingredients, and European Article Numbers), date of prescription issue, and date of prescription completion.
Data on patient deaths were obtained from the Poland’s PESEL system, in which all citizens and long‑term residents are registered with a number, along with sex, date of birth, and date of death, among other things.
Data on the size of the population in Poland in the years 2009–2020 were obtained from the Statistics Poland (GUS), formerly the Central Statistical Office of Poland, the government executive agency responsible for the collection and publishing of statistical data.
Crohn’s disease and ulcerative colitis prevalence and incidence
The algorithm used for the identification of CD and UC patients is presented in Supplementary material, Figure S1. We selected individuals meeting the following criteria: at least 2 services in hospital or outpatient specialist care reported with K50 or K51 ICD‑10 code, and (1) at least 2 prescriptions filled for IBD drugs (listed in Supplementary material, Table S1) with an interval of at least 2 months, or (2) an intestinal surgery episode with one of the defined ICD‑9 codes (Supplementary material, Table S2) preceding at least 1 service reported with K50 or K51 ICD‑10 code. In the next step, the patients were classified as sufferers from either CD or UC, on the basis of the ICD‑10 code reported with their last service received. This way, each patient was assigned to the group with 1 or these 2 diagnoses.
In the patients identified with the above methods, the date of the first service reported with K50 or K51 code was considered to mark the onset of the disease.
Due to the fact that the oldest records in the NFZ database are from 2009, the incidence for the first few years of the analysis was overestimated. For this reason, we assumed that the patients identified as incident cases in 2009–2011 might have been diagnosed before 2009. On the other hand, as the incidence in the most recent years of the analysis was underestimated, we proceeded on the assumption that the patients who developed IBD symptoms for the first time in 2019 or 2020 might not yet have met the criteria applied by us. Limited access to health care services during the COVID‑19 pandemic might have contributed to this situation. We therefore examined the epidemiological trends over the period 2012–2018.
The crude rate was calculated by dividing the number of cases by the population size. The European age‑standardized rate (EASR) was calculated using data from the 2013 European Standard Population (ESP),5 and 95% CIs were calculated using normal approximation.
Sensitivity of the algorithm
To test the sensitivity of our algorithm, we compared the group of patients selected based on the algorithm with the group in whom biological treatment for IBD was provided by hospitals and reimbursed by NFZ. We assumed that the patients who received biological treatment represented the group of confirmed diagnosis. Biological drugs are not reimbursed outside hospital settings in Poland. The patients were identified in the NFZ databases by specific diagnosis‑related group products reported with the services.
Among all 4618 patients treated with biological drugs for IBD in the years 2012–2018, 4583 (99.2%) met our criteria for diagnosis of CD or UC. However, when the diseases were analyzed separately, the precision of the algorithm seemed lower. Among the 3379 patients treated with biological drugs for CD, 3214 (95.1%) were assigned by the algorithm to the CD group, and 136 (4.0%) to the UC group. Similarly, among the 1306 individuals treated with biological drugs for UC, 1244 (95.3%) were assigned to the UC group, and 56 (4.3%) to the CD group. It is worth noting that 67 patients (1.5%) were treated with biological drugs sequentially for either CD or UC.
Statistical analysis
Incidence cases in a given year were defined as the number of individuals showing an onset of the disease in that year, and at least 2 reported services with K50 or K51 ICD‑10 code designations between 2009 and 2020. Prevalence cases in a given year were defined as the sum of incidence cases in that year and previous years, excluding the deceased. Incidence and prevalence rates per 100 000 inhabitants were calculated by dividing the number of cases by the number of inhabitants at the end of a given year, multiplied by 100 000. The EASR was calculated using the direct standardization method as based around the 2013 ESP used as a reference.5,6 The calculations were performed using the R programming language, version 3.6.2 (R Foundation for Statistical Computing, Vienna, Austria), as well as the “data.Table” packages (version 1.12.8).
Joinpoint regression was used to analyze temporal trends for incidence and prevalence. Annual percentage rates (APC) and corresponding 95% CIs were calculated. A permutation test was used in the model selection. Subgroup comparisons were carried out using the parallel testing.7 The relatively short study period (just 7 years from 2012 to 2018) accounted for the non‑adjustment of P values for multiple comparisons. All hypotheses were tested at 0.05 significance level. The Joinpoint regression was performed in the Joinpoint Regression Program, Version 4.9.0.0 (Statistical Research and Applications Branch, National Cancer Institute, Calverton, United States).
Ethics
The study was approved by the Bioethical Committee of the Maria Sklodowska‑Curie National Research Institute of Oncology (Decision 73/2021).
Results
The population of Crohn’s disease and ulcerative colitis patients in Poland
The aforementioned electronic databases run by the NFZ and covering the years 2009–2020 allowed us to identify 124 249 people hospitalized or served during a specialist visit at least 2 times due to K50 or K51 diagnosis. By selecting from within this group the patients receiving prescriptions for IBD drugs or having intestinal surgeries, we reduced the population identified initially by reference to the 2 records by some 17%. It was in relation to this reduced population that the date of the first service reported with a K50 or K51 designation was considered to mark the disease onset (Supplementary material, Figure S1). As of 2020, Poland had 23 574 identified patients with CD (including 1730 children and teenagers aged 0–19), as well as 73 235 patients with UC (including 2064 aged 0–19) (Figure 1 and 2, Table 1 and 2, and Supplementary material, Figure S1, Tables S3 and S11).
Year | Cases | Population | Crude rate (per 100 000 population) | EASR | 95% LCL | 95% UCL |
Abbreviations: EASR, European age‑standardized rate; LCL, lower limit of control; UCL, upper limit of control | ||||||
2009 | 5016 | 38 167 329 | 13.1 | 12.2 | 11.9 | 12.6 |
2010 | 7172 | 38 529 866 | 18.6 | 17.4 | 17.0 | 17.9 |
2011 | 9155 | 38 538 447 | 23.8 | 22.4 | 21.9 | 22.8 |
2012 | 11 107 | 38 533 299 | 28.8 | 27.3 | 26.8 | 27.9 |
2013 | 13 022 | 38 495 659 | 33.8 | 32.2 | 31.6 | 32.7 |
2014 | 14 953 | 38 478 602 | 38.9 | 37.1 | 36.5 | 37.7 |
2015 | 16 784 | 38 437 239 | 43.7 | 41.9 | 41.3 | 42.6 |
2016 | 18 477 | 38 432 992 | 48.1 | 46.4 | 45.7 | 47.1 |
2017 | 20 125 | 38 433 558 | 52.4 | 50.8 | 50.0 | 51.5 |
2018 | 21 712 | 38 411 148 | 56.5 | 55.0 | 54.2 | 55.7 |
2019 | 23 058 | 38 382 576 | 60.1 | 58.6 | 57.9 | 59.4 |
2020 | 23 574 | 38 265 013 | 61.6 | 60.3 | 59.5 | 61.0 |
Year | Cases | Population | Crude rate (per 100 000 population) | EASR | 95% LCL | 95% UCL |
Abbreviations: see Table 1 | ||||||
2009 | 16 561 | 38 167 329 | 43.4 | 43.4 | 42.8 | 44.1 |
2010 | 23 727 | 38 529 866 | 61.6 | 61.8 | 60.9 | 62.6 |
2011 | 30 401 | 38 538 447 | 78.9 | 79.0 | 78.1 | 79.9 |
2012 | 37 755 | 38 533 299 | 98.0 | 98.0 | 97.0 | 99.1 |
2013 | 44 013 | 38 495 659 | 114.3 | 114.1 | 113.0 | 115.2 |
2014 | 49 758 | 38 478 602 | 129.3 | 128.6 | 127.4 | 129.7 |
2015 | 55 005 | 38 437 239 | 143.1 | 141.8 | 140.6 | 143.0 |
2016 | 59 924 | 38 432 992 | 155.9 | 154.2 | 153.0 | 155.5 |
2017 | 64 468 | 38 433 558 | 167.7 | 165.8 | 164.5 | 167.1 |
2018 | 68 546 | 38 411 148 | 178.5 | 176.0 | 174.7 | 177.4 |
2019 | 72 080 | 38 382 576 | 187.8 | 184.8 | 183.4 | 186.2 |
2020 | 73 235 | 38 265 013 | 191.4 | 187.8 | 186.5 | 189.2 |
This denoted an identified total of 96 809 IBD patients (0.25% of the total population of Poland), meaning that approximately 1 in every 400 of the country’s inhabitants was affected by IBD. Of these, 3794 patients were within the 0–19 age range.
Crohn’s disease
The prevalence of Crohn’s disease
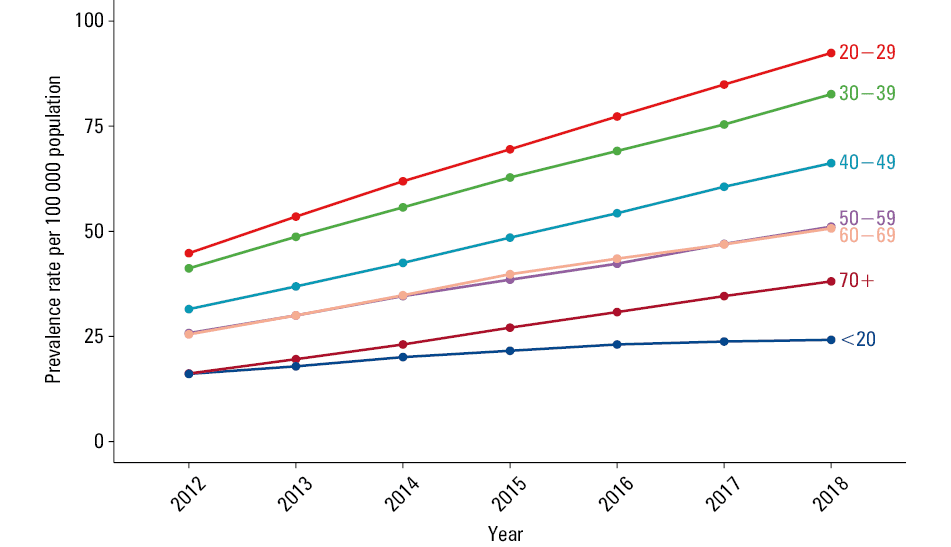
As of 2020, the crude prevalence of CD was 61.6 (EASR 60.3; 95% CI, 59.5–61.0) per 100 000 (Table 1, Figure 1).
The prevalence of CD per 100 000 inhabitants was slightly higher in men (64.1; EASR 61.3; 95% CI, 60.2–62.5) than in women (59.3; EASR 58.4; 95% CI, 57.3–59.5) (Supplementary material, Tables S4 and S5).
The prevalence of CD was the highest in the 20–29 age group, reaching 101.1 patients per 100 000 inhabitants (Supplementary material, Table S3 and Figure S2).
Temporal trends for the prevalence of Crohn’s disease
Between 2012 and 2018, the prevalence of CD in the Polish population rose significantly year by year, albeit with the rate of increase greater for 2012–2015 (APC = 14.8; 95% CI, 12.4–17.3) than for 2015–2018 (APC = 8.7; 95% CI, 6.8–10.5, Supplementary material, Table S6). The upward trend was true of both men and women, though the rate of increase declined in 2015 for both sexes. Our analysis for different age groups revealed an increase in prevalence each year, though its rate was higher between 2012 and 2015 than between 2015 and 2019.
The incidence of Crohn’s disease
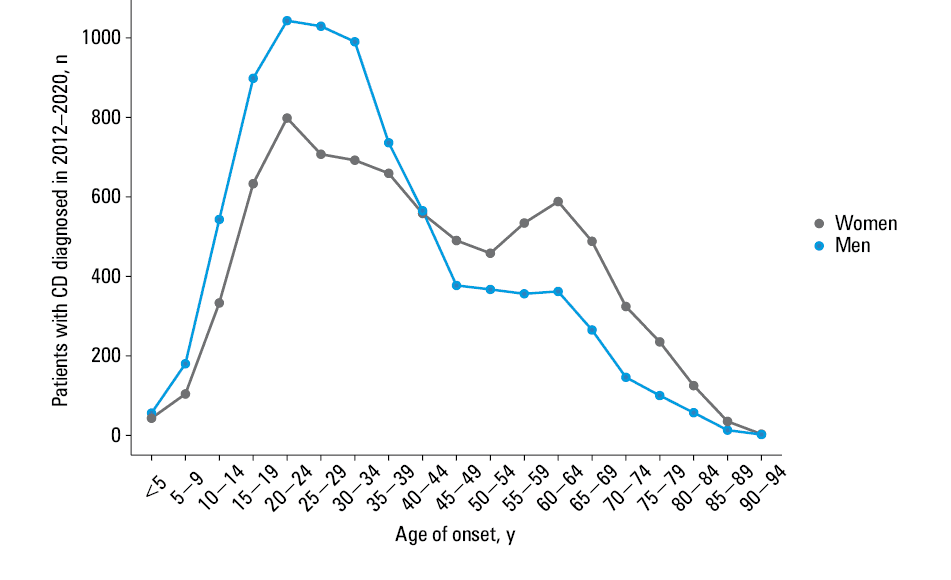
In 2018, the crude annual incidence of CD was 4.7 per 100 000 (EASR 4.6; 95% CI, 4.4–4.8), and was higher in men (4.9 per 100 000; EASR 4.7; 95% CI, (4.4–5.0) than in women (4.5 and 4.4, 95% CI, 4.2–4.7, respectively) (Table 3, Figure 2 and Supplementary material, Tables S7 and S8).
Year | Cases | Population | Crude rate (per 100 000 population) | EASR | 95% LCL | 95% UCL |
Abbreviations: see Table 1 | ||||||
2009 | 5022 | 38 167 329 | 13.2 | 12.3 | 11.9 | 12.6 |
2010 | 2170 | 38 529 866 | 5.6 | 5.3 | 5.0 | 5.5 |
2011 | 2011 | 38 538 447 | 5.2 | 4.9 | 4.7 | 5.1 |
2012 | 2000 | 38 533 299 | 5.2 | 5.0 | 4.8 | 5.2 |
2013 | 2003 | 38 495 659 | 5.2 | 5.0 | 4.7 | 5.2 |
2014 | 2046 | 38 478 602 | 5.3 | 5.2 | 4.9 | 5.4 |
2015 | 1980 | 38 437 239 | 5.2 | 5.1 | 4.8 | 5.3 |
2016 | 1869 | 38 432 992 | 4.9 | 4.8 | 4.6 | 5.0 |
2017 | 1817 | 38 433 558 | 4.7 | 4.7 | 4.5 | 4.9 |
2018 | 1794 | 38 411 148 | 4.7 | 4.6 | 4.4 | 4.8 |
2019 | 1584 | 38 382 576 | 4.1 | 4.1 | 3.9 | 4.4 |
2020 | 799 | 38 265 013 | 2.1 | 2.1 | 2.0 | 2.3 |
The incidence of CD was the highest in the 20–29 age group, reaching 8.2 cases per 100 000 (Supplementary material, Table S9). However, it was only slightly lower in the 10–19 age group (7.2 per 100 000). Following a gradual decline in the incidence in the 4th, 5th, and 6th decade of life, another rise was observed in the 60–69 age group (3.9 per 100 000).
Temporal trends for the incidence of Crohn’s disease
Over the years 2014–2018, we observed a downward trend for the incidence of CD in the Polish population (APC = –6.7; 95% CI, –7.9 to –5.4, Supplementary material, Table S10). This was present in both men and women. However, no differences were noted when the trends were compared in particular age groups.
Ulcerative colitis
The prevalence of ulcerative colitis
As of 2020, the crude prevalence of UC was 191.4 per 100 000 (EASR, 187.85; 95% CI, 186.5–189.2) (Table 2, Figure 3).
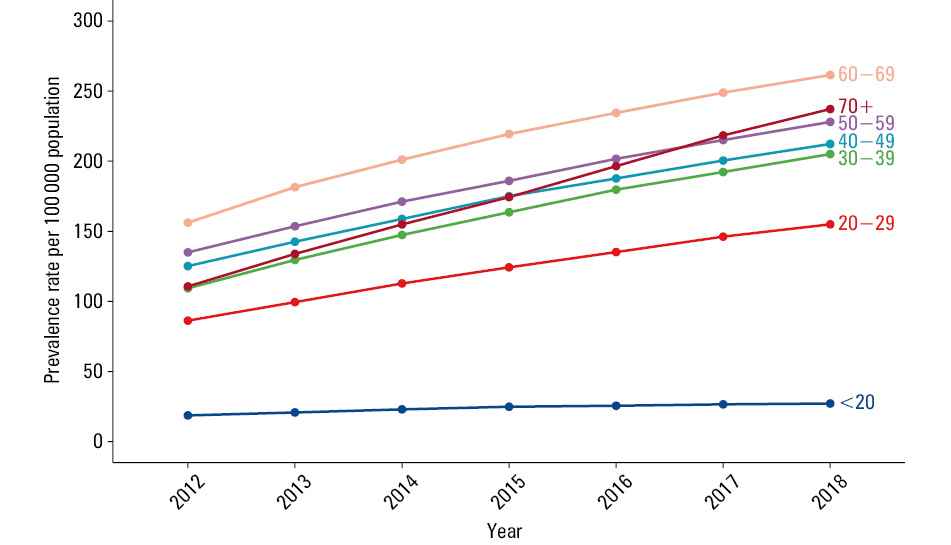
The prevalence of UC was substantially higher in men (201.4 per 100 000; EASR, 202.7; 95% CI, 200.5–204.8) than in women (182.0 per 100 000; EASR, 175.5; 95% CI, 173.7–177.4) (Supplementary material, Tables S12 and S13).
The prevalence of UC was the highest in the 60–69 age group, reaching 275 patients per 100 000 inhabitants (Supplementary material, Table S11 and Figure S3).
Time trends in the prevalence of ulcerative colitis
In the years 2012–2018, the prevalence of UC in the Polish population rose significantly year by year but the rate of the increase was greater in the years 2012–2015 (APC = 13.4; 95% CI, 10.0–16.8) than in 2015–2018 (APC = 7.3; 95% CI, 4.7–10.0, Supplementary material, Table S14). The upward trend was present among both men and women, while the rate of the increase was lower in 2015 for both sexes. The increase in UC prevalence was observed each year in all age groups, but there were significant differences in its magnitude. The greatest rise was observed in the oldest (60+) group, while the smallest in the youngest people (aged 0–20).
In all age groups a decline in the rate of UC prevalence increase was seen through the 2015–2018 period, as compared with 2012–2015.
The incidence of ulcerative colitis
As of 2018, the crude annual incidence of UC was 12.5 per 100 000 (EASR 12.3; 95% CI, 12.0–12.7), higher in men (13.7 per 100 000, EASR 13.5; 95% CI, 13.0–14.1) than in women (11.4 and EASR 11.2; 95% CI, 10.7–11.7) (Table 4, Figure 4, Supplementary material, Tables S15 and S16).
Year | Cases | Population | Crude rate (per 100 000 population) | EASR | 95% LCL | 95% UCL |
Abbreviations: see Table 1 | ||||||
2009 | 16 565 | 38 167 329 | 43.4 | 43.5 | 42.8 | 44.1 |
2010 | 7175 | 38 529 866 | 18.6 | 18.6 | 18.2 | 19.0 |
2011 | 6684 | 38 538 447 | 17.3 | 17.2 | 16.7 | 17.6 |
2012 | 7492 | 38 533 299 | 19.4 | 19.3 | 18.8 | 19.7 |
2013 | 6570 | 38 495 659 | 17.1 | 16.8 | 16.4 | 17.3 |
2014 | 6137 | 38 478 602 | 15.9 | 15.6 | 15.2 | 16.0 |
2015 | 5736 | 38 437 239 | 14.9 | 14.6 | 14.2 | 15.0 |
2016 | 5485 | 38 432 992 | 14.3 | 14.0 | 13.6 | 14.4 |
2017 | 5187 | 38 433 558 | 13.5 | 13.3 | 12.9 | 13.7 |
2018 | 4808 | 38 411 148 | 12.5 | 12.3 | 12.0 | 12.7 |
2019 | 4340 | 38 382 576 | 11.3 | 11.2 | 10.9 | 11.5 |
2020 | 2309 | 38 265 013 | 6.0 | 6.0 | 5.8 | 6.2 |
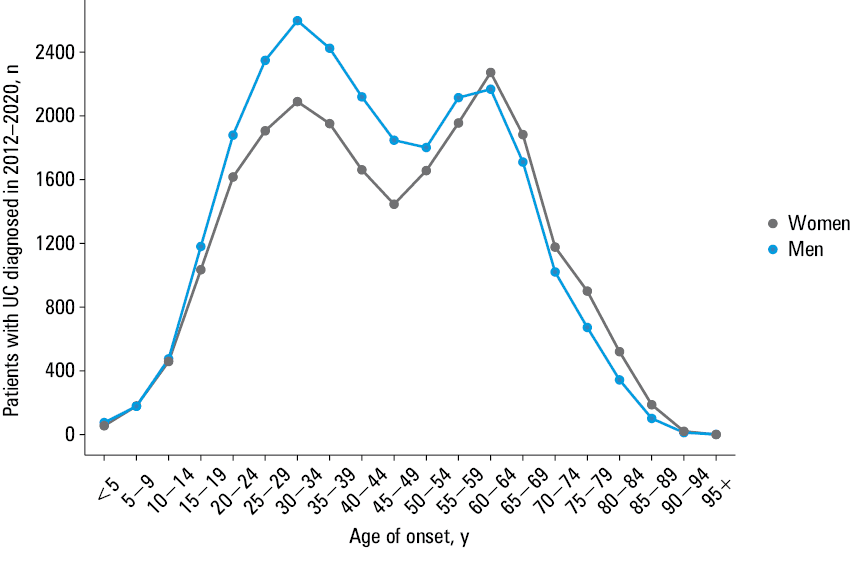
The annual incidence of UC was the highest in the 20–29 age group, reaching 16.4 cases per 100 000 (Supplementary material, Table S17). In the 2 first decades of life (0–9 and 10–19), the incidences were 1.6 and 9.5 per 100 000, respectively. Interestingly, the second most risky decade of life was 60–69, with the incidence of 15.8 per 100 000 (Figure 3, Supplementary material, Table S17).
Temporal trends in ulcerative colitis incidence
The years 2012–2018 witnessed a downward trend for the incidence of UC in the Polish population (APC = –6.7; 95% CI, –7.9 to –5.4, Supplementary material, Table S18), with the rate of decline proving similar throughout that period. The downward trend was visible for both men and women.
However, the analysis of different age groups showed constant incidence in the youngest (0–20) group (APC = 2.2; 95% CI, –0.3 to 4.7), which differed from all the other age groups. Interestingly, the fall in UC incidence in the 40–59 and 60+ age groups was slower in the years 2014–2018 (APC = –6.5; 95% CI, –7.8 to –5.2) than in 2012–2014 (APC = –14.1; 95% CI, –17.3 to –10.9).
Discussion
This paper is the first to present nationwide data on the incidence and prevalence of IBD in Poland. Indeed, the incidence of IBD in Poland has not been investigated so far, and there is no national registry of patients. It is the recent digitalization of the reimbursement process in the national health care system that has allowed us to perform the analyses based on ICD‑10 and ICD‑9 coding. The methodology we employed was also used in recent epidemiological studies from Denmark and Israel.8,9
As the analysis of the Danish National Patient Registry demonstrated, the number of records chosen to define IBD cases influenced the estimated incidence to a great extent.9 The greatest difference in the incidence in the Danish study was found when the results were based on at least 1 record vs at least 2 records. For this reason, we chose the latter option as we sought to analyze the Polish data. Similarly to Stulman et al,9 we also chose to apply an additional criterion involving reimbursed prescriptions for IBD drugs, and added an alternative criterion of IBD‑related surgery, in line with a presumption that some proportion of IBD patients failed to receive pharmacological treatment following the surgery.8
A total of 96 809 patients ultimately identified in the year 2020 represent 0.25% of the population of Poland, with age‑standardized prevalence of 60.3 and 187.8 per 100 000 population for CD and UC, respectively.
Two main differences can be seen as these data are set against the global population of IBD patients. First, while the prevalence of both conditions is higher in Polish men than women, the global trend is reverse, with a significant prevalence of IBD in women.1 In a systematic review of IBD incidence by Molodecky et al,10 the authors reported women to men ratios of 0.51–1.58 for UC, and 0.34–1.65 for CD. The differences of this type seem to depend on geographical area.10 Therefore, while in Western Europe and North America IBD is more often diagnosed in women, in Central Europe the opposite is true, as our data serve to confirm. In Western Europe and the United States, the prevalence of CD again appears to be higher in women than in men.11,12 An approximately 3‑fold prevalence of UC over CD occuring in Poland is responsible for greater number of men among the Polish IBD patients. Moreover, the presence of various other types of colitis, including that associated with diverticular disease, ischemic colitis, microscopic colitis, or the increasingly common immune checkpoint inhibitor–induced colitis, and their wrong classification, might contribute to the prevalence of K51 (UC) over K50 (CD) diagnosis.
The maximum IBD prevalence in Poland is observed at the age of 30–44 years, which is in contrast to the age of 45–64 years observed in the global IBD population.1 This observation suggests that a rise in the incidence of IBD in Poland began later than in the countries now reporting the highest frequency of the disease. Furthermore, a decline in the prevalence of CD may be noticed in the older age groups, in contrast to the prevalence of UC that seems to rise with age. This might suggest that a rise in the incidence of UC in Poland preceded that related to CD by a few decades.
According to recent analyses concerning the burden of IBD, its prevalence is seen to vary substantially between countries. In 2017, the overall prevalence of IBD in Western Europe was 136.6 per 100 000, even as Eastern Europe reported a lower prevalence of 104.5 per 100 000.1,13 The CD prevalence ranged from 1.5 (Romania) to 331 (the Netherlands), and UC prevalence per 100 000 was from 2.4 (Romania) to 432 (Scotland). Our data pointing to a continuously rising prevalence of IBD beyond the average Eastern European level, need to be taken into account while planning for the regional health care systems.
Geographical gradients in IBD prevalence running from West to East and from North to South are in line with the trends noted for incidence.14 While the incidence of CD in Poland was 4.6 per 100 000, that of UC was 12.3. A similar dominance of UC characterizes the countries of Northern Europe, including Denmark, Finland, Iceland, and the United Kingdom. CD is the more frequent presentation of IBD in Southern Europe (Portugal, Spain) and Israel.8,15-17 Among Central and Eastern European Countries (CEEC), the incidences of CD and UC are closer to each other. The population of Poland seems to follow the Northern pattern, even as Polish values for the prevalence and incidence look distinctly lower than those in the most affected regions. In a multinational European population‑cohort study undertaken by the European Crohn’s and Colitis Organisation (ECCO) (though not including Poland), the median incidence of CD in the CEEC was reported at 3.3 per 100 000, while the value for UC was 4.6. Nationwide studies using central databases tend to generate higher IBD prevalence and incidence values than prospective registries with predefined strict criteria where diagnosis is concerned. That said, the values in our study were considerably higher for both diagnoses than in the ECCO study.15
It is worth noting how Poland’s younger generations are characterized by a more limited dominance of UC over CD. Thus, the prevalence of UC equal to 158.5 per 100 000 in the 20–29 age group and 26.9 for those aged 0–19 years, should be set against the values of 101.1 and 22.5, respectively, for CD. The incidence of UC was at 16.4 per 100 000 in the case of patients aged 20–29, as opposed to 5.5 in the group including those aged 0–19. The incidences of CD were 8.2 and 4.0, respectively. The Figures for the incidence among the youngest members of the society seem particularly concerning, as they are clearly higher than in the report from a prospective Polish registry study covering the years 2002–2004 (which places Poland among the countries with high occurrence of IBD in the pediatric population).18-20
Our analysis of trends for the years 2012–2018 showed increasing prevalence of both CD and UC (in line with global data), even as incidences declined. While we were only able to study a relatively short period of time, having no national data from the past to offer a comparison, stable or decreasing IBD incidences have already been reported by some authors in North America or Europe.10 A repetition of similar analysis in the future will be necessary to confirm current results describing national level trends in Poland.
There are several limitations to our study. First, we analyzed the data from the National Health Fund that do not include patients from the private health care sector. Due to shortcomings of the public system in Poland, the contribution of the private sector to endoscopic diagnostics and gastroenterological care may be substantial. According to a recent report from the GUS, the share of private funds spent on specialist care in Poland was as high as 42%, even as the corresponding number for hospital treatment was just 5.2%.21
This implies that some IBD patients with mild to moderate disease may have been treated outside the public sector, and remained unidentified by the algorithm we used.
Another weakness of our analysis is a lack of histological confirmation of IBD in the identified cases, as the histopathological results are not available in the national databases. Pathological examination is not essential to the diagnosis of IBD, but one of its roles is to distinguish between IBD and other, including acute, bowel inflammations. This is why, with a view to limit the number of false‑positive cases identified by ICD‑10 alone, we used additional criteria related to drugs and surgery. Apart from that, the validation of our algorithm showed that its precision in CD or UC diagnosis was lower by a few per cent than in IBD diagnosis. Ultimately, as the Polish databases established recently cover a relatively short period of time, the results of our trend analyses will need to be confirmed through the use of data collected in the future.
In conclusion, we present Polish national data of an epidemiological nature for IBD cases in the years 2009–2020. These were obtained from the electronic database of Poland’s National Health Fund. The prevalence of both CD and UC seems to be rising above the average values for CEEC. Meanwhile, the population of UC patients is almost 3 times as high as that of patients with CD, with men diagnosed more often with either disease. The prevalence of CD is higher in the younger than the older generations, while evaluation of the trends over time suggests reduced incidences of both CD and UC. We believe these data are of importance at the national level, especially for those involved in shaping the health policy, as well as medical professionals dealing with IBD patients, and, last but not least, the patients themselves. In addition, our results may prove useful as the changing epidemiology of IBD in Europe is analyzed.
- GBD 2017 Inflammatory Bowel Disease Collaborators. The global, regional, and national burden of inflammatory bowel disease in 195 countries and territories, 1990‑2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet Gastroenterol Hepatol. 2020; 5: 17‑30.
- International Monetary Fund. April 2020 WEO Database‑Country Data Documentation. https://www.imf.org › WEO › weo‑database › April. Accessed August 17, 2021.
- Holko P, Kawalec P, Stawowczyk E. Prevalence and drug treatment practices of inflammatory bowel diseases in Poland in the years 2012‑2014. Eur J Gastroenterol Hepatol. 2018; 30: 456‑464. | Crossref
- Jakubowski A, Zagórowicz E, Kraszewska E, Bartnik W. Rising hospitalization rates for inflammatory bowel disease in Poland. Pol Arch Med Wewn. 2014; 124: 180‑190. | Crossref
- Pace M, Gissler M, Lanzieri G, et al. Revision of the European Standard Population: report of Eurostat’s task force: 2013 edition. Eurostat (European Comission) Publications Office; 2013. https://op.europa.eu/en/publication‑detail/-/publication/69399636‑1113‑4a38‑9ad1‑269c33d0dc01/language‑en. Accessed October 7, 2021.
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION