Exposure to polycyclic aromatic hydrocarbons and its relationship with increased expression of human epididymal secretory protein 4
Key words: human epididymal secretory protein 4, NHANES, ovarian cancer, polycyclic aromatic hydrocarbons



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Exposure to polycyclic aromatic hydrocarbons and its relationship with increased expression of human epididymal secretory protein 4
Introduction: Ovarian cancer is the most lethal gynecologic malignancy, and its early detection is important for prognosis. Human epididymal secretory protein 4 (HE4) elevation has been studied as a crucial biomarker for this type of cancer. There are currently many organic pollutants in the environment, including polycyclic aromatic hydrocarbons (PAHs).
Objectives: The purpose of our study was to determine relationships between PAH exposure, HE4 levels, and the risk for ovarian cancer.
Patients and methods: We included a total of 799 participants over the age of 20 years from the United States National Health and Nutrition Examination Survey datasets (2001–2002) with complete data on urinary PAH metabolites and HE4 levels for multivariable analysis. A multivariable linear regression model was used to investigate the associations between PAH metabolites and HE4 in ovarian cancer.
Results: Multivariable linear regression analysis showed that except for 2‑hydroxyphenanthrene, PAH metabolites correlated positively with ln(HE4) after adjustment for relevant covariates (all P <0.05). Higher quartiles of urinary concentrations of PAH metabolites tended to be associated with higher HE4 levels, with statistical significance in per‑quartile analysis. A dose‑dependent relationship between PAH metabolites and HE4 was found (all P trends <0.05).
Conclusions: Exposure to PAHs was found to be associated with elevated HE4 levels and a higher risk for ovarian cancer, which was confirmed by epidemiological evidence. This finding should alert gynecologists and public health experts to pay more attention to the potential role of PAH metabolites in the tumorigenesis of ovarian cancer.
What's new?
Ovarian cancer is a gynecologic malignancy associated with the highest mortality, and the patient’s prognosis largely depends on its early detection. Human epididymal secretory protein 4 (HE4) is considered a crucial biomarker for ovarian cancer. Polycyclic aromatic hydrocarbons (PAHs) are a class of organic pollutants currently present in the environment. The purpose of our study was to investigate the effects of PAH exposure and elevated HE4 levels on the risk for ovarian cancer. The potential pathogenic mechanism by which PAHs may induce ovarian cancer is considered to be mediated by the aryl hydrocarbon receptor (AhR) present in different ovarian cells. Subsequent AhR signaling pathways are potentially carcinogenic, with an elevated expression of AhR in ovarian cancer cell lines. Our results indicated that exposure to PAHs was associated with elevated HE4 levels and a higher risk for ovarian cancer. Exposure to PAH metabolites may be a crucial factor in predicting the risk for ovarian cancer.
Introduction
Ovarian cancer is the most lethal gynecologic malignancy, with a 5‑year survival rate ranging from less than 20% to approximately 90%, depending on the staging of the tumor.1 It is well known that early detection of ovarian cancer is important for prognosis. There are 2 common algorithms for predicting the risk of ovarian cancer; namely, the risk of malignancy index (RMI), including ultrasound findings and architectural features of the pelvic mass, cancer antigen 125 (CA125) levels, and the menopausal status; and the risk of ovarian malignancy algorithm (ROMA) including CA125 levels, human epididymal secretory protein 4 (HE4) levels, and the menopausal status.2 Of these, it was shown that ROMA had a significantly more accurate detection rate, with higher sensitivity than RMI.3
HE4, a member of the family of acidic 4‑disulfide core proteins secreted by epithelial cells,4 is found in multiple normal human tissues, such as the female genital system, including the endocervix, endometrial glands, fallopian tubes, epithelium of the breast, the respiratory epithelium, distal renal tubules, colonic mucosa, and salivary glands.5 High expression of HE4 has been investigated and considered a potential crucial biomarker for detecting and monitoring ovarian cancer, especially for the identification of benign ovarian tumors and malignant ovarian carcinomas.5,6 However, some factors may interfere with HE4 expression. For example, smoking and age are the 2 major factors that affect and increase the level of HE4 in humans7; elevated HE4 levels have also been noted in renal failure, liver disease,8 type 2 diabetes mellitus, and hypertension.9 In contrast, pregnancy is associated with lower HE4 levels.10
There are currently many organic pollutants in the environment, including polycyclic aromatic hydrocarbons (PAHs).11 PAHs comprise a group of compounds composed of 2 or more fused benzene rings formed through processes associated with industrial waste, vehicular exhaust, unburned fossil fuel, and cigarette smoke, and they are thought to be carcinogenic.12 Recent studies have further identified PAHs as harmful to human health, with strong evidence that exposure to these compounds led to different carcinomas in experimental animal models, showing a significant relationship with lung and breast cancer.13,14
Over the past few years, a number of studies have been conducted on the role of PAHs in changing female fertility and inducing serious reproductive disorders, such as anovulation, reduced pregnancy rates, and menstrual abnormalities.15 However, most studies exploring the relationship between PAHs and ovarian cancer have been superficial and limited, and there has been no in‑depth research to date investigating the associations between PAH exposure, HE4 levels, and ovarian cancer. The purpose of our study was to reveal the effects of PAHs and HE4 on the risk for ovarian cancer.
Patients and methods
Study design and population
Our study sample was derived from the United States National Health and Nutrition Examination Survey (NHANES) conducted by the National Centers for Health Statistics, a part of the Centers for Disease Control and Prevention. The NHANES study combined interviews and physical examinations at a mobile examination center to assess the health and nutritional status of adults and children in the United States. We included 11 039 adult participants from the NHANES survey over the age of 20 years assessed between 2001 and 2002. We excluded men and those with missing data on HE4 levels, urinary PAH concentrations, or other relevant covariates, as specified below. Finally, we analyzed 799 participants with complete data of interest for multivariable analysis (Figure 1). The study was approved by the NHANES Institutional Review Board Protocol no. 98–12, and all participants signed the informed consent prior to participation.
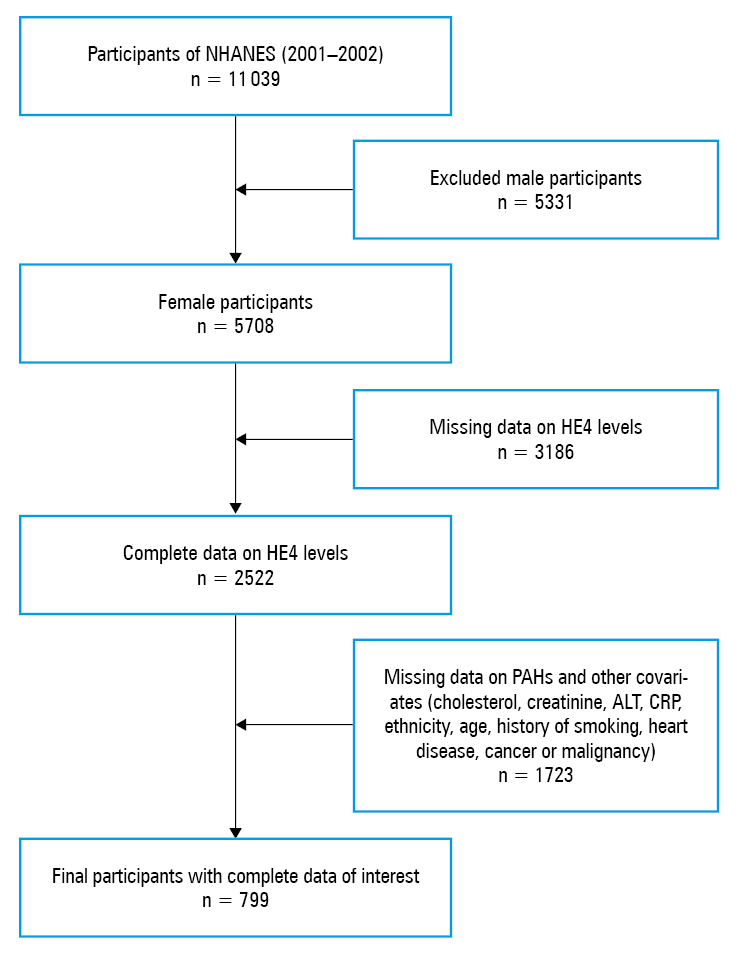
Abbreviations: ALT, alanine aminotransferase; CRP, C‑reactive protein; HE4 human epididymal secretory protein 4; NHANES, the United States National Health and Nutrition Examination Survey; PAHs, polycyclic aromatic hydrocarbons
Measurement of human epididymal secretory protein 4
Levels of HE4 were assessed using the Meso Scale Discovery electrochemiluminescence immunoassay platform under standardized operational procedures and quality control protocols at the Genital Tract Biology Laboratory, Brigham and Women’s Hospital, Boston, Massachusetts, United States. The linearity range of HE4 was 0.1 to 466.9 pmol/l, and the acceptable quality control pool variation was set at 25%.
Measurement of urinary polycyclic aromatic hydrocarbons
Single spot urine samples were collected and stored at –20 °C. Urinary PAH concentrations were examined using capillary gas chromatography combined with high‑resolution mass spectrometry under standardized operational procedures and quality control protocols of the NHANES Laboratory / Medical Technologists Procedures Manual. In our study, we assessed hydroxylated PAH metabolites, including 1‑hydroxynaphthalene, 2‑hydroxynaphthalene, 2‑hydroxyfluorene, 3‑hydroxyfluorene, 1‑hydroxyphenanthrene, 2‑hydroxyphenanthrene, 3‑hydroxyphenanthrene, and 1‑hydroxypyrene.
Measurement of covariates
Demographic information was collected in participants’ homes prior to the health examination, using the computer‑assisted personal interviewing technique. The selected demographic variables included age, sex, and ethnicity (Mexican American, other Hispanic, non‑Hispanic White, non‑Hispanic Black, or other). Medical condition was assessed based on self‑reported personal interview data on health conditions, including a history of any diagnosis made by a physician and the smoking status. The level of cholesterol was measured with the Beckman Synchron LX20 analyzer system and the level of creatinine, with the Beckman Synchron CX3 clinical analyzer system (Beckman Coulter Inc., Brea, California, United States). The Hitachi 917 multichannel analyzer system (Roche Diagnostics, Indianapolis, Indiana, United States) was used to determine the level of alanine aminotransferase (ALT), and C‑reactive protein (CRP) levels were assessed using the Dade Behring Turbidimetry II Analyzer System (Dade Behring Diagnostics Inc., Somerville, New Jersey, United States).
Statistical analysis
In our study, all analyses were performed using the International Business Machines Statistical Package for the Social Sciences, version 22.0 for Windows (SPSS Inc., Chicago, Illinois, United States). The levels of HE4 were considered a dependent variable; they were evaluated using the Kolmogorov–Smirnov normality test and were not normally distributed. Natural log transformation was performed to normalize the distributions of HE4 levels. A linear regression model was applied to explore the relationship between HE4 levels and PAH concentrations. Associations between HE4 levels and PAH concentrations were adjusted for the following models: Model 1 = age and ethnicity; Model 2 = Model 1 + cholesterol, creatinine, ALT, and CRP; Model 3 = Model 2 + smoking, history of congestive heart failure (CHF), coronary heart disease (CHD), angina pectoris, cancer or malignancy, diabetes mellitus, and hypertension. Statistical significance was defined as a P value equal or below 0.05. We divided urinary PAH levels into 4 quartiles and used the first quartile as the reference group. Dose‑dependent relationships between PAH metabolites and HE4 were investigated.
Results
Characteristics of the study participants Characteristics of the study group (n = 799) are listed in Table 1. The median (interquartile range [IQR]) age was 45 (31–64) years. The median (IQR) values of baseline laboratory variables were as follows: cholesterol, 201 (175–227) mg/dl; creatinine, 0.7 (0.6–0.8) mg/dl; ALT, 18 (14–23) U/l, and C‑reactive protein, 0.29 (0.11–0.64) mg/dl. The median values of individual PAH metabolites are also listed in Table 1.
Variable | Value | |
Continuous variables are presented as medians (interquartile ranges), continuous variables are presented as numbers (percentages).
SI conversion factors: to convert total cholesterol to mmol/l, multiply by 0.0259; creatinine to μmol/l, by 88.4; ALT to μkat/l, by 0.0167; CRP to mg/l, by 10.
Abbreviations: see Figure 1 | ||
Age, y | 45 (31–64) | |
HE4, pmol/l | 15.44 (10.30–23.41) | |
Total cholesterol, mg/dl | 201 (175–227) | |
Creatinine, mg/dl | 0.7 (0.6–0.8) | |
ALT, U/l | 18 (14–23) | |
C‑reactive protein, mg/dl | 0.29 (0.11–0.64) | |
1‑hydroxynaphthalene, ng/l | 1599 (744–4500) | |
2‑hydroxynaphthalene, ng/l | 2267 (955–5570) | |
3‑hydroxyfluorene, ng/l | 85 (44–178) | |
2‑hydroxyfluorene, ng/l | 242 (121–488) | |
3‑hydroxyphenanthrene, ng/l | 86 (42–170) | |
1‑hydroxyphenanthrene, ng/l | 135 (68–244) | |
2‑hydroxyphenanthrene, ng/l | 51 (23.5–104) | |
1‑hydroxypyrene, ng/l | 40 (20–82.25) | |
Ethnicity | Mexican American | 193 (24.2) |
Other Hispanic | 31 (3.9) | |
Non‑Hispanic White | 348 (43.5) | |
Non‑Hispanic Black | 197 (24.7) | |
Other | 30 (3.7) | |
At least 100 cigarettes in lifetime | 375 (46.9) | |
Congestive heart failure | 18 (2.3) | |
Coronary heart disease | 34 (4.3) | |
Angina pectoris | 24 (3.0) | |
Cancer or malignancy | 66 (8.2) | |
Diabetes mellitus | 49 (6.1) | |
Hypertension | 223 (27.9) | |
Associations between polycyclic aromatic hydrocarbon concentrations and human epididymal secretory protein 4 levels
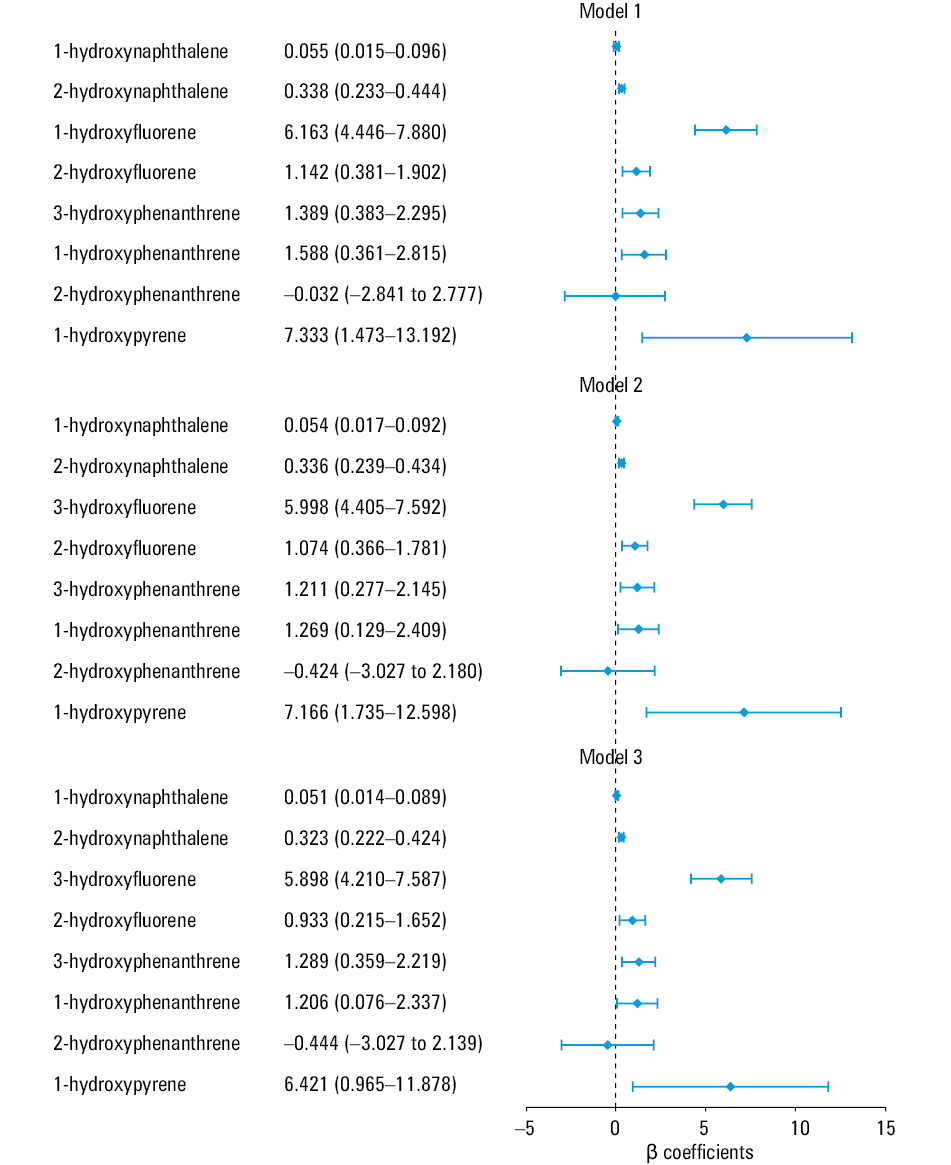
Multivariable linear regression analysis (Figure 2) showed that except for 2‑hydroxyphenanthrene, concetrations of PAH metabolites correlated positively with HE4 levels. The regression coefficients between PAH concentrations and ln(HE4) were as follows: 1‑hydroxynaphthalene, 0.055 (P = 0.007), 0.054 (P = 0.004), and 0.051 (P = 0.007) for Models 1, 2, and 3, respectively; 2‑hydroxynaphthalene, 0.338 (P ≤0.001), 0.336 (P ≤0.001), and 0.323 (P ≤0.001) for Models 1, 2, and 3, respectively; 3‑hydroxyfluorene, 6.163 (P ≤0.001), 5.998 (P ≤0.001), and 5.898 (P ≤0.001) for Models 1, 2, and 3, respectively; 2‑hydroxyfluorene, 1.142 (P = 0.003), 1.074 (P = 0.003), and 0.933 (P = 0.01) for Models 1, 2, and 3, respectively; 3‑hydroxyphenanthrene, 1.389 (P = 0.007), 1.211 (P = 0.01), and 1.289 (P = 0.007) for Models 1, 2, and 3, respectively; 1‑hydroxyphenanthrene, 1.588 (P = 0.01), 1.269 (P = 0.03), and 1.206 (P = 0.04) for Models 1, 2, and 3, respectively; 2‑hydroxyphenanthrene, –0.032 (P = 0.98), –0.424 (P = 0.75), and –0.444 (P = 0.74) for Models 1, 2, and 3, respectively; 1‑hydroxypyrene, 7.333 (P = 0.01), 7.166 (P = 0.01), and 6.421 (P = 0.02) for Models 1, 2, and 3, respectively.
Associations between different quartile levels of polycyclic aromatic hydrocarbons and human epididymal secretory protein 4 levels
Analysis of the 4 quartiles of PAH metabolites concentrations is shown in Table 2. The median HE4 levels in different quartiles of PAHs are listed in Table 3. A dose‑dependent relationship between PAH metabolites and HE4 levels was found. A signifcant positive correlation was noted in the higher quartiles of 1‑hydroxynaphthalene, 2‑hydroxyfluorene, 3‑hydroxyphenanthrene, and 1‑hydroxypyrene in all models as compared with the lowest quartile. P values for the trends between quartiles of PAH metabolites and ln(HE4) were as follows: 1‑hydroxynaphthalene, all P <0.001; 2‑hydroxyfluorene, P = 0.003, P = 0.003, and P =0.03 for Models 1, 2 and 3, respectively; 3‑hydroxyphenatherene, P = 0.005, P = 0.01, and P = 0.03 for Models 1, 2 and 3, respectively; 1‑hydroxypyrene, P = 0.009, P = 0.003, and P = 0.02 for Models 1, 2 and 3, respectively. The regression coefficients observed in the higher quartiles of PAH metabolites were higher than those in the lower quartiles.
PAH metabolitea,b | Q2 vs Q1 | Q3 vs Q1 | Q4 vs Q1 | P for trend | ||||
β (95% CI) | P value | β (95% CI) | P value | β (95% CI) | P value | |||
a Adjusted covariates: Model 1: age + ethnicity; Model 2: Model 1 + cholesterol + creatinine + ALT + CRP; Model 3: Model 2 + history of smoking, congestive heart failure, coronary heart disease, angina / angina pectoris, cancer or malignancy, diabetes mellitus, and / or hypertension
b Independent variables: 1‑hydroxynaphthalene, 2‑hydroxynaphthalene, 3‑hydroxyfluorene, 2‑hydroxyfluorene, 3‑hydroxyphenanthrene, 1‑hydroxyphenanthrene, 2‑hydroxyphenanthrene, 1‑hydroxypyrene; dependent variable: HE4
Abbreviations: Q, quartile; others, see Figure 1 | ||||||||
1‑Hydroxynaphthalene | Model 1 | 0.036 (–0.106 to 0.178) | 0.62 | 0.169 (0.031–0.307) | 0.02 | 0.341 (0.202–0.481) | <0.001 | <0.001 |
Model 2 | 0.023 (–0.117 to 0.162) | 0.75 | 0.150 (0.014–0.286) | 0.03 | 0.308 (0.170–0.445) | <0.001 | <0.001 | |
Model 3 | 0.015 (–0.125 to 0.156) | 0.83 | 0.143 (0.006–0.280) | 0.04 | 0.266 (0.123–0.410) | <0.001 | <0.001 | |
2‑Hydroxynaphthalene | Model 1 | –0.035 (–0.178 to 0.108) | 0.63 | –0.054 (–0.197 to 0.089) | 0.46 | 0.138 (–0.008 to 0.284) | 0.06 | 0.09 |
Model 2 | –0.040 (–0.180 to 0.100) | 0.57 | –0.055 (–0.195 to 0.085) | 0.44 | 0.127 (–0.016 to 0.269) | 0.08 | 0.11 | |
Model 3 | –0.048 (–0.189 to 0.093) | 0.50 | –0.070 (–0.211 to 0.072) | 0.33 | 0.074 (–0.075 to 0.224) | 0.33 | 0.44 | |
3‑Hydroxyfluorene | Model 1 | –0.069 (–0.209 to 0.071) | 0.34 | –0.084 (–0.226 to 0.057) | 0.24 | 0.205 (0.063 to 0.346) | 0.005 | 0.008 |
Model 2 | –0.059 (–0.196 to 0.079) | 0.40 | –0.082 (–0.221 to 0.057) | 0.25 | 0.196 (0.057 to 0.335) | 0.006 | 0.01 | |
Model 3 | –0.074 (–0.212 to 0.065) | 0.30 | –0.099 (–0.238 to 0.041) | 0.17 | 0.144 (–0.003 to 0.291) | 0.06 | 0.11 | |
2‑Hydroxyfluorene | Model 1 | –0.032 (–0.172 to 0.109) | 0.66 | 0.026 (–0.115 to 0.166) | 0.72 | 0.210 (0.068,0.352) | 0.004 | 0.003 |
Model 2 | –0.025 (–0.163 to 0.113) | 0.72 | 0.026 (–0.112 to 0.164) | 0.72 | 0.208 (0.003–0.069) | 0.003 | 0.003 | |
Model 3 | –0.031 (–0.169 to 0.107) | 0.66 | 0.018 (–0.120 to 0.157) | 0.79 | 0.162 (0.017–0.307) | 0.03 | 0.03 | |
3‑Hydroxyphenanthrene | Model 1 | –0.066 (–0.208 to 0.077) | 0.37 | –0.003 (–0.145 to 0.138) | 0.96 | 0.196 (0.054–0.339) | 0.007 | 0.005 |
Model 2 | –0.055 (–0.195 to 0.085) | 0.44 | –0.009 (–0.148 to 0.129) | 0.89 | 0.181 (0.041–0.321) | 0.01 | 0.01 | |
Model 3 | –0.063 (–0.204–0.077) | 0.38 | –0.029 (–0.168 to 0.110) | 0.68 | 0.154 (0.012–0.296) | 0.03 | 0.03 | |
1‑Hydroxyphenanthrene | Model 1 | –0.044 (–0.186 to 0.097) | 0.54 | –0.078 (–0.220 to 0.064) | 0.28 | 0.147 (0.004–0.290) | 0.04 | 0.08 |
Model 2 | –0.053 (–0.192 to 0.085) | 0.45 | –0.084 (–0.223 to 0.055) | 0.24 | 0.143 (0.003–0.283) | 0.05 | 0.08 | |
Model 3 | –0.079 (–0.218 to 0.060) | 0.27 | –0.103 (–0.242 to 0.036) | 0.15 | 0.116 (–0.026 to 0.257) | 0.11 | 0.16 | |
2‑Hydroxyphenanthrene | Model 1 | –0.003 (–0.145 to 0.140) | 0.97 | –0.041 (–0.183 to 0.101) | 0.57 | 0.115 (–0.031 to 0.260) | 0.12 | 0.20 |
Model 2 | 0.010 (–0.130 to 0.149) | 0.89 | –0.022 (–0.162 to 0.118) | 0.76 | 0.120 (–0.023 to 0.262) | 0.10 | 0.16 | |
Model 3 | –0.016 (–0.156 to 0.124) | 0.82 | –0.041 (–0.182 to 0.100) | 0.57 | 0.090 (–0.054 to 0.235) | 0.22 | 0.30 | |
1‑Hydroxypyrene | Model 1 | 0.09 (–0.133 to 0.152) | 0.89 | 0.025 (–0.116 to 0.167) | 0.73 | 0.198 (0.054–0.342) | 0.007 | 0.009 |
Model 2 | 0.013 (–0.126 to 0.153) | 0.85 | 0.046 (–0.092 to 0.185) | 0.51 | 0.215 (0.075–0.356) | 0.003 | 0.003 | |
Model 3 | –0.011 (–0.151 to 0.129) | 0.88 | 0.031 (–0.108 to 0.170) | 0.66 | 0.177 (0.032–0.322) | 0.02 | 0.02 | |
Quartile | 1‑Hydroxynaphthalene | 2‑Hydroxynaphthalene | 3‑Hydroxyfluorene | 2‑Hydroxyfluorene | 3‑Hydroxyphenanthrene | 1‑Hydroxyphenanthrene | 2‑Hydroxyphenanthrene | 1‑Hydroxypyrene |
HE4, pmol/l, median | ||||||||
Q1 | 16.726 | 21.794 | 18.655 | 18.599 | 19.013 | 18.963 | 19.756 | 20.085 |
Q2 | 17.435 | 18.006 | 19.085 | 18.267 | 16.557 | 18.863 | 20.064 | 19.435 |
Q3 | 18.661 | 16.038 | 17.359 | 18.239 | 18.328 | 18.036 | 17.018 | 17.200 |
Q4 | 23.996 | 21.005 | 21.717 | 21.722 | 22.976 | 21.095 | 20.065 | 20.149 |
Discussion
Our analysis revealed a close relationship between urinary concentrations of PAH metabolites and HE4 levels in adult American women. First, we found most PAH metabolites to positively correlate with HE4 levels, except for 2‑hydroxyphenanthrene. When comparing the different quartiles of PAH metabolites, higher concentrations were associated with higher HE4 levels. Therefore, the dose‑dependent correlation between PAHs and HE4 was also positive. To the best of our knowledge, this is the first study to report a relationship between PAH metabolites and HE4 levels.
The carcinogenic mechanism associated with occupational exposure to PAHs has been fully demonstrated in patients with lung cancer.16 Occupational exposure to PAHs in different industries, including coke ovens, generator gas production, coal gasification, and roof and chimney sweeping, is associated with a higher risk of lung cancer.17 Several epidemiological studies have also shown that PAH exposure is related to an increased risk of breast cancer.18 Certain industrial PAH exposures, such as the production of aluminum and coal gasification, are associated with an increased risk of bladder cancer.19 In addition, higher dermal PAH exposure increases the risk of skin cancer.20 Similarly, in our study, increased exposure to PAH metabolites was significantly associated with elevated HE4 levels, an important clinical sign of ovarian cancer. Therefore, it can be speculated that PAH exposure could also enhance the risk of ovarian cancer through elevated HE4 levels.
There have been numerous scientific attempts to elucidate the carcinogenic mechanism of PAHs. PAHs can quickly and easily enter the body through all exposure pathways because they are rich in carbon and hydrophobic.21 PAHs do not directly induce DNA damage and are considered procarcinogens.22 A single PAH is converted into hydroxylated and glucuronide metabolites, and these modified molecules are generally safely excreted from the body. However, some of the intermediate forms cause genetic damage before being removed and contribute to cancer formation.21
Most of the widely known effects of PAH exposure are mediated by the aryl hydrocarbon receptor (AhR). PAH is an exogenous ligand that directly binds to AhR.23 AhR is activated by various ligands, both endo- and exogenous. The functions of AhR ligands differ, and the regulatory roles of this receptor are both physiological and pathophysiological. The downstream effects include organism detoxification, antiproliferative activity, neurodevelopmental activity, cancer promotion, cell migration, inability to renew stem cells, and inflammation.24,25 PAHs are exogenous ligands that bind to AhR, activating a transcription factor that translocates to the nucleus and binds to the AhR nuclear translocator (ARNT) to produce an active heterodimer. ARNT binds to xenobiotic‑responsive elements to promote the expression of target genes24 that encode drug‑metabolizing enzymes such as cytochrome P450 (CYP) 1A1, 1A2, and 1B1, which are phase 1 metabolizing enzymes. CYP enzymes catalyze the biotransformation of xenobiotics such as PAHs. As mentioned above, this biochemical process sometimes produces toxic and reactive intermediates of xenobiotics, which increase the production of reactive oxygen species.26 This may lead to DNA, RNA, and protein damage, cell proliferation, carcinogenesis, and even cell death.27
Ovarian tissue has 2 main physiological roles in the female reproductive system. First, the ovary manages follicle development, differentiation, and oocyte release for fertilization.28 Second, the tissue controls the synthesis and secretion of sex steroid hormones, which are important for the maintenance of follicular development, fertility, menstrual cycle, and pregnancy.29 Several studies revealed that the AhR protein and transcript are present in different ovarian cells such as oocytes, granulosa cells, and theca cells in different species, including humans, mice, and monkeys.30-32 As previously mentioned, certain AhR signaling pathways are potentially carcinogenic.33 Some studies found elevated AhR expression in ovarian cancer cell lines.34
PAHs are harmful to human health in many ways. Excessive exposure to 1‑hydroxynaphthalene and 2‑hydroxynaphthalene can damage red blood cells and cause hemolytic anemia, most commonly in people with inherited glucose‑6‑phosphate dehydrogenase deficiency.35 Among all PAH metabolites, the 1‑hydroxypyrene subgroup in Models 1 to 3 showed a significant positive correlation with HE4 levels. This may be due to the fact that 1‑hydroxypyrene is a metabolite of all PAHs present at relatively high concentrations, and the most common biomarker representing total PAH exposure.36,37 A high level of hydroxyfluorene is associated with low high‑density lipoprotein cholesterol levels, which could be harmful to the antioxidant system.38,39 C‑reactive protein, a biomarker of oxidative stress and inflammation as well as creatinine, as a marker of renal function, have been found to be positively associated with PAH levels.40 Liver dysfunction was also found to be associated with exposure to PAHs.41 The oxidative and inflammatory effects of PAHs cause DNA damage and methylation, and play a key role in carcinogenesis.42,43 PAHs also induce peroxisome proliferator–activated receptors and disrupt tissue homeostasis.44 The latter process leads to activation of the immune response, which also contributes to the development of ovarian cancer.45
There are some limitations to the present study. First, because it was a cross‑sectional and not a longitudinal study, the temporality of the association between HE4 levels and PAHs could not be determined. Second, the enrolled participants with available HE4 data in the NHANES 2001–2002 dataset were older than 20 years. Menopausal status, which influences the level of HE4, was not an exclusion criterion in the NHANES survey.46 The median age of our final study group was 45 years. However, our findings cannot be applied to the general population, because the age range of our female participants was 31 to 64 years. Third, our data were collected almost 20 years ago and in the meantime there have been many studies focusing on the changes of PAH concentration in the environment. However, the concentrations of atmospheric PAHs were almost the same or even slightly decreased after 2000.47,48 Thus, even though our study considered the PAHs levels during 2001–2002, they were not very different from their concentration nowadays. Finally, we used a single spot urine sample, which may have not represented the actual concentration of urinary PAH metabolites. Nevertheless, according to a previous study,49 analysis based on a single spot urine sample can still provide trends in the association between PAH exposure and HE4 levels.49
Conclusion
In our study, we discovered a causal association between PAH exposure and elevated HE4 levels, and increased risk for ovarian cancer, which was supported with strong epidemiological evidence. Additionally, our research emphasized the necessity of exploring the pathogenetic mechanism of PAH metabolites for ovarian cancer in association with elevated HE4 levels. Exposure to PAH metabolites may become a crucial factor in ovarian cancer prediction for gynecologists and public health experts to enhance the efficacy and quality of treatment.
- Yang WL, Lu Z, Guo J, et al. Human epididymis protein 4 antigen‑autoantibody complexes complement cancer antigen 125 for detecting early‑stage ovarian cancer. Cancer. 2020; 126: 725‑736. | Crossref
- Moore RG, Jabre‑Raughley M, Brown AK, et al. Comparison of a novel multiple marker assay vs the Risk of Malignancy Index for the prediction of epithelial ovarian cancer in patients with a pelvic mass. Am J Obstet Gynecol. 2010; 203: E1‑E6. | Crossref
- Karlsen MA, Sandhu N, Høgdall C, et al. Evaluation of HE4, CA125, risk of ovarian malignancy algorithm (ROMA) and risk of malignancy index (RMI) as diagnostic tools of epithelial ovarian cancer in patients with a pelvic mass. Gynecol Oncol. 2012; 127: 379‑383. | Crossref
- Kirchhoff C, Habben I, Ivell R, Krull N. A major human epididymis‑specific cDNA encodes a protein with sequence homology to extracellular proteinase inhibitors. Biol Reprod. 1991; 45: 350‑357. | Crossref
- Galgano MT, Hampton GM, Frierson HF. Jr. Comprehensive analysis of HE4 expression in normal and malignant human tissues. Mod Pathol. 2006; 19: 847‑853. | Crossref
ARTICLE INFORMATION