Diagnostic and therapeutic management in gastroesophageal reflux disease: consensus of the Polish Society of Gastroenterology
Key words: endoscopy, gastroesophageal reflux disease, impedance, pH



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Diagnostic and therapeutic management in gastroesophageal reflux disease: consensus of the Polish Society of Gastroenterology
The paper was prepared by an expert group appointed by the Polish Society of Gastroenterology with an aim to update and systematize the knowledge about diagnosis and treatment of gastroesophageal reflux disease (GERD). Based on the previously published guidelines of international societies, expert consensuses, and recently published good quality data, we formulated 74 statements regarding the definition, diagnosis and treatment of GERD and assessed the level of acceptance of these statements and the reliability of the data. We discussed in details the possibilities and limitations of the available diagnostic methods and therapies, with particular emphasis on the diversity of gastroesophageal reflux symptoms and complications including Barrett’s esophagus. Practical principles regarding interpretation of the diagnostic tests are presented. In addition, we discussed the indications for surgical treatment as well as the situations in which surgical treatment is not indicated with emphasis on the importance of preoperative diagnostics. The role of add‑on therapy and indications for maintenance treatment are defined.
Introduction
Significant worldwide incidence of gastroesophageal reflux disease (GERD) and its complications pose serious health, economic and social consequences, including increasing health care costs and a negative impact on patient’s productivity and quality of life.1-4
After abdominal pain, GERD and esophagitis are the second most common causes of outpatient visits. Annual direct and indirect costs of this disease are estimated at $15–20 billion in the United States of America, of which approximately 60% is spent on treatment. The cost of using acid suppressive therapy for various indications in the last 5 years was estimated at approximately $60 billion.5,6
GERD is characterized by a broad spectrum of symptoms and complications that may occur separately or in combination. A gold standard in the diagnosis of GERD still does not exist, and treatment with proton pump inhibitors (PPIs) is often overused. One study showed that over 1/3 of patients receiving a PPI had no documented indications for their chronic use.7
The aim of this study is to update and systematize the knowledge about the possibilities and limitations of available diagnostic methods and therapies, with particular emphasis on the diversity of GERD symptoms. This work presents the consensus on GERD diagnosis and treatment developed by an expert group appointed by the Polish Society of Gastroenterology. It takes into account the guidelines of international societies published in recent years, expert opinions and consensuses, as well as the latest research results. Supplementary material, Part 1 includes Polish version of the consensus.
Methodology
Based on previously published guidelines of international societies and expert consensuses, the main statements regarding the definition, diagnosis and treatment of GERD were formulated, and then assessed by a group of experts appointed by the Polish Society of Gastroenterology. The level of acceptance of the statements (I‑V) and reliability of the data (A‑C) were determined using appropriate rating scales (Tables 1 and 2). The issues important for clinical practice are discussed in detail.
Category | Acceptance level |
I | Full acceptance |
II | Acceptance with minor reservations |
III | Acceptance with major reservations |
IV | Rejection with minor reservations |
V | Full rejection |
Category | Data reliability |
A | High (data based on meta‑analyzes and randomized clinical trials) |
B | Moderate (data based on clinical trials and observational studies) |
C | Low (data mainly based on expert opinion) |
GERD epidemiology
STATEMENT 1. GERD reflux disease has a negative impact on the patients’ quality of life. Pathological gastroesophageal reflux can cause esophagitis, Barrett’s esophagitis, and esophageal adenocarcinoma (A / I‑100%).
In developed countries, GERD prevalence is estimated at approximately 20%, based on the occurrence of heartburn and / or regurgitation 1‑2 times a week.8,9 The prevalence of GERD is estimated at 8.8%–25.9% in Europe, 2.5%–7.8% in Asia, 8.7%–33.1% in the Middle East, 11.6% in Australia, and 23% in South Africa.10 About 25–40% of American adults report heartburn at least once a month, and about 7%–10% of patients experience heartburn every day.11,12 In Poland, among 850 people aged 21‑76, GERD symptoms were reported by 36% of the respondents.13
GERD has a negative impact on the patients’ quality of life. Reduced productivity and physical activity are especially reported by patients with frequent symptoms.14 GERD is equally common among men and women but complications are more common in men: erosive esophagitis (about 2 times more often), Barrett’s esophagus (BE) (about 10 times), and esophageal adenocarcinoma (about 8 times).15-17 Erosive esophagitis was found in 6.4% of patients in China and 15.5% of patients in Sweden in populational studies of patients undergoing endoscopy, regardless of the reported symptoms.18,19 A prospective study found erosions in the esophagus in 26% of patients with non‑erosive reflux disease (NERD) after 2 years,20 while in another study, erosive esophagitis was found in a follow‑up endoscopy after 5 years in 10% of patients.21 GERD is a risk factor for BE, which affects approximately 2% of the population and may progress to esophageal adenocarcinoma.22-24 GERD increases the risk of esophageal adenocarcinoma (odds ratio [OR], 7.7; 95% CI, 5.3–11.4), especially in patients with long‑term GERD and severe or daily symptoms. The risk, however, is low and accounts for less than 0.001% annually.25,26 The risk of esophageal adenocarcinoma in patients with BE is clearly greater in those with at least low‑grade epithelial dysplasia.27-29
Potential pathophysiological factors increasing the risk of GERD include, but are not limited to: lower esophageal sphincter (LES) dysfunction, delayed gastric emptying, impaired esophageal clearance, esophageal motility disorders, obesity, and hiatal hernia.17,30 Several studies reported an association between increased body mass index (BMI), waist circumference, and weight gain, and the presence of GERD symptoms and complications.31-36
Definition and classification of GERD
STATEMENT 2. GERD is a condition that develops when pathological gastric reflux into the esophagus causes troublesome symptoms and / or complications (C / I‑70%, II‑30%)
Acid reflux from the stomach into the esophagus, especially after a meal, is a physiological phenomenon. Therefore, the presence of gastroesophageal reflux or occasional symptoms cannot be defined as a disease. In 2006, a group of 44 experts from 18 countries provided the definition and classification of GERD.9 According to the Montreal Consensus, GERD is a condition that develops when gastric reflux into the esophagus causes troublesome symptoms and / or complications. Thus, GERD diagnosis can be made on the basis of the presence of troublesome heartburn and / or regurgitation or GERD complications as a consequence of pathological reflux. Troublesome symptoms are symptoms that have a negative impact on the patient’s quality of life. Most often these are mild symptoms reported at least twice a week or more severe symptoms at least once a week.9
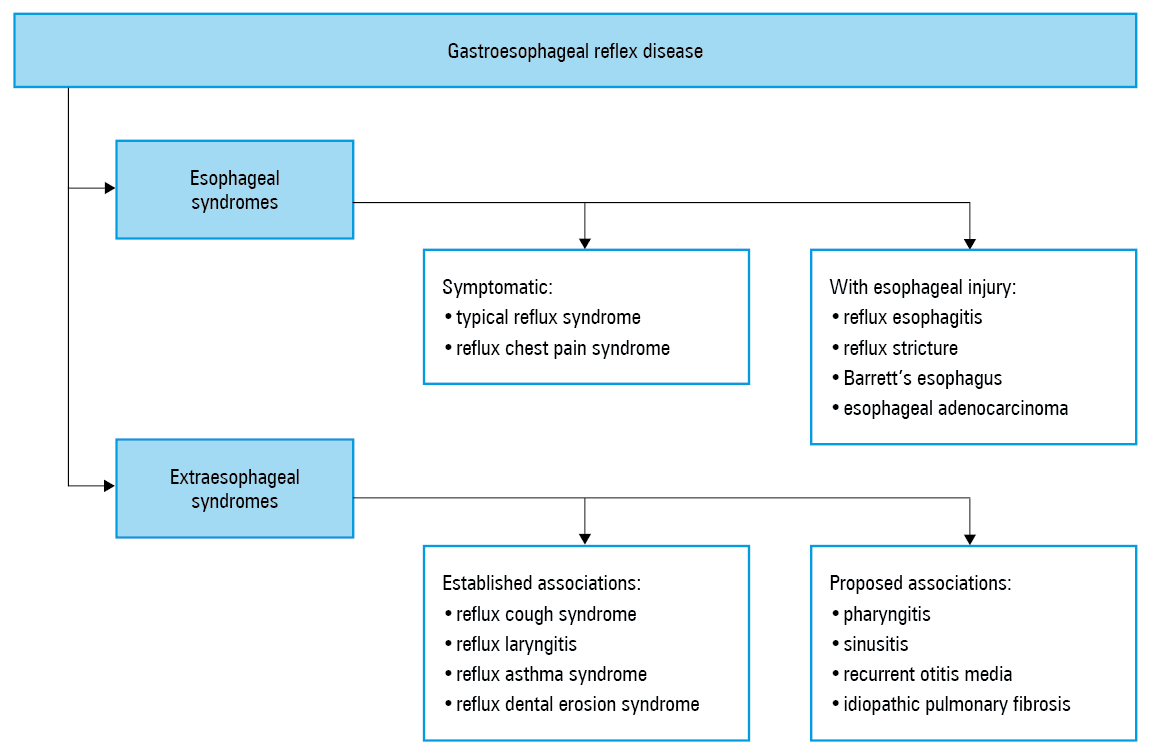
The Montreal Consensus distinguishes between esophageal and extraesophageal GERD syndromes (Figure 1). Esophageal syndromes were divided into symptomatic syndromes and syndromes with esophageal injury. Symptomatic esophageal syndromes include a typical reflux syndrome with troublesome heartburn and / or regurgitation. Abdominal pain and sleep disturbances may also be present in this syndrome. In a reflux chest pain syndrome, the pain is the only or predominant symptom of the disease. Esophageal syndromes with injury include: reflux esophagitis, reflux esophageal stricture, BE, and esophageal adenocarcinoma. In the group of extraesophageal syndromes, syndromes with a documented association with reflux were distinguished, including reflux cough syndrome, reflux laryngitis syndrome, reflux asthma syndrome, and reflux dental erosion syndrome, as well as syndromes with a not fully confirmed relationship with GERD, such as pharyngitis, sinusitis, recurrent otitis media, and idiopathic pulmonary fibrosis.9 More than a dozen years have passed since the publication of the Montreal definition. Studies published within this time frame confirmed a causal relationship between GERD and reflux cough syndrome and dental erosions. However, there is no clear evidence of a causal relationship between GERD and laryngitis and asthma. The association of GERD with pharyngitis, sinusitis, otitis media, and idiopathic pulmonary fibrosis has not been established. The division of GERD into esophageal and extraesophageal syndromes determines further diagnostic and therapeutic management in GERD and is discussed below.
GERD diagnosis
Although several methods are available to facilitate GERD diagnosis, it is debatable whether there is a so‑called gold standard. The recently published Lyon Consensus suggests that intra‑esophageal impedance and pH monitoring may be considered the gold standard in the detection and characterization of reflux episodes.37 Depending on the clinical situation, each of the methods discussed below may be helpful, if implemented and interpreted correctly. It is also crucial to understand the limitations of each method (Tables 3 and 4).
Diagnostic test | Indications |
Abbreviations: GERD, gastroesophageal reflux disease | |
Upper gastrointestinal endoscopy |
|
Ambulatory monitoring of intraesophageal pH or pH and impedance |
|
Esophageal manometry |
|
Laryngoscopy, pharyngeal pH monitoring | No indications in clinical practice |
Method | Benefits | Limitation |
Abbreviations: LES, lower esophageal sphincter; MNBI, mean nocturnal baseline impedance; PPI, proton pump inhibitor; PSPW, postreflux swallow‑induced peristaltic wave; SAP, symptom association probability; SI, symptom index; others, see Table 3 | ||
GERD questionnaire | Easy in use | Inability to distinguish nonerosive GERD from hypersensitive esophagus and functional heartburn |
PPI inhibitor trial | Rapid test for use in general practicioner’s care for patients with no alarm symptoms | Positive in 69% of patients with erosive GERD, 49% of patients with nonerosive GERD, and 35% of patients with no changes in endoscopy and normal esophageal pH.
Sensitivity 71% and specificity 44% among patients reporting heartburn. Lower response in patients reporting atypical symptoms.
A negative test result does not rule out GERD. |
Upper gastrointestinal endoscopy | Recognition of GERD complications and other causes of symptoms | About 70% of patients have a normal endoscopy.
Grade A esophagitis according to the Los Angeles classification is found in 5%–7.5% of healthy people.
Differences in endoscopists’ assessment of low‑grade inflammation in the Los Angeles Classification. |
Biopsy | Diagnosis of inflammatory changes in the esophagus and exclusion of eosinophilic esophagitis | 15% of healthy people have changes on histological examination, 20% of patients with GERD have no changes. |
Ambulatory esophageal pH monitoring | Easy to perform, accessible, relatively noninvasive, detection of exposure to acid in the esophagus, automatic analysis | Discomfort from transnasal probe placement (impact on daily activity).
Diurnal variability of the occurrence of reflux and symptoms.
LES localization required for probe placement.
Study specificity lower than 71% in patients with normal endoscopy. |
Ambulatory intraesophageal pH and impedance monitoring | Easy to perform, limited availability, relatively noninvasive, detection of esophageal acid exposure, automatic analysis
It enables the assessment of nonacid reflux.
The best method in the differential diagnosis of patients with GERD and functional heartburn and in patients with refractory GERD.
Helpful in the diagnosis of belching and rumination disorders. | Discomfort from transnasal probe placement (impact on daily activity).
Diurnal variability of the occurrence of reflux and symptoms.
LES localization required for probe placement.
The clinical significance of nonacid reflux is uncertain.
Automatic analysis requires manual adjustment.
Limitation of SI and SAP indexes assessment.
Clinical significance of the new parameters: MNBI and PSPW not specified and time‑consuming “manual” evaluation. |
Diagnosis of GERD based on symptoms
STATEMENT 3. The assessment of clinical symptoms is the first step in the diagnostic and therapeutic management of GERD (C / I‑80%, II‑20%).
STATEMENT 4. GERD diagnosis can be made on the basis of the presence of troublesome heartburn and / or regurgitation (typical symptoms) (B / I‑80%, II‑10%, III‑10%).
STATEMENT 5. Sensitivity and specificity of atypical symptoms in GERD diagnosis are lower than of typical symptoms. The etiology of extraesophageal symptoms is multifactorial, and GERD probability is low in the absence of typical symptoms (B / I‑70%, II‑20%, III‑10%).
STATEMENT 6. The presence of alarm symptoms requires imaging studies to be performed in order to exclude an organic disease (B / I‑90%, II‑10%).
According to the Montreal Consensus, the presence of troublesome typical symptoms, that is, heartburn and/or regurgitation is sufficient to diagnose GERD and initiate empirical treatment.9,17 Unfortunately, as compared with objective diagnostic methods (pH‑metry and endoscopy), the sensitivity and specificity of typical reflux symptoms are suboptimal.17,37-39 In comparison with typical symptoms, sensitivity and specificity of atypical symptoms in GERD diagnosis are lower.
Heartburn and regurgitation have a sensitivity of about 30%–76%, and a specificity of 62%–96%, with the specificity of acid regurgitation being greater than that of heartburn.40-42 Other causes of heartburn can be functional disorders (so‑called functional heartburn), eosinophilic esophagitis or esophageal motility disorders. On the other hand, not all GERD patients report heartburn. It was suggested that up to 50% of patients with severe esophagitis remain asymptomatic.43 Similar limitations apply to the usefulness of questionnaires in GERD diagnosis.37 It should also be noted that the typical symptoms are not characteristic of GERD only. They can also occur in other diseases, including gastric and duodenal ulcer disease, gastritis and duodenitis, and gastric cancer. This means that each case suggesting an initial GERD diagnosis requires an individual diagnostic and therapeutic approach.
Chest pain may coexist with other symptoms or be the only symptom of GERD, but it should be remembered that its most common cause is cardiovascular disease.9,17 GERD may be responsible for approximately 21%–41% of cases of unexplained chronic cough.44 The 2016 guidelines for the management of chronic cough listed a set of features suggesting that chronic cough (lasting for more than 8 weeks) may be related to GERD. These include: no exposure to smoking and other environmental pollutants, not taking angiotensin converting enzyme inhibitors, normal chest X‑ray results, and excluded asthma, sinus and bronchial diseases.45 Only half of the patients with extraesophageal symptoms simultaneously report typical GERD symptoms. The likelihood of extraesophageal symptoms association with GERD is low in the absence of typical symptoms. Therefore, a multifactorial etiology of extraesophageal symptoms should be kept in mind. GERD may contribute to the pathogenesis of these symptoms only in some patients. It is estimated that only 4%–10% of the symptoms reported by patients who visit laryngologists due to hoarseness, excessive mucus production, sore throat or foreign body sensation are caused by GERD.9,17,46
GERD patients may report a number of other atypical symptoms, such as nausea, belching, and dyspepsia. These symptoms may also result from the coexistence of other diseases, that is, functional dyspepsia or irritable bowel syndrome.9,17 In addition, these symptoms can be reported by patients with a number of other conditions including diseases of the stomach, duodenum, gallbladder, pancreas, and intestines. Dysphagia may be reported by patients with esophagitis (approximately 37%) and BE, but it may be a symptom of a post‑inflammatory or neoplastic esophageal stricture, the presence of the Schatzki ring or eosinophilic esophagitis, and may also be a consequence of esophageal motility disorders.9,17,47
The presence of alarm symptoms requires imaging diagnostic studies before starting the treatment, in order to exclude GERD complications and other possible causes of symptoms, including neoplastic disease. The alarm symptoms include: weight loss, dysphagia, abdominal pain at night (waking the patient up from sleep), persistent vomiting, symptoms of gastrointestinal bleeding, and anemia.17,37,48
Proton pump inhibitor test
STATEMENT 7. The 14‑day proton pump inhibitor test should not be used routinely for GERD diagnosis (B / I‑50%, II‑50%)
Attempting treatment with a PPI at a standard dose twice a day for 14 days should not be used routinely as a method of GERD diagnosis.37,49 Symptom relief with the PPI is reported by an average of 69% of patients with reflux esophagitis, 49% of patients with GERD with a normal endoscopy, and 35% of patients with normal endoscopy and pH‑metry.50 Among patients reporting heartburn, the PPI test has a sensitivity of about 71%–78% and a specificity of 44%–54%, when compared to a combination of endoscopy and pH‑metry.37,51-53 In the case of atypical symptoms, as mentioned earlier, the response to PPI treatment is lower, which further reduces the usefulness of this test in GERD diagnosis.37,53 The limitations of this test include: a significant role of visceral hypersensitivity in symptom modulation, differences in drug doses, and various duration of the test.37,54-56 The widespread use of the PPI test leads to over‑diagnosis of GERD and PPI abuse.37
Endoscopy
STATEMENT 8. It is not necessary to perform upper gastrointestinal endoscopy (EGD), if only typical symptoms are present (B / I‑60%, II‑30%, III‑10%).
STATEMENT 9. EGD is necessary in patients reporting alarm symptoms (B / I‑90%, II‑10%)
EGD is not required when typical symptoms of GERD are present. The indication for EGD is a lack of a response to empirical PPI treatment. The procedure is then used to assess not only possible GERD complications but also to exclude other causes of the symptoms. It should be remembered that treatment should not delay examination of the upper gastrointestinal tract in the presence of alarm symptoms (weight loss, dysphagia, abdominal pain waking the patient up from sleep, persistent vomiting, symptoms of gastrointestinal bleeding, anemia); this diagnostic procedure should be performed immediately.17,48
EGD confirms the presence of disease complications such as erosions in the esophagus – erosive form of GERD (reflux esophagitis), esophageal postinflammatory stricture, or BE.48,57 Normal endoscopy results do not exclude GERD. Esophageal erosions are found only in approximately 30%–40% of patients with heartburn not receiving acid suppression therapy, and in less than 10% of patients receiving PPIs.58,59 The severity of reflux esophagitis is assessed using the Los Angeles (LA) classification (Table 5). It should be kept in mind that low grade esophagitis, that is, grade A according to the LA classification, is not specific for GERD and occurs in 5%–7.5% of asymptomatic individuals.60-62 In addition, there are difficulties in its endoscopic recognition and some authors suggest that there may also be intraobserver variations in endoscopic assessment of not only grade A but also grade B esophagitis. For this reason, some experts believe that the presence erosive esophagitis of at least grade B indicates GERD.37 The American College of Gastroenterology (ACG) guidelines from 2013 recommend broader GERD diagnostics in the presence of grade A esophagitis.17
Grade | Characteristics of changes |
A | At least 1 mucosal break no longer than 5 mm |
B | At least 1 mucosal break longer than 5 mm that does not extend between the tops of two mucosal folds |
C | At least 1 mucosal break that extends between the tops of 2 or more mucosal folds, but which involves less than 75% of the esophageal circumference |
D | Mucosal breaks which involve at least 75% of the esophagus circumference |
STATEMENT 10. Routine EGD in all patients with symptomatic GERD is not recommended as a screening test for Barrett’s esophagus. However, this examination should be performed in patients with multiple (≥ 3) risk factors: GERD duration above 5 years, age 50 or above, white race, male gender, obesity, BE, and / or grade 1 relative with esophageal adenocarcinoma (B / I‑80%, II‑20%)
BE occurs in approximately 5%–15% of patients with long‑term GERD.63-65 There is no high‑quality scientific evidence to support screening for BE. However, it seems that BE diagnosis prior to the diagnosis of esophageal adenocarcinoma is associated with better survival.66 Most of the published guidelines recommend or allow screening in patients with multiple risk factors, the most important of which seems to be a long duration of GERD.67-71
STATEMENT 11. Barrett’s esophagus is diagnosed by the presence of glandular epithelium covering at least 1 cm of the distal part of the esophagus, with histopathological evidence of intestinal metaplasia (B / I‑80%, II‑10%, III‑10%).
Due to the adoption of such a definition, neither random biopsy from metaplastic segments more than 1 cm long, nor long‑term surveillance in these cases are recommended.70,71 However, in such a situation, targeted biopsies should be performed, if macroscopically visible lesions are found. The 1 cm border was adopted due to a low degree of agreement in BE diagnosis in the case of segments more than 1 cm long and a low risk of progression to cancer.72-74 Most scientific societies do not recognize the presence of gastric metaplasia in the esophagus as a basis for BE diagnosis.
STATEMENT 12. Lesions suggesting Barrett’s esophagus in endoscopy should be assessed according to the Prague C&M Criteria (specifying the length of the circumferential segment and total length of the metaplastic segment). If focal changes are found, their exact location, size, and macroscopic appearance according to the Paris classification should be provided. Additionally, the presence or absence of inflammatory changes should be described (C / I‑90%, II‑10%).
STATEMENT 13. If endoscopy suggests Barrett’s esophagus, specimens should be taken for histopathological examination according to the following scheme:
-
Random sections from 4 quadrants of the metaplastic segment (1 set of sections for every 2 cm of the segment, counting from the upper border of the gastric folds).
-
Targeted sections from the identified macroscopic lesions (B / I‑100%) There is common acceptance for the BE assessment according to the Prague C&M Criteria, and focal changes according to the Paris classification.75-77 It is widely recognized that a biopsy in BE is taken according to the Seattle Protocol, and targeted biopsies should be performed for focal lesions.78-80
STATEMENT 14. In patients with (LA) grade C and D reflux esophagitis, and in doubtful B grade, follow‑up EGD should be performed after 8 weeks of PPI therapy to exclude Barrett’s esophagus (B / I‑60%, II‑40%).
STATEMENT 15. Biopsy specimens should not be taken for histopathological examination to diagnose Barrett’s esophagus and during surveillance EGD in the presence of active inflammatory lesions (reflux esophagitis) (B / I‑100%)
BE often coexists with reflux esophagitis. This brings about two important implications. First, inflammatory changes may mask the presence of the metaplastic segment, especially with high intensity inflammatory changes (LA grades C and D and, in doubtful cases, grade B), and a short lingual segment of BE.81,82 Secondly, due to difficulties in distinguishing between dysplasia and regenerative changes, biopsy specimens should not be taken for histopathological examination in the presence of inflammatory changes, in order to avoid a false positive diagnosis of dysplasia.70,83-85
STATEMENT 16. The diagnosis of any degree of dysplasia (including indeterminate dysplasia) requires confirmation by a second pathologist, preferably an expert in the field of gastrointestinal pathology (B / I‑90%, II‑10%)
The diagnosis of dysplasia in BE is difficult, and the degree of agreement among pathologists is low.86-88 Low‑grade dysplasia seems to be overly diagnosed mainly because it is difficult to distinguish from regenerative changes.83 More than 4 out of 5 diagnoses of low‑grade dysplasia may not be confirmed by experts in the pathology of BE. On the other hand, if the diagnosis is confirmed (the presence or absence of dysplasia) by a second pathologist, its diagnostic effectiveness increases significantly.69,84,89,90
STATEMENT 17. Long‑term endoscopic surveillance is recommended in patients with Barrett’s esophagus (B / I‑70%, II‑30%).
STATEMENT 18. Patients diagnosed with dysplasia and a very long metaplastic segment (≥ 10 cm) should be monitored or treated in a center specialized in the management of Barrett’s esophagus (C / I‑60%, II‑40%).
STATEMENT 19. Surveillance may be discontinued in patients without dysplasia who were over 75‑80 years of age at the time of the last surveillance EGD (C / I‑70%, II‑30%)
Long‑term endoscopic surveillance in BE leads to the diagnosis of esophageal adenocarcinoma at earlier stages and, consequently, to improved survival of patients with adenocarcinoma.66,91,92 In order to ensure the highest level of quality of management in BE, the American Gastroenterological Association and the European Society of Gastrointestinal Endoscopy (ESGE) proposed that diagnostics and supervision in the case of dysplasia as well as BE treatment should be carried out in expert centers with sufficient clinical experience and appropriate training, personnel, and equipment.71,85 For metaplastic segments 10 or more centimeters long, the risk of progression to cancer may be comparable to BE with dysplasia. Therefore, such a cut‑off point was arbitrarily established for referral to an expert center.71 The proposed time to discontinue surveillance was also determined arbitrarily, based on life expectancy.93
STATEMENT 20. Time intervals of EGD surveillance in Barrett’s esophagus without dysplasia should depend on the overall length of the metaplastic segment:• from 1 to below 3 cm (short segment) ‑ every 5 years • from 3 to below 10 cm (long segment) ‑ every 3 years (C / I‑60%, II‑40%)
The risk of progression to adenocarcinoma increases with the length of the metaplastic segment.73 These time intervals were arbitrarily proposed by the ESGE for the European population.71 The prerequisite for such intervals is high‑quality EGD surveillance, that is, examination by an appropriately trained physician, high‑resolution equipment, and biopsy collection in accordance with the Seattle protocol.
STATEMENT 21. In patients diagnosed with dysplasia not specified in a random biopsy, a follow‑up EGD should be performed after 6 months. If this examination does not reveal dysplasia, then surveillance should be continued as in Barrett’s esophagus without dysplasia (B / I‑70%, II‑30%).
STATEMENT 22. In patients diagnosed with la ow‑grade dysplasia in a random biopsy, a follow‑up EGD should be performed after 6 months. If this examination does not confirm dysplasia, another examination should be performed after 12 months. If no dysplasia is found in this examination, then surveillance should be continued as in Barrett’s esophagus without dysplasia (B / I‑70%, II‑30%)
Even if the diagnosis of dysplasia is confirmed by an another histopathologist, about 30% of patients experience regression of dysplastic changes. On the other hand, confirmation of the diagnosis of dysplasia at the next time point significantly increases the risk of progression to cancer.84,90,94
Biopsy for GERD diagnosis
STATEMENT 23. Routine distal esophageal biopsy for GERD diagnosis is not recommended (B / I‑70%, II‑30%)
Comments in Supplementary material, Part 2.1. See appropriate references.17,37,59,95-102
Ambulatory reflux monitoring
STATEMENT 24. Ambulatory 24‑hour intraesophageal monitoring of pH and impedance or pH only should be considered in patients reporting atypical GERD symptoms, in patients with refractory GERD, and in patients qualified for antireflux surgery (C / I‑80%, II‑20%).
STATEMENT 25. In patients with a high probability of GERD as the cause of symptoms (abnormal endoscopy or pathological reflux in pH or pH and impedance monitoring test), reflux monitoring (preferably pH and impedance) should be performed on PPI therapy (B / I‑80%, II‑20%).
STATEMENT 26. In patients with a low probability of GERD (normal endoscopy, atypical / extraesophageal symptoms), monitoring of pH and impedance, or possibly only pH, is best performed off PPI therapy in order to confirm or rule out GERD (B / I‑90%, II‑10%).
STATEMENT 27. The parameters of reflux monitoring that best support GERD include: abnormal acid exposure in the esophagus (AET >6), abnormal reflux number (>80), and a positive correlation of symptoms with reflux (symptom association probability [SAP] and symptom index [SI]) (C / I‑70%, II‑30%).
Ambulatory reflux monitoring is possible through the use of 24 h pH measurement (pH‑metry) or multichannel intraesophageal pH and impedance monitoring. There is no need for ambulatory reflux monitoring in patients responding to PPI treatment and not qualified for antireflux surgery.103 Currently, monitoring is performed mainly to exclude or confirm GERD in patients with normal upper GI endoscopy, reporting atypical symptoms, in patients with persistent symptoms despite PPI therapy (refractory GERD), and in patients who are considering antireflux surgery.17,37-39,49,54,95
Monitoring of pH or pH and impedance determines the pathophysiological basis of GERD, that is, excessive esophageal acid exposure and reflux episodes, and assesses the relationship between the reported symptoms and reflux. As compared with pH‑metry alone, pH and impedance monitoring detects not only acid reflux but also nonacid reflux and assesses its correlation with the symptoms reported by the patient. Monitoring of pH and impedance is therefore advantageous in the assessment of patients receiving PPI treatment, and is considered a gold standard in GERD diagnosis. However, one should take into account the still limited availability of this test in Poland, as compared with classic pH‑metry. The assessment of esophageal acid exposure time (AET) remains the most reproducible parameter and a predictor of response to antireflux therapy, both pharmacological and surgical.37,104,105 Currently, it is proposed to consider AET below 4% as normal (physiological) and AET above 6% as abnormal. For AET in the 4‑6 range (considered inconclusive), a detailed evaluation of other parameters, including the number of refluxes, is required. A total number of reflux episodes below 40 per day is considered physiological, more than 80 episodes – completely abnormal, and values in between are viewed as intermediate (inconclusive).37,57 The clinical relevance of the number of reflux episodes remains unknown. An important advantage of reflux monitoring is the assessment of a correlation between the patient’s symptoms and reflux by the use of indexes, most often SI, and the index determining the probability of a symptom‑reflux correlation, SAP. SI index, assessing the percentage of symptoms preceded by reflux, is considered positive when it exceeds 50%. SAP index is more mathematically complicated and it takes into account the number of reflux episodes, symptom events, and reflux–related symptoms. SAP result above 95% is positive, which means that the probability of a random symptom‑reflux correlation is lower than 5%.37-39,57,93,106-108 Although SAP index appears to be more reproducible than SI, clinical practice shows that the best assessment of reflux‑symptom correlation is obtained by analyzing both indexes, which are predictors of response to PPI or surgical treatment regardless of AET value.37,38,95,109,110 It should be mentioned that the assessment of the symptom‑reflux correlation is difficult, especially with a small number of symptoms (more reliable with at least 3 episodes of symptoms) and low acid exposure, and it depends on the correctness of the patient’s reporting of symptoms. Moreover, in the cases of some atypical symptoms, the assessment of indexes may be significantly difficult (eg, the accuracy and reliability of cough analysis may require acoustic detection) or impossible (eg, chronic laryngitis).37-39,57,95 Symptoms are more likely to occur without PPI treatment, so pH and impedance monitoring off PPI therapy increases the likelihood of a positive symptom‑reflux correlation.111 Monitoring of pH and impedance allows for the assessment of nonacid (weakly acidic) reflux and the correlation of these reflux episodes with symptoms. However, the importance of such a correlation is not fully understood. Automatic analysis requires manual verification, as it overestimates the number of nonacid reflux events and may misjudge their association with symptoms.112
In the diagnosis of GERD, the importance of additional parameters including: bolus exposure, baseline impedance, mean nocturnal baseline impedance (MNBI) and postreflux swallow‑induced peristaltic wave (PSPW) are not well understood due to a small number of studies. It was shown that MNBI and PSPW can be particularly helpful in the differential diagnosis of GERD and functional heartburn.37,57
Currently, it is recommended that monitoring of pH and impedance or pH only is performed off PPI therapy to determine baseline AET in patients with no prior GERD confirmation or low probability thereof, for example, patients with normal EGD, who did not have a previous pH‑metry and report atypical symptoms. This differentiates patients with GERD from those with hypersensitive esophagus or functional heartburn. In the impedance and pH monitoring, a hypersensitive esophagus is diagnosed when there is a normal number of reflux and AET events but symptoms are correlated with reflux. In a patient complaining of heartburn with a normal test result and lack of symptom‑reflux correlation, the diagnosis is a functional heartburn. It is also recommended to monitoring the PPI therapy in the patients qualified for antireflux surgery.17,37-39,57,95,113 It was demonstrated that an abnormal 24 h pH‑metry is a predictor of symptom improvement after antireflux surgery.114 On the other hand, patients with typical symptoms and a normal endoscopy are less likely to respond to the surgery.114 The Lyon consensus recommends that pH or pH and impedance monitoring are performed prior to the antireflux surgery, especially in patients with normal EGD or LA grade A and B esophagitis.37 When measuring pH and intraesophageal impedance, or pH alone in patients with low probability of GERD, one should also remember to discontinue drugs blocking histamine H2 receptor.
Monitoring of pH and impedance during PPI therapy (at a standard dose, twice a day) is recommended in patients with documented GERD, that is, positive pH or pH and impedance monitoring, or GERD complications in EGD (reflux esophagitis, especially LA grade C or D, esophageal stricture, BE), to assess the correlation of persistent symptoms with reflux episodes despite therapy and / or determine their cause, for example insufficient acid suppression, poor compliance / adherence.37
Recent guidelines of the British Society of Gastroenterology (BSG, 2019) favor the use of pH and impedance monitoring for primary evaluation of patients with refractory PPI, chest pain, or laryngological / pulmonary symptoms. In patients qualified for anti‑reflux surgery, but responding to PPI treatment, BSG recommends pH‑metry. On the other hand, pH and impedance monitoring enables a more accurate assessment of patients with GERD refractory to PPI therapy and qualified for surgery. Moreover, BSG prefers to perform pH and impedance monitoring over pH‑metry in patients with recurrent or persistent symptoms after surgery.103 BSG guidelines also recommend pH and impedance monitoring in patients with idiopathic pulmonary fibrosis, cystic fibrosis or other lung diseases qualified for lung transplantation in whom GERD is suspected.103
In comparison with other diagnostic methods, ambulatory monitoring of pH or pH and impedance is more accurate in the assessment of reflux, however, it does not always allow for the exclusion or confirmation of GERD. The sensitivity and specificity of pH monitoring is high (80‑100%) in patients with reflux esophagitis, while in patients with normal endoscopy it is lower.17 Factors that may affect the procedure, its results, and interpretation of the test include: discomfort resulting from the presence of a transnasal probe, limitation of physical activity and altered meals, and daily variability in the occurrence of symptoms and reflux episodes. Tables 3 and 4 list a number of other limitations of the testing methods discussed above that should be considered during data interpretation.
Other methods of reflux monitoring
STATEMENT 28. Pharyngeal pH monitoring is not recommended in GERD diagnostics (C / I‑90%, II‑10%).
STATEMENT 29. Routine evaluation of duodeno‑gastro‑esophageal reflux is not recommended in GERD diagnostics (C / I‑90%, II‑10%)
Comments in Supplementary material, Part 2.2. See appropriate references.17,35,37,39,95,115-117
Manometry
STATEMENT 30. Esophageal manometry is not recommended for GERD diagnostics (C / I‑90%, II‑10%).
STATEMENT 31. Esophageal manometry should be performed in GERD patients qualified for anti‑reflux surgery (C / I‑90%, II‑10%)
Comments in Supplementary material, Part 2.3. See appropriate references.17,37,103,118-121
Radiographic examination of the esophagus with contrast
STATEMENT 32. Contrast‑enhanced radiography of the esophagus should not be performed in GERD diagnostics (B / I‑80%, II‑20%)
Comments in Supplementary material, Part 2.4. See appropriate references.17,39,95,122,123
Laryngoscopy
STATEMENT 33. Diagnosis of reflux laryngitis syndrome as extraesophageal GERD should not be based on the results of laryngoscopy (B / I‑100%)
Comments in Supplementary material, Part 2.5. See appropriate references.17,37,95,124-129
GERD treatment
STATEMENT 34. In the treatment of GERD, lifestyle modifications are recommended, including: weight reduction in overweight and obese patients, head of bed elevation during sleep and avoiding meals at least 3 hours before bedtime (B / I‑60%, II‑40%).
STATEMENT 35. PPIs are currently the most effective class of drugs in relieving GERD symptoms and healing inflammatory lesions of the esophagus (A / I‑80%, II‑20%).
STATEMENT 36. PPIs are a safe group of drugs, the use of which is associated with a small percentage of side effects (A / I‑90%, II‑10%).
STATEMENT 37. Histamine 2 receptor antagonists can be used to control symptoms in patients with GERD and normal endoscopy, as an add‑on therapy (especially at night) in the case of insufficient PPI effectiveness, and as a treatment in gradually reduced doses (“step‑down”) after obtaining symptom remission with PPI (B / I‑90%, II‑10%).
STATEMENT 38. Antacids and / or topical mucosal preparations can be used on demand to relieve intermittent GERD symptoms, or as add‑on therapy to acid suppression therapy (PPI or PPI and histamine 2 receptor antagonists) for better symptom control (B / I‑100%).
STATEMENT 39. The routine use of prokinetic drugs is not recommended (B / I‑60%, II‑30%, III‑10%).
STATEMENT 40. Surgical treatment can be an effective method of GERD treatment in a carefully selected group of patients. Fundoplication can be performed in patients with pathological reflux confirmed by pH or pH and impedance monitoring (off PPI therapy), who responded to PPI therapy but do not want to take PPIs chronically; or when there are side effects of PPI therapy; or when symptoms (regurgitation) persist despite PPI therapy in a patient with a known mechanical defect of the antireflux barrier (eg, hiatal hernia) (B / I‑60%, II‑40%).
STATEMENT 41. Surgical treatment is not recommended in patients with extraesophageal GERD symptoms, especially isolated and unresponsive to PPI therapy. It can only be considered in patients with objectively confirmed GERD that is refractory to pharmacological treatment (B / I‑100%).
General recommendations
A majority of physicians advise GERD patients to modify their lifestyle. There is insufficient evidence to routinely recommend smoking cessation, alcohol abstinence, avoiding chocolate, caffeine and coffee, mint, citrus, hot spices, and soda.17,130 However, individual patients may benefit from excluding certain foods from their diet. Other interventions that may be helpful include: reducing meal volumes, avoiding vigorous exercise, torso bends, wearing looser clothes around the waist, avoiding the lying position immediately after a meal and lying on the right side, avoiding certain medications (methylxanthines, nitrates, calcium channel blockers, tricyclic antidepressants, estrogens).131
Weight gain was shown to increase the risk of GERD symptoms and complications, while weight loss was confirmed to reduce GERD symptoms.10,17,31,33-36,132 In all patients with BMI over 25 or patients with weight gain (even within normal BMI range), it is recommended to reduce body weight.17 Regular, moderate exercise, including aerobic exercise, can be helpful in GERD treatment. In populational studies, lower GERD prevalence was observed in patients who regularly exercised. Regular exercise strengthens the diaphragm’s striated muscles.133 Randomized trials demonstrated the benefit of head of bed elevation during sleep resulting in symptom reduction and lower AET, especially in patients with confirmed nocturnal reflux.17,134,135 It is also recommended to avoid taking a meal at least 3 h before going to bed.17
Pharmacological treatment
PPIs are currently the most effective class of drugs in relieving GERD symptoms and healing inflammatory esophageal changes. PPIs heal reflux esophagitis in 72%–83% of patients and relieve heartburn in 56%–77% of patients with esophagitis.37 The risk of recurrence of inflammatory changes in the esophagus in patients continuing PPI therapy is 13%, and the risk in patients who discontinue the therapy is 72%, and it is the highest in LA grade C and D esophagitis.136,137
PPIs are more effective in maintaining remission after healing esophagitis than histamine H2 receptor antagonists (91% vs 62%).137 The available data on PPIs used in the prevention of esophageal adenocarcinoma in patients with BE are contradictory, although a significant number of studies indicate that such a therapy brings about desired outcomes.67,69,136,138-140 In a recently published study, the analyzed end parameters, that is, mortality, incidence of high‑grade dysplasia and esophageal adenocarcinoma in patients with BE, were more favorable in a group of patients receiving high‑dose PPIs (esomeprazole 40 mg twice daily) than in a group receiving low‑dose PPIs (20 mg once daily) for over 8 years (139 cases of the above‑mentioned end events in 1270 patients taking high‑dose PPIs vs 174 events in 1265 patients taking low‑dose PPIs (time ratio [TR], 1.27; 95% CI, 1.01–1.58; P = 0.038). Moreover, a beneficial chemopreventive effect was demonstrated after the addition of acetylsalicylic acid.141 The results of this study require confirmation before implementing its treatment regimens in routine clinical practice. Long‑term effects of prolonged PPI therapy are still the subject of research and numerous controversies. Treatment with a standard PPI dose is effective in 37%–61% of patients with undiagnosed heartburn and normal endoscopy (note that this group includes patients without GERD and functional heartburn).51 Improvement with PPI therapy is experienced by 26%–64% of patients reporting regurgitation. In the case of extraesophageal symptoms, especially in the absence of the typical reflux symptoms, the response to treatment is low. In one study, the effectiveness of PPI did not exceed general recommendations that included a Mediterranean diet and consumption of water with pH above 8.142 A recently published meta‑analysis showed that the effectiveness of PPIs, defined as a 50% reduction in laryngological symptoms, was comparable to placebo (42% and 39%, respectively). There were also no differences in the changes on laryngoscopy.143 A response to PPI therapy is much weaker in patients with a hypersensitive esophagus and almost does not exist in patients with functional heartburn. In summary, the best candidates for PPI therapy are patients with reflux esophagitis or patients with normal endoscopy and GERD confirmed by testing (pH or pH and impedance monitoring).37
PPIs do not affect the pathophysiological mechanism of reflux or the number of refluxes, and by blocking the proton pumps they only inhibit the secretion of hydrochloric acid in the stomach. The guidelines of the National Institute for Health and Care Excellence recommend the following as standard equivalent doses: omeprazole 20 mg, esomeprazole 20 mg, lansoprazole 30 mg, rabeprazole 20 mg, and pantoprazole 40 mg.144 To optimize the effectiveness of PPIs, they should be administered 30‑60 minutes before a meal. Making sure that the drug is properly taken (appropriate dose, timing, no skipped doses) should be the first step in assessing treatment efficacy, especially in patients without improvement. Expert opinions suggest there are no major differences in the effectiveness of various PPIs mentioned above, for example, in the percentage of esophagitis cures after 8 weeks of therapy.17,37 A newer PPI, dexlansoprazole, can be taken with or without food as it consists of two types of microgranules released in the stomach and small intestine, resulting in two effect peaks (1‑2 h and 4‑5 h) (Table 6).
Medication | Dose | Comments | |
Abbreviations: see Table 3 | |||
Antacids, alginates, chondroitin sulfate with hyaluronic acid | Several times a day, after meals | Recommended on an ad hoc basis, can be added at any stage of the treatment. | |
Histamine 2 receptor antagonists | Ranitidine | 150 mg twice a day, once a night | Possible tachyphylaxis |
Famotidine | 20 mg twice a day, once a night | Taken in the evening for nocturnal symptoms | |
Proton pump inhibitors | Omeprazole | 20 mg 1–2 times a day | 30–60 min before a meal |
Esomeprazole | 20 mg 1–2 times a day | ||
Rabeprazole | 20 mg 1–2 times a day | ||
Lansoprazole | 30 mg 1–2 times a day | ||
Pantoprazole | 40 mg 1–2 times a day | ||
Dexlansoprazole | 30 mg, 60 mg | Independently of the meal | |
Baclofen | 5 mg 3 times a day (after 7 days 10 mg 3 times a day, after 1 month effectiveness assessment, or a dose of 20 mg 3 times a day) | Not registered for GERD treatment; central side effects | |
Itopride | 50 mg 3 times a day for 8 weeks (followed by evaluation of its efficacy) | It can be helpful in patients with dyspeptic symptoms. | |
Amitriptyline | 25–50 mg once a day at night | Beneficial for sleep / anxiety disorders, helpful for chest pain | |
Citalopram/Fluoxetine | 20 mg once a day | ||
Side effects of PPI therapy are reported by a small group of patients (<5%, similar to placebo), and the most common ones include: diarrhea, headache, nausea and vomiting, and excessive gas emission. There are still concerns about undesirable consequences resulting from long‑term PPI use. Although available literature postulates a relationship between PPI intake and a number of disease entities and complications, it should be remembered that most studies were epidemiological, retrospective, observational, and the timing of PPI use or the temporal relationship between PPIs and the occurrence of the adverse event was difficult to determine.136 Generally, PPIs are considered a safe class of drugs. Significant side effects include dysbiosis of the intestinal microbiota, which predisposes to an increase in the incidence of Clostridioides difficile (OR, 1.26), and small intestinal bacterial overgrowth syndrome, as well as malabsorption and deficiency of vitamin B12 (OR, 1.83), magnesium, and iron.136,145 Considering the long time of the therapy and potential side effects, PPIs should be used at the lowest effective dose and for the shortest time possible.
In most patients, the symptoms and inflammatory esophageal changes disappear after 8‑12 weeks of therapy. Maintenance treatment is required in patients with GERD complications. Maintenance treatment for symptomatic GERD should be carried out at the lowest effective dose. On‑demand or intermittent therapy may be considered in patients with NERD, LA grade A or B esophagitis, in young patients without comorbidities, in whom factors aggravating reflux were eliminated.17,30,37,49,53,136,144,146 One study showed that in as many as 80% of patients with well‑controlled symptoms on high‑dose PPIs, treatment could be reduced to a standard dose without significantly worsening the symptoms.147 Some patients do not want to discontinue PPIs, fearing recurrence of the symptoms. In another study, PPI therapy was administered for 8 weeks in patients without GERD and dyspepsia, followed by placebo or PPI for 4 weeks. In the subgroup of patients who discontinued PPIs, 40% reported dyspeptic symptoms.148 A one more paper reported that 2/3 of the patients who discontinued PPIs (due to a lack of indications for their use) developed upper gastrointestinal symptoms within 6 months; 40% of them even had slight inflammatory changes in the esophagus.149 The symptoms occurring after PPI discontinuation were shown to correlate with hypergastrinemia.150 Gradual PPI withdrawal reduces the risk of their onset (eg, half dose for 2 weeks, then discontinue; alternatively use every second day for 2 weeks, then twice a week for another 2 weeks, and then discontinue).136 During a 12‑month follow‑up, 60% of patients did not require any treatment after gradual PPI withdrawal (half of the standard dose for 2 weeks, then discontinuation).151 Some researchers advise patients not to take PPIs (especially in the first week after discontinuation) as soon as the first signs of recurrence of the symptoms appear.136
Histamine 2 receptor antagonists are a class of acid inhibitors that are less effective than PPIs but better than placebo in healing reflux esophagitis and controlling symptoms. They can be used in NERD patients to control reflux symptoms. Adding these drugs at night may be effective in patients with nocturnal reflux. Moreover, in some patients with GERD refractory to PPI therapy, it may be beneficial to add a drug from this group at night.37,151,152 However, attention should be paid to potential tachyphylaxis that may occur very quickly (usually after 2‑4 weeks, and even within the first 7 days). It was suggested that the long‑term effect of a combination therapy is the same as that of PPI monotherapy53,153 (Table 6).
Antacids, as well as alginates and hyaluronic acid in combination with chondroitin sulfate can be used as an on‑demand therapy, to relieve intermittent GERD symptoms or as an add‑on therapy to an acid suppression therapy (PPI or PPI and histamine 2 receptor antagonists). The main advantage of antacids containing such compounds as aluminum or calcium and magnesium salts is that they reduce the symptoms rapidly. However, they neither provide good long‑term symptom control nor heal inflammatory esophageal changes, and do not prevent GERD complications54 (Table 6). Drugs containing alginates can create a physical antireflux barrier (“raft” formation) and increase viscosity of stomach contents. It was suggested that they are most useful in neutralizing the acid pocket.53 Adding them to the therapy with acid suppressive drugs increases effectiveness of the treatment: it reduces the severity of heartburn and acid esophageal exposure, and may help control GERD symptoms.49,53,154-158
Another medication is a combination of hyaluronic acid with chondroitin sulfate. Its mechanism of action is the formation of a protective layer on the surface of the esophageal mucosa. In a randomized study in NERD patients, a combined therapy of PPI with a preparation of hyaluronic acid and chondroitin sulfate was more effective in reducing heartburn and regurgitation as well as all GERD symptoms than PPI and placebo, thus significantly improving the patient’s quality of life.159 This drug may therefore be an additional option for an add‑on therapy.160-162
Sucralfate is more effective than placebo in healing esophageal inflammatory changes, but due to the existence of more effective acid‑blocking drugs, it is mainly used in pregnant women.53
Prokinetic drugs should not be used routinely in GERD patients. Due to side effects, the use of metoclopramide and cisapride in GERD is not recommended, despite their potential impact on pathophysiological mechanisms in GERD, including improvement of peristalsis and gastric emptying.163 A drug that has the potential to improve gastric emptying is itopride, a D2 antagonist.163-165 An addition of this drug may be beneficial in GERD patients who report dyspeptic symptoms166 (Table 6). There are limited reports of the beneficial role of adding itopride to PPI therapy in alleviating mild GERD symptoms or laryngopharyngeal reflux.167,168
Reflux inhibitors include a group of drugs that reduce reflux episodes by lowering the frequency of transient relaxation of the LES. An example is baclofen, which is an agonist of B‑type γ-aminobutyric acid receptor. This drug reduces the rate of LES relaxation, reduces total reflux, weak acid reflux and duodenogastroesophageal reflux, increases LES resting pressure, and accelerates gastric emptying. Unfortunately, baclofen has a number of central side effects (including excessive sleepiness, dizziness, and seizures), and is not approved for use in GERD17,53,131,169-172 (Table 6).
Development of new drugs used in GERD has decreased significantly in recent years, mainly due to the wide availability and high effectiveness of PPIs.
Endoscopic treatment
In recent years, a number of new, minimally invasive endoscopic methods have been developed to improve the effectiveness of the antireflux barrier – the gastroesophageal junction. They include, for example, ablative therapy (antireflux ablation therapy, ARAT, Stretta procedure) and endoscopic fundoplication using Medigus Ultrasonic Surgical Endostapler. While they appear to be promising, research into their effectiveness and safety is ongoing and their availability is limited.53,131,173-175
Surgical treatment
The most common method of antireflux surgery is laparoscopic fundoplication. The essence of this procedure is to create a fold from the bottom of the stomach around the esophagus. The procedure may involve a complete fundoplication (covering the entire circumference of the esophagus, 360 °) by the Nissen method, incomplete fundoplication with posterior Toupet method (270 °), or anterior Dora or Watson method (180 °).176-188
The utilization of fundoplication has decreased in recent years. The number of surgical fundoplications in the United States was similar in 2003 and 2013. In addition, a gradual increase in the use of acid suppressive therapy after surgery was observed. Overall, post‑fundoplication PPI use increased from 45% in 2010 to 80% in 2013.176 The results of studies comparing surgical treatment with pharmacological treatment in GERD patients are contradictory.177-184 In one study, over 80% of patients with documented GERD were asymptomatic after 10 years of follow‑up.177 In another study, 60% of patients did not require PPIs after 17 years of follow‑up.178 In other studies, 60%–80% of patients started taking PPIs again within a few years after surgery.179,184 The LOTUS study showed that both acid suppressive therapy and surgery enabled symptom remission to be achieved in the majority of patients over a 5‑year follow‑up. Heartburn was reported by a similar percentage of patients receiving esomeprazole and those undergoing surgery (16% and 8%, respectively), while regurgitation was significantly less frequent in the surgical group.184 In patients with documented GERD, who underwent surgery, a meta‑analysis of 7 studies showed that antireflux surgery was more effective than pharmacological treatment in terms of relief of heartburn and regurgitation, although a significant proportion of patients still required pharmacological treatment to control symptoms. Satisfaction with treatment and symptom control, as well as with quality of life, were greater in patients undergoing surgery.180,189,190 The economic aspect of chronic PPI use may also favor surgical treatment. A 2015 review of 4 randomized, controlled trials involving 1160 patients undergoing laparoscopic fundoplication (589 patients) or treated with PPIs (571 patients) showed that there are still many doubts. This does not allow for establishing a precise balance of the benefits and side effects or complications of fundoplication in comparison with PPIs, especially over a long‑term follow‑up period.181 Therefore, further research is necessary, taking into account patients’ assessment of the severity of symptoms and complications, quality of life, and the impact of symptoms on social and occupational functioning in the long‑term follow‑up.
Most of the studies of antireflux surgery in chronic cough, laryngopharyngeal reflux disease, and asthma are retrospective, uncontrolled studies involving small groups of patients.191-200 One study comparing the effect of Nissen fundoplication with histamine H2 receptor antagonists in GERD patients with asthma, reported an improvement in asthma symptoms after 2 years in 75% of patients undergoing surgery and only in 9% of patients treated pharmacologically.191 Despite promising observations, most surgeons do not recommend surgery in patients with extraesophageal symptoms without concomitant typical GERD symptoms, due to a lack of sufficient data from randomized trials.17,45 In addition, extraesophageal symptoms respond worse to the surgery than typical symptoms. The best predictor of improvement after surgery is a good early response to PPI therapy.197,199 In a 1‑year follow‑up, surgical treatment in the case of laryngeal symptoms refractory to PPI treatment had no advantage over PPI continuation and only 10% of patients after surgery and 7% of patients treated with PPIs reported improvement in symptoms.200
After antireflux surgery, approximately 50%–93% of patients report an inability to belch and vomit, abdominal distension, excessive gas flow, 10%–50% of patients report dysphagia, and 18%–33% diarrhea.183,184,186,201,202 In the above‑mentioned LOTUS study, comparing pharmacological and surgical GERD treatment, belching (40% vs 28%), flatulence (57% vs 40%) and dysphagia (11% vs 5%) were significantly more frequent after surgery.184 Surgical treatment is associated with a risk of death and complications in the perioperative period, although laparoscopic surgery significantly reduces this risk. Reoperations were required in about 5.2% of patients after 5 years and 6.9% of patients 10 years after the procedure.183,184,186,201,202 When comparing different types of surgery, Nissen fundoplication is associated with a higher but not significant incidence of dysphagia than anterior fundoplication. Of note, reoperations were observed more frequently after the latter.188 When analyzing incomplete fundoplication, anterior and posterior fundoplication gave similar results in terms of symptom control, dysphagia frequency, and treatment satisfaction.203 In another study, the posterior approach was found more effective than the anterior approach, taking into account postoperatively observed reduced heartburn rate, reoperation frequency, and the need for PPIs.204 In patients with hiatal hernia, Nissen fundoplication gives much better results than incomplete fundoplication. The procedure’s success depends on proper qualification of patients and its execution in a reference center. Surgical treatment may be beneficial in a carefully selected group of patients. All patients should undergo an endoscopy, pH or pH and impedance monitoring, and esophageal manometry.17,45,47,51,95,131,132,205 Relative contraindications to the surgical treatment are older age, severe comorbidities, and significant esophageal motility disorders. The best predictors of a good response to surgery include documented GERD (abnormal AET, no esophageal motility disorders), good response to PPIs, typical symptoms, and the presence of hiatal hernia.17,45,48,51,95,114,205,206
Surgical treatment may therefore be considered in patients with typical symptoms who respond well to PPI therapy but are intolerant to PPI, experience side effects, or do not accept long‑term PPI therapy. Surgical treatment may also be indicated in patients with insufficient PPI response, provided that GERD is objectively confirmed and functional heartburn is excluded. A complete lack of response to acid suppressive therapy should raise doubts as to the correctness of GERD diagnosis, and in patients with refractory GERD in whom surgery is considered, requires a full evaluation with pH and impedance monitoring, or possibly pH monitoring.17,18,51,53,95,103,131,132,207-210 A recently published study comparing the effectiveness of pharmacological and surgical therapy showed great benefits of comprehensive preoperative diagnostics in patients with refractory GERD.211 Patients with symptoms persisting despite PPI therapy were initially enrolled in the study. Further diagnostics included EGD, esophageal biopsy, manometry, and pH and impedance monitoring. Ultimately, 78 patients were randomized to either pharmacological therapy or Nissen fundoplication. After 1 year of observation, surgical treatment was more effective (67% of patients presented with improved symptoms) than pharmacological treatment (reduction of symptoms in 28% of patients receiving omeprazole with baclofen and possibly desipramine, and in 12% of patients receiving omeprazole with placebo). This study showed that patients with reflux–associated heartburn despite PPI therapy constituted a small subgroup among patients not responding to PPIs. Their identification, which is possible only through comprehensive diagnostics, is necessary during qualification for surgical treatment, because this strictly selected subgroup of patients may benefit from fundoplication.
Surgical treatment should be considered in symptomatic patients (eg, persistent regurgitation) with a large hiatal hernia. In obese patients with GERD, bariatric surgery is the preferred treatment option.17,49,53,95,131,210,212 In patients with morbid obesity or persistent symptoms after fundoplication, Roux‑en‑Y gastric bypass should be considered212 (Table 7).
The best candidates for antireflux surgery are: | Antireflux surgery should be avoided in the case of: |
|
|
The ACG guidelines suggest that surgery should be avoided in the case of extraesophageal symptoms.17 Surgical treatment should not be offered to patients with extraesophageal GERD symptoms unresponsive to PPI therapy.17,45,49,53,95 It can be considered in patients with objectively confirmed GERD refractory to pharmacological treatment, taking into account other causes of the symptoms not related to GERD.46 The guidelines for the management of chronic cough also do not recommend surgical treatment in patients with chronic cough and normal esophageal pH monitoring results or with esophageal motility disorders.45 It is suggested that surgery may be considered only in patients with chronic cough and confirmed abnormal acid exposure, but with normal esophageal motility45 (Table 7).
Diagnostic and terapeutic management in GERD
Typical reflux syndrome
STATEMENT 42. The presence of a typical reflux syndrome is an indication for empirical PPI therapy (A / I‑90%, II‑10%).
STATEMENT 43. Empirical PPI therapy for 8 weeks is recommended for symptom relief (A / I‑90%, II‑10%).
STATEMENT 44. Empirical PPI therapy should be started at the standard dose, applied once a day (A / I‑90%, II‑10%).
STATEMENT 45. For optimal inhibition of hydrochloric acid secretion, classic PPIs are administered 30‑60 minutes before meals (A / I‑90%, II‑10%).
STATEMENT 46. Maintenance treatment with PPIs is recommended in patients with recurrence of symptoms after PPI discontinuation. This treatment should be carried out at the lowest effective dose, daily, on‑demand, or intermittently (B / I‑80%, II‑20%).
STATEMENT 47. On‑demand or intermittent PPI therapy may be considered in patients with nonerosive and uncomplicated GERD and in patients with LA grade A esophagitis at an early age in whom other potential factors contributing to acid reflux were eliminated (B / I‑60%, II‑40%).
STATEMENT 48. Histamine H2 antagonists may be used as maintenance therapy in patients with normal endoscopy to control symptoms. Antacids and / or topical mucosal preparations may also be considered (B / I‑90%, II‑10%).
STATEMENT 49. In the absence or partial response to once daily PPIs, apply PPIs at the standard dose twice daily for 8 weeks. Alternatively, a different PPI can be used and / or a drug from a different group can be added (add‑on therapy): histamine H2 receptor antagonists, antacids and / or topical mucosal preparations (B / I‑60%, II‑30%, III‑10%).
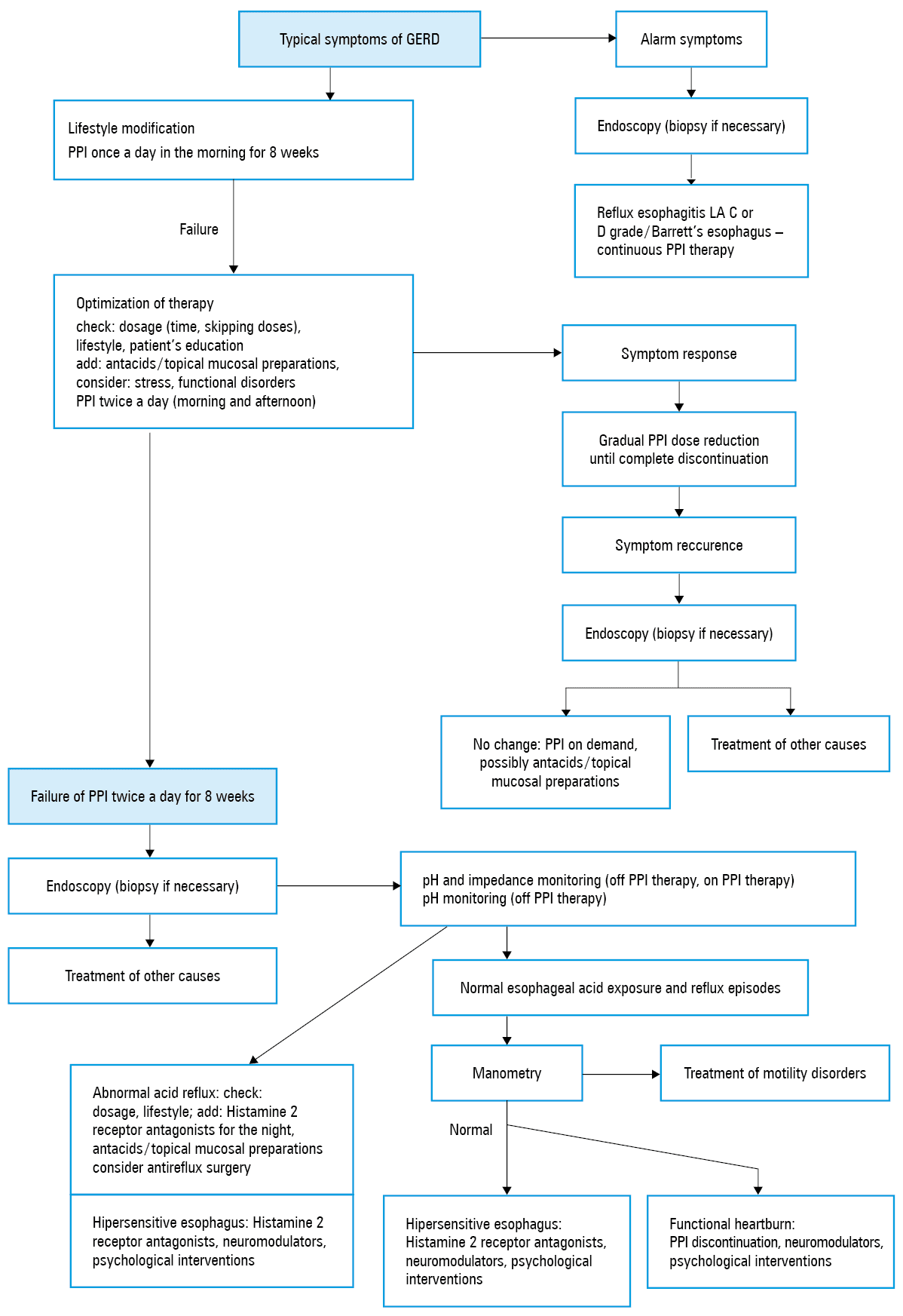
Management algorithm is shown in Figure 2. Comments in Supplementary material, Part 2.6. See appropriate references.37,51,213-215
Refractory GERD
STATEMENT 50. Refractory GERD should be considered in the absence of symptom improvement after 8 weeks of treatment with the standard dose of PPIs used twice daily (B / I‑90%, II‑10%).
STATEMENT 51. The first step in managing a patient suspected of refractory GERD is to reassess the symptoms and ensure that the patient is taking the medication correctly (A / I‑90%, III‑10%).
STATEMENT 52. Diagnosis of refractory GERD includes EGD, ambulatory pH and impedance monitoring, and esophageal manometry (B / I‑100%).
STATEMENT 53. Functional heartburn and hypersensitive esophagus are significant causes of PPI therapy failure (B / I‑60%, II‑40%)
Management algorithm is shown in Figure 2. Comments in Supplementary material, Part 2.7. See appropriate references.17,49,51,53,93,95,96,118-121,131,136,144,215-225
Extraesophageal syndromes
STATEMENT 54. Due to the multifactorial etiology of extraesophageal symptoms, in these cases a laryngological and pulmonological / allergological evaluation is necessary. Ideally, diagnosis of the causes of extraesophageal symptoms should be performed prior to gastroenterological evaluation (C / I‑80%, II‑20%).
STATEMENT 55. Empirical PPI therapy (standard dose twice a day) can be started in patients with extraesophageal symptoms with concomitant typical GERD symptoms. This treatment should be continued for 8‑12 weeks (C / I‑90%, II‑10%).
STATEMENT 56. In patients with improvement of symptoms after PPI therapy, treatment should be continued with the lowest effective dose. Lack of improvement after PPI requires further diagnostics (C / I‑90%, II‑10%).
STATEMENT 57. Empirical PPI therapy should not be initiated in patients reporting only extraesophageal symptoms. In these cases, a comprehensive laryngological, pulmonological / allergological assessment (if not performed previously) and pH and impedance or pH monitoring (before PPIs are instituted) are necessary to confirm or rule out GERD (C / I‑80%, II‑20%)
Comments in Supplementary material, Part 2.8. Management algorithm is shown in Figure 3. See appropriate references.17,45,46,95,226,227
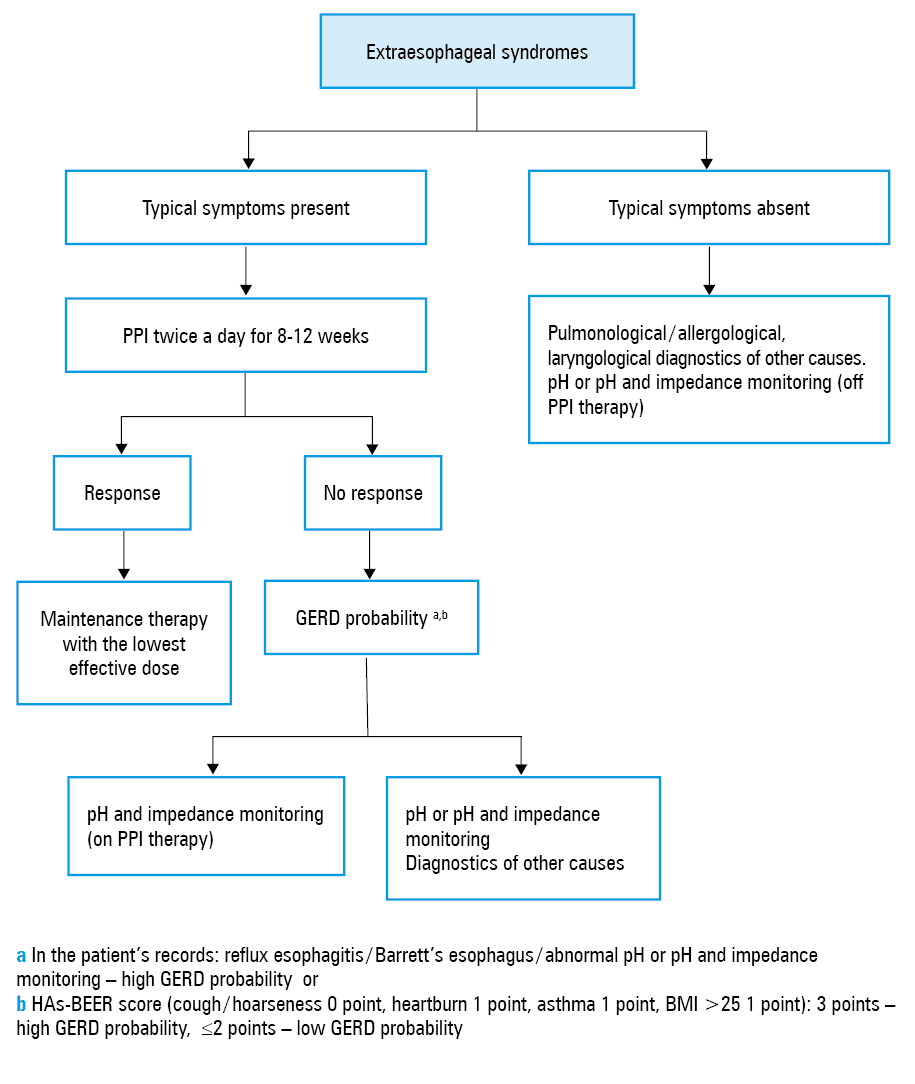
Abbreviations: BMI, body mass index; others, see Tables 3 and 4
Chest pain
STATEMENT 58. In the case of chest pain, possible cardiological causes should be ruled out first. Before starting PPI therapy, the following diagnostics should be performed: EGD, pH or pH and impedance monitoring, and esophageal manometry (C / I‑70%, II‑20%, III‑10%).
STATEMENT 59. PPI therapy should be started in patients with chest pain and confirmed GERD (C / I‑90%, II‑10%).
STATEMENT 60. In patients with chest pain that do not respond or partially respond to PPI therapy, the addition of pain modulators may be considered (C / I‑50%, II‑50%)
Comments in Supplementary material, Part 2.9. See appropriate references.17,228
Dysphagia
STATEMENT 61. The presence of dysphagia is an indication for an urgent endoscopy with biopsy to exclude cancer, GERD complications, and eosinophilic esophagitis (A / I‑100%)
Comments in Supplementary material, Part 2.10. See appropriate references.17,38,39,47,103,229
Belching
STATEMENT 62. Belching can be a symptom of GERD, but it can also result from functional and behavioral disorders (C / I‑70%, II‑30%)
Comments in Supplementary material, Part 2.11. See appropriate references.95,96,230
GERD management in pregnancy
STATEMENT 63. In pregnant women with GERD, it is recommended to modify the lifestyle and diet. Pharmacological treatment should be carried out at the lowest effective dose and for the shortest duration possible. Preferred drugs are alginates and sucralfate. PPIs can be used in case of severe symptoms (B / I‑100%)
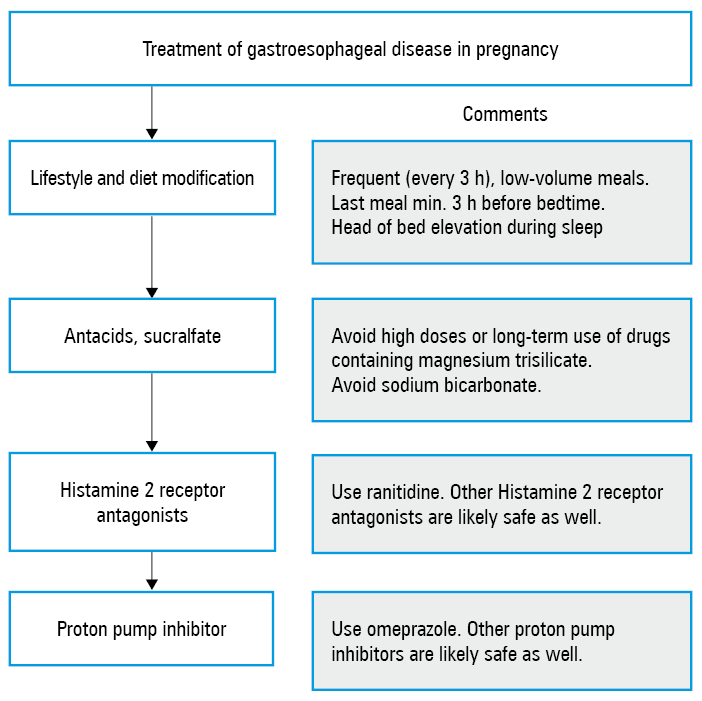
Management algorithm is shown in Figure 4. Comments in Supplementary material, Part 2.12. See appropriate references.49,231-238
GERD complications
STATEMENT 64. PPIs at a standard dose taken once a day for 8 weeks are used in the treatment of reflux esophagitis. Patients with LA grade C and D reflux esophagitis and esophageal stricture require maintenance therapy (A / I‑80%, II‑10%, III‑10%).
Barrett’s esophagus treatment
STATEMENT 65. Chronic PPIs therapy in asymptomatic patients with Barrett’s esophagus, although under discussion, is recommended by most experts (B / I‑80%, II‑20%).
STATEMENT 66. In patients with Barrett’s esophagus and GERD symptoms and / or esophagitis, it is recommended to use PPIs at doses sufficient to control GERD symptoms and heal inflammatory lesions (B / I‑80%, II‑20%).
STATEMENT 67. In patients with Barrett’s esophagus without GERD symptoms, PPI therapy at a standard dose once a day is recommended (C / I‑80%, II‑20%).
STATEMENT 68. Endoscopic treatment of Barrett’s esophagus should be carried out in an expert center specializing in this field (C / I‑90%, II‑10%).
STATEMENT 69. Endoscopic resection and / or ablative therapy should not be used in Barrett’s esophagus without dysplasia (B / I‑90%, II‑10%).
STATEMENT 70. All visible focal lesions, regardless of the degree of neoplasia, should be removed endoscopically (preferably by endoscopic mucosal resection) to obtain an appropriate histopathological assessment (A / I‑100%).
STATEMENT 71. Endoscopic treatment of esophageal adenocarcinoma T1a meeting the criteria for oncological completeness is considered the treatment of choice (A / I‑100%).
STATEMENT 72. Endoscopic treatment of esophageal adenocarcinoma in T1b (sm1) stage, meeting the criteria for oncological completeness, may be considered as an alternative to surgical treatment (C / I‑90%, II‑10%).
STATEMENT 73. Barrett’s esophagus with persistent (in two consecutive studies) macroscopically invisible (low or high grade) dysplasia (diagnosed by random biopsy) should undergo ablative treatment (B / I‑100%).
STATEMENT 74. After endoscopic removal of visible focal lesions containing dysplasia / neoplasia (regardless of its degree), the remaining metaplastic epithelium should be destroyed, preferably by RFA technique (A / I‑80%, II‑20%)
Comments in Supplementary material, Part 2.13. See appropriate references.17,67,70,71,85,94,136,138,141,239-253
- Henke CJ, Levin TR, Henning JM, Potter LP. Work loss costs due to peptic ulcer disease and gastroesophageal reflux disease in a health maintenance organization. Am J Gastroenterol. 2000; 95: 788‑792. | Crossref
- Liker H, Hungin P, Wiklund I. Managing gastroesophageal reflux disease in primary care: the patient perspective. J Am Board Fam Pract. 2005; 18: 393‑400. | Crossref
- Jurkowska G, Swidnicka‑Siergiejko A, Łagoda K, et al. Quality of life in patients with gastroesophageal reflux disease following pharmacotherapeutic, endoscopic, and surgical treatment. Studia Medyczne. 2016; 32: 299‑306. | Crossref
- Petryszyn P, Staniak A, Grzegrzolka J. Is the use of esomeprazole in gastroesophageal reflux disease a cost‑effective option in Poland? J Comp Eff Res. 2016; 5: 169‑178. | Crossref
- Shaheen NJ, Hansen RA, Morgan DR, et al. The burden of gastrointestinal and liver diseases, 2006. Am J Gastroenterol. 2006;101: 2128‑2138. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION