Reversing the poor prognosis of primary amyloid light‑chain amyloidosis with cardiac involvement



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Reversing the poor prognosis of primary amyloid light‑chain amyloidosis with cardiac involvement
New York Heart Association (NYHA) functional class, brain natriuretic peptide (BNP), and C‑reactive protein (CRP) levels are known risk factors for increased mortality in patients with primary amyloid light‑chain (AL) amyloidosis.1 However, therapeutic options to overcome its poor prognosis are limited. A regimen approved in January 2021 and including daratumumab (Dara) with cyclophosphamide, bortezomib, and dexamethasone (CyBorD) demonstrated improved hematological and organ response in patients with newly diagnosed AL amyloidosis.2 Here, we describe a clinical image of a 63‑year‑old man with primary AL amyloidosis presenting with a rapidly progressive heart failure.3
The patient was diagnosed with acute heart failure (NYHA III). In addition, he had a history of hypertension, diabetes, and renal failure (estimated glomerular filtration rate, 50 ml/min/1.73 m2). The electrocardiogram demonstrated a depression of 1 mm of ST segments with inverted T waves in I, avL, and V1–V6 leading to coronary angiography, which was normal. On echocardiography, red flags for cardiac amyloidosis were found, that is, myocardial granular sparkling, and thickening of the left (LV) and right ventricle (Figure 1A), significant enlargement of both atria, LV ejection fraction of 50%, and a restrictive filling pattern with low mitral annulus velocity in using tissue Doppler imaging (<5 cm/s).4 The global longitudinal strain (GLS) was abnormal (–10.4%), with apical sparing (Figure 1B), and scintigraphy with technetium‑99m‑labeled 3,3‑diphosphono‑1,2‑propanodicarboxylic acid was negative for transthyretin amyloidosis. Myocardial volume overload was confirmed by significantly elevated cardiac biomarkers, N‑terminal pro‑brain natriuretic peptide (NT‑proBNP) (Figure 1C), and high sensitivity‑troponin I (45.6 ng/l). AL amyloidosis (kappa light chain) was diagnosed, Mayo stage III (Figure 1D).
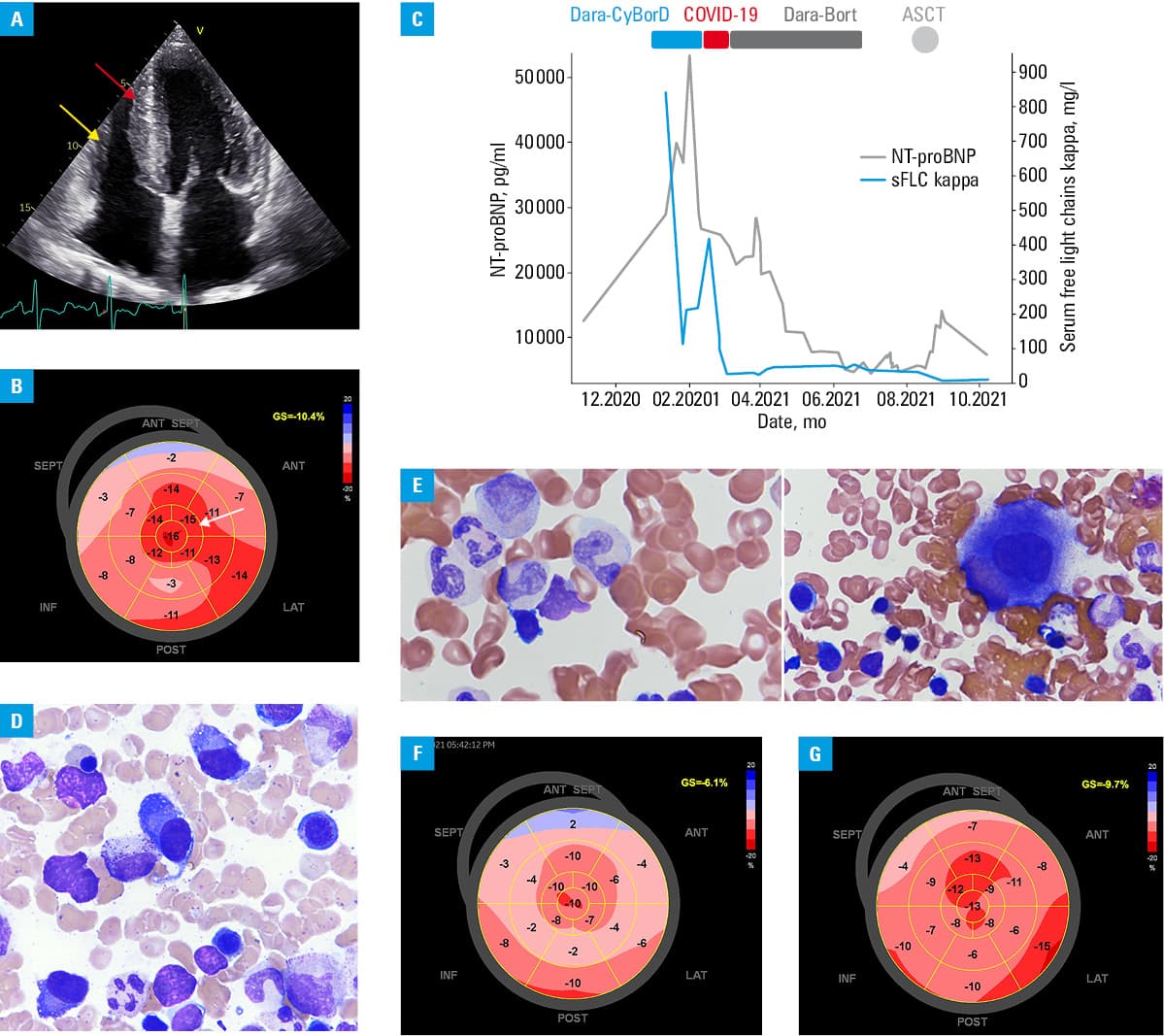
In January 2021, the patient received treatment with Dara‑CyBorD under an emergency drug access scheme. The hematological response was immediate and followed by a gradual decline in NT‑proBNT by 60% from its peak (Figure 1C). The treatment was interrupted after 2 cycles due to SARS‑CoV‑2 infection. After recovery, the patient received maintenance treatment with daratumumab plus bortezomib. Granulocyte colony‑stimulating factor‑based (G‑CSF) stem cell mobilization failed, and a second attempt with plerixafor plus G‑CSF plus cytarabine was successful. In August 2021, the patient received high‑dose chemotherapy (MEL140) followed by autologous stem cell transplantation. The therapy deepened the response (complete response [CR]) (Figure 1C and 1E), and minimal residual disease (MRD) was undetectable. Renal function was stable, whereas further cardiac improvement was observed after a maximum deterioration (GLS –6.11%; Figure 1C) as a decrease in GLS to baseline levels (Figure 1F vs 1G). The patient returned to full‑time work.
Historically, the median overall survival in Mayo cardiac stage III AL amyloidosis was 7 months, with 42% of patients dying before the first response evaluation.3 Dara‑CyBorD remarkably improved hematological response and organ involvement.2 The treatment, interrupted and modified, reversed the poor prognosis. Consolidative stem cell transplant therapy became possible, and resulted in MRD‑negativity associated with improved cardiac function after CR.5
- Tahir UA, Doros G, Kim JS, et al. Predictors of mortality in light chain cardiac amyloidosis with heart failure. Sci Rep. 2019; 9: 8552‑8552. | Crossref
- Palladini G, Kastritis E, Maurer MS, et al. Daratumumab plus CyBorD for patients with newly diagnosed AL amyloidosis: safety run‑in results of ANDROMEDA. Blood. 2020; 136: 71‑80. | Crossref
- Wechalekar AD, Schonland SO, Kastritis E, et al. A European collaborative study of treatment outcomes in 346 patients with cardiac stage III AL amyloidosis. Blood. 2013; 121: 3420‑3427. | Crossref
- Dorbala S, Ando Y, Bokhari S, et al. SNC/AHA/ASE/EANM/HFSA/ISA/SCMR/SNMMI expert consensus recommendations for multimodality imaging in cardiac amyloidosis: part 2 of 2‑Diagnostic criteria and appropriate utilization. J Nucl Cardiol. 2020; 27: 659‑673. | Crossref
- Palladini G, Paiva B, Wechalekar A, et al. Minimal residual disease negativity by next‑generation flow cytometry is associated with improved organ response in AL amyloidosis. Blood Cancer J. 2021; 11: 34. | Crossref
ARTICLE INFORMATION