Sex differences in incidence, management, and outcomes in adult patients aged over 20 years with clinically diagnosed myocarditis in the last 10 years: data from the MYO‑PL nationwide database
Key words: cardiomyopathy, endomyocardial biopsy, epidemiology, heart failure, seasonal incidence



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Sex differences in incidence, management, and outcomes in adult patients aged over 20 years with clinically diagnosed myocarditis in the last 10 years: data from the MYO‑PL nationwide database
Introduction: Comprehensive epidemiological data about the course of myocarditis and sex differences are lacking.
Objectives: We aimed to investigate the current differences in the incidence, clinical characteristics, management, and outcomes of men and women with a clinical diagnosis of myocarditis in Poland in the last 10 years.
Patients and methods: The nationwide MYO‑PL (Occurrence, Trends, Management, and Outcomes of Patients with Myocarditis in Poland) database identified hospitalization records with a primary diagnosis of myocarditis following the International Classification of Diseases and Related Health Problems, 10th Revision (ICD‑10), derived from the database of the national health care insurer; ClinicalTrials.gov identifier: NCT04827706.
Results: A total of 16 319 patients (4208 [25.8%] women and 12 111 [74.2%] men) aged over 20 years with a hospital‑based clinical diagnosis of myocarditis were included in the study. The women were older than the men (median age, 54 (36–70) and 35 (28–47) years, respectively). The incidence of myocarditis was age-, sex-, and season‑dependent. The incidence rate of myocarditis increased over time only in men. Although women were more symptomatic and demonstrated more comorbidities than men, they were less likely to be admitted to a cardiology ward or undergo diagnostic tests. Regardless of the age and sex, the patients with myocarditis had a poorer prognosis than the general population. The women aged 21–40 years had a poorer prognosis than the men of the same age.
Conclusions: The incidence of myocarditis was age-, sex-, and season‑dependent. Significant improvement is required in the management of myocarditis, including the initial diagnostic process, as well as short- and long‑term therapy, particularly in women.
What's new?
The MYO‑PL database is a nationwide registry designed to evaluate the incidence, clinical characteristics, management, and outcomes of patients hospitalized due to myocarditis in the last 10 years. The presented analysis showed that in the last 10 years, the incidence of myocarditis increased, particularly in men. Furthermore, survival rates for patients with myocarditis were worse than in the general population. Therefore, the diagnosis but also the treatment of myocarditis require significant improvement.
Introduction
Myocarditis is an increasingly common cause of acute and chronic heart failure.1,2 The main known factors contributing to myocarditis are infections (mostly viral), postinfective autoimmune reactions, autoimmune diseases, and toxins. The clinical manifestation of myocarditis may vary widely. It may present as an asymptomatic disease or with mild symptoms, slight ventricular dysfunction, and resolve spontaneously without treatment. Up to 30%–50% of biopsy‑proven cases of myocarditis are associated with acute or slowly aggravating cardiac function, leading to dilated cardiomyopathy or life‑threatening arrhythmias.1,3 The initial diagnosis of clinically suspected myocarditis is based on the clinical presentation and noninvasive work‑up (electrocardiography, echocardiography, cardiac magnetic resonance [CMR], cardiac troponins).1,2
Nevertheless, the right diagnosis remains a serious challenge to contemporary cardiology due to the scarcity of knowledge gained via systematic investigation. It was especially emphasized during the COVID‑19 pandemic, when most published papers included conflicting definitions of myocarditis, showing a distorted picture of the actual scale of the disease.4,5
The available data are seriously limited due to the design of the reports mainly discussing small, single‑center studies. Current data indicate that myocarditis is more common in men than in women,5 however, its actual incidence and distribution rate according to age is largely unknown. A previous report showed an increasing incidence of hospitalizations for myocarditis in the years 2007–2014 in the United States, both in men and women.6
There is also a lack of data regarding sex differences in clinical characteristics, management, and long‑term outcomes. The Global Burden of Disease 2016 and 2019 Study (GBD2016 and GBD2019) revealed an increase of approximately 10% in all‑age deaths. Moreover, the levels of years of life lost due to cardiomyopathy and myocarditis were much higher than expected over the past decades.7,8 The presented analysis indicates a pressing need for obtaining actual population data on myocarditis, as they may provide relevant information on the demographic trends and outcomes in recent years. Population‑based studies are important to highlight the epidemiological and unselected characteristics of the cohort. Such results could be hypothesis‑generating, and can direct and stimulate further research.
Therefore, a nationwide MYO‑PL (Occurrence, Trends, Management, and Outcomes of Patients with Myocarditis in Poland) database was designed to investigate current differences in the incidence, clinical characteristics, management, and long‑term outcomes of the adult mem and women with a hospital‑based clinical diagnosis of myocarditis in Poland in the last 10 years. This paper is a continuation of a recently published article on the population of children and young adults.9
Methods
The National Health Fund (NHF) data were used to design the MYO‑PL database in a retrospective‑prospective manner. The rationale for and design of the database based on NHF resources were previously discussed in the literature.2 The NHF is the only public health care insurer in Poland. It reimburses health care services and drugs provided by health care providers (both public and private) with public funds collected from health insurance premiums. In Poland, public health insurance covers 88.4% of the inhabitants.
We gathered information concerning the health care services reported over the years 2009–2020 with a diagnosis of myocarditis hospitalizations reported with codes I40, I40.0, I40.1, I40.8, I40.9, I41, I41.0, I41.1, I41.2, I41.8, I51.4, and B33.2 according to the International Classification of Diseases and Related Health Problems, 10th Revision (ICD‑10). The diagnostic criteria of myocarditis (based on international ICD‑10 codes) were clinician‑dependent, reflecting a routine clinical practice. The diagnosis of myocarditis did not need to be confirmed histologically. Our analysis included patients aged over 20 years.
The dataset was limited to the first hospitalization due to myocarditis, that is, only patients for whom no information about a previous diagnosis of myocarditis (either ambulatory visit or hospitalization with a myocarditis ICD‑10 code) was reported. There were no specific exclusion criteria.
To establish the baseline characteristics of the selected patients, the database was searched 400 days back from the initial diagnosis of myocarditis. We obtained information about in‑hospital and long‑term outcomes, including all‑cause mortality, as well as the occurrence of selected diseases (defined as receiving a service where a selected ICD‑10 code was reported), and procedures (defined with codes according to ICD, 9th Revision, Clinical Modification [ICD‑9‑CM]). For the follow‑up, at least a 6‑month period was used. Thus, only the patients with the diagnosis of myocarditis between January 2011 and December 2019 were finally included in the analysis.
To show differences related to the age of the patients hospitalized for myocarditis, long‑term outcomes were assessed regarding the age groups.
Data from the Central Statistical Office of Poland were used to refer the obtained results to the population of Poland, and to obtain life Tables for relative survival analysis.
Ethics approval and patients’ informed consent were not required for this study, as it involved the analysis of administrative data.
Statistical analysis
The results were presented as the median (and quartiles) for continuous variables, and percentages for ordinal variables. The Pearson χ2 test, t test, and logistic regression were used for the assessment of associations between the studied parameters. The relative survival (with 95% CIs) was calculated using the Hakulinen method employing single age-, year-, and sex‑specific life Tables for the general Polish population. The observed survival was analyzed using the Kaplan–Meier estimates. For comparison between the sexes, odds ratio (OR) adjusted for age was calculated using the logistic regression. In terms of hospital admission (Table 1), logistic regression model was built for each unit separately, in which the explanatory variables were the age and the binary variable specifying the sex (1, woman; 0, man). The dependent variable was a binary variable specifying whether a given person was admitted to a given department or not. For each regression, an estimate of the coefficient standing for the sex variable was obtained, and the OR was calculated (the ratio of the odds of hospitalization in the department X for women vs the odds of hospitalization in this department for men). A P value below 0.05 was considered significant. All tests were 2‑tailed. R software, version 3.6.2 (R Core Team 2020, R Foundation for Statistical Computing, Vienna, Austria) was used for the statistical analysis.
Variable | Total (n = 16 319) | Women (n = 4208) | Men (n = 12 111) | OR (95% CI)a | P valuea | |
a Comparison between sex groups, adjusted for age
b Sum of patients hospitalized in different wards may not equal the “Total” number, if a patient on the day of the first diagnosis of myocarditis was hospitalized at two different departments
c Any other hospital department within the last or following 6 months from the diagnosis of myocarditis
d Within the index hospitalization
e Within the last or following 6 months from the diagnosis of myocarditis
Abbreviations: IQR, interquartile range; n, number; OR, odds ratio | ||||||
Demographics | ||||||
Age, y, median (IQR) | 37 (29–56) | 54 (36–70) | 35 (28–47) | 0.001 | ||
Management | ||||||
Hospital ward on admission, n (%)b | Cardiology unit | 9812 (58.1) | 1806 (42.9) | 8006 (66.1) | 0.58 (0.53–0.62) | <0.001 |
General ward | 3270 (19.4) | 985 (23.4) | 2285 (18.9) | 1.16 (1.06–1.28) | 0.01 | |
Intensive care unit | 199 (1.2) | 77 (1.8) | 122 (1.0) | 1.29 (0.94–1.76) | 0.11 | |
Intensive cardiac care unit | 120 (0.7) | 16 (0.4) | 104 (0.9) | 0.62 (0.36–1.08) | 0.09 | |
Otherc | 3481 (21.3) | 1381 (32.8) | 2100 (17.3) | 1.63 (1.50–1.78) | <0.001 | |
Diagnostic procedures, n (%) | C‑reactive proteind | 6838 (41.9) | 1507 (35.8) | 5331 (44.0) | 0.88 (0.82–0.95) | <0.001 |
Troponinsd | 6905 (42.3) | 1478 (35.1) | 5427 (44.8) | 0.87 (0.81–0.94) | <0.001 | |
Brain natriuretic peptidesd | 2279 (14.0) | 488 (11.6) | 1791 (14.8) | 0.88 (0.79–0.99) | 0.03 | |
Echocardiographye | 13 018 (79.8) | 2938 (69.8) | 10 080 (83.2) | 0.70 (0.64–0.76) | <0.001 | |
Cardiac magnetic resonancee | 2721 (16.7) | 636 (15.1) | 2085 (17.2) | 1.10 (0.99–1.22) | 0.07 | |
Endomyocardial biopsye | 130 (0.8) | 29 (0.7) | 101 (0.8) | 1.05 (0.68–1.63) | 0.83 | |
Endomyocardial biopsy or heart catheterizatione | 211 (1.3) | 38 (0.9) | 173 (1.4) | 0.76 (0.53–1.11) | 0.15 | |
Coronary angiography (invasive or computed tomography)e | 5902 (36.2) | 1061 (25.2) | 4841 (40.0) | 0.46 (0.43–0.50) | <0.001 | |
Medical history (for the previous 400 days) | ||||||
Cardiac arrhythmias, n (%) | Atrial extrasystole | 781 (4.8) | 362 (8.6) | 419 (3.5) | 0.93 (0.79–1.09) | 0.37 |
Tachycardia, palpitations | 203 (1.2) | 94 (2.2) | 109 (0.9) | 2.60 (1.93–3.51) | 0.01 | |
Bradycardia | 10 (0.1) | 8 (0.2) | 2 (0.0) | 17.30 (3.53–84.70) | 0.01 | |
Atrial extra beat | 14 (0.1) | 6 (0.1) | 8 (0.1) | 1.48 (0.47–4.70) | 0.50 | |
Ventricular extrasystole | 39 (0.2) | 18 (0.4) | 21 (0.2) | 2.24 (1.13–4.44) | 0.02 | |
Paroxysmal tachycardia | 187 (1.1) | 85 (2.0) | 102 (0.8) | 2.11 (1.54–2.89) | 0.01 | |
Ventricular tachycardia | 46 (0.3) | 13 (0.3) | 33 (0.3) | 0.79 (0.40–1.57) | 0.50 | |
Ventricular fibrillation | 16 (0.1) | 8 (0.2) | 8 (0.1) | 3.17 (1.11–9.08) | 0.03 | |
Chronic coronary syndrome, n (%) | 1102 (6.8) | 488 (11.6) | 614 (5.1) | 0.92 (0.80–1.06) | 0.24 | |
Heart failure, n (%) | 1154 (7.1) | 450 (10.7) | 704 (5.8) | 0.69 (0.60–0.80) | <0.001 | |
Hypertension, n (%) | 3387 (20.8) | 1488 (35.4) | 1899 (15.7) | 1.31 (1.19–1.44) | <0.001 | |
Diabetes, n (%) | 800 (4.9) | 356 (8.5) | 444 (3.7) | 0.96 (0.82–1.13) | 0.66 | |
Stroke or transient ischemic attack, n (%) | 278 (1.7) | 118 (2.8) | 160 (1.3) | 0.86 (0.67–1.12) | 0.27 | |
Chronic kidney disease, n (%) | 208 (1.3) | 80 (1.9) | 128 (1.1) | 0.72 (0.53–0.97) | 0.03 | |
Asthma, n (%) | 688 (4.2) | 309 (7.3) | 379 (3.1) | 1.99 (1.68–2.35) | <0.001 | |
Autoimmune disease, n (%) | 239 (1.5) | 146 (3.5) | 93 (0.8) | 3.41 (2.57–4.53) | <0.001 | |
Psychiatric disease, n (%) | 394 (2.4) | 174 (4.1) | 220 (1.8) | 2.72 (2.19–3.37) | <0.001 | |
Infectious disease within the last 6 months, n (%) | Otolaryngologic and ophthalmic | 5159 (31.6) | 1337 (31.8) | 3822 (31.6) | 1.37 (1.26–1.49) | 0.01 |
Central nervous system | 12 (0.1) | 5 (0.1) | 7 (0.1) | 2.62 (0.77–8.88) | 0.12 | |
Respiratory | 2364 (14.5) | 720 (17.1) | 1644 (13.6) | 1.14 (1.03–1.26) | 0.01 | |
Digestive | 747 (4.6) | 248 (5.9) | 499 (4.1) | 1.35 (1.14–1.60) | 0.01 | |
Urogenital | 119 (0.7) | 43 (1.0) | 76 (0.6) | 1.08 (0.72–1.62) | 0.71 | |
Sepsis | 59 (0.4) | 15 (0.4) | 44 (0.4) | 0.56 (0.30–1.05) | 0.07 | |
Other | 941 (5.8) | 340 (8.1) | 601 (5.0) | 1.44 (1.24–1.67) | 0.01 | |
Results
Incidence of myocarditis, clinical characteristics, and hospital management
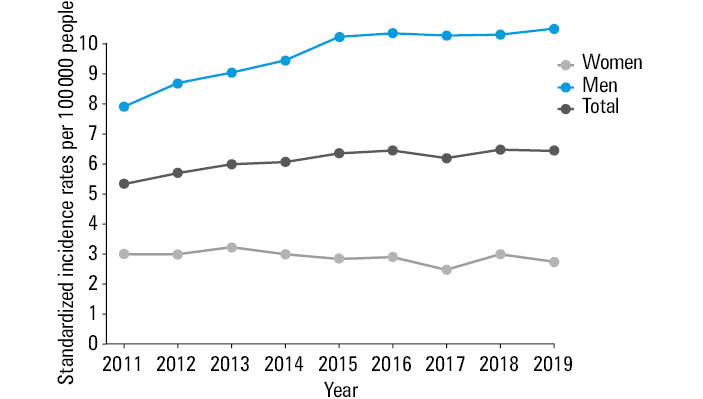
The analysis included 16 319 patients (4208 [25.8%] women and 12 111 [74.2%] men) with a clinical diagnosis of myocarditis, hospitalized between January 2011 and December 2019. The median age was 54 years in women (36–70) and 35 in men (28–47). The incidence of myocarditis was age- and sex‑related. Over the years 2011–2019, an increasing incidence rate of myocarditis was observed in men, while in women it remained stable (Figure 1). In men, myocarditis was the most frequent in the 21–30 and 31–40‑year age groups, and significantly lower in patients aged over 40 years (Table 2). In contrast, the myocarditis incidence rate in women tended to be higher in the older age groups (Table 2).
Age group, y | Average incidence | Year | P valuea | ||||||||
2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | 2019 | |||
a The χ2 test for the independence of the number of patients with myocarditis in a given age group by year | |||||||||||
Men | |||||||||||
21–30 | 17.03 | 12.18 | 15.06 | 14.73 | 17.65 | 18.09 | 19.35 | 18.87 | 18.81 | 18.50 | <0.001 |
31–40 | 13.32 | 11.44 | 11.36 | 12.08 | 13.25 | 14.73 | 13.61 | 14.46 | 13.68 | 15.26 | <0.001 |
41–50 | 6.59 | 3.92 | 4.77 | 6.94 | 5.41 | 6.93 | 7.76 | 7.25 | 8.74 | 7.57 | <0.001 |
51–60 | 4.53 | 4.22 | 4.27 | 4.16 | 4.39 | 4.15 | 4.46 | 4.92 | 4.99 | 5.21 | 0.52 |
61–70 | 4.67 | 6.23 | 4.95 | 5.03 | 3.88 | 4.79 | 4.64 | 4.59 | 4.14 | 3.74 | 0.02 |
71–80 | 6.11 | 7.50 | 9.10 | 7.34 | 6.62 | 6.55 | 5.00 | 3.60 | 3.94 | 5.36 | <0.001 |
81+ | 6.73 | 6.88 | 8.43 | 9.37 | 5.76 | 8.27 | 7.75 | 5.26 | 4.03 | 4.82 | 0.03 |
Women | |||||||||||
21–30 | 2.57 | 1.76 | 2.17 | 2.09 | 2.78 | 2.47 | 2.72 | 2.66 | 3.09 | 3.38 | 0.01 |
31–40 | 2.69 | 1.86 | 2.97 | 2.49 | 2.77 | 2.70 | 3.04 | 2.82 | 3.03 | 2.57 | 0.16 |
41–50 | 2.31 | 1.95 | 2.01 | 2.25 | 2.35 | 2.69 | 1.87 | 2.36 | 2.64 | 2.65 | 0.38 |
51–60 | 2.62 | 2.93 | 2.61 | 3.18 | 2.65 | 1.92 | 2.81 | 2.28 | 2.88 | 2.31 | 0.12 |
61–70 | 3.13 | 3.73 | 3.10 | 4.09 | 2.99 | 2.72 | 3.31 | 2.33 | 2.98 | 2.91 | 0.03 |
71–80 | 4.38 | 6.45 | 4.76 | 5.69 | 4.15 | 5.20 | 4.18 | 2.40 | 3.67 | 2.92 | <0.001 |
81+ | 5.17 | 7.25 | 7.30 | 6.94 | 6.31 | 5.12 | 3.97 | 2.89 | 3.62 | 3.08 | <0.001 |
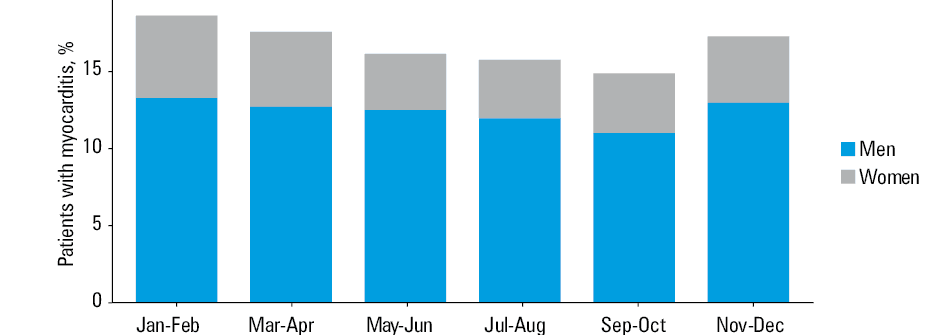
Seasonal variability in the incidence of myocarditis was also observed. Hospital admissions were more common between late autumn and early spring (November to April), for both sexes (Figure 2). Conversely, the lowest rates were observed in mid‑summer (July to August).
Men were more often admitted to a cardiology unit than women. Women were usually admitted to a general or another hospital ward. There was no difference in admissions to intensive (cardiac) care units (Table 1).
Clinical presentation at the time of hospital admission and medical history differed between the sexes. Cardiac arrhythmias were observed more often in women than in men. Although the analysis was age‑adjusted, women were more likely to be diagnosed with a heart failure and other comorbidities (hypertension, chronic kidney disease, as well as concomitant asthma or autoimmune disease). Infective diseases in the period of up to 6 months prior to the hospital admission, were more common in women.
The reported use of diagnostic procedures, particularly CMR and endomyocardial biopsy (EMB), was generally very low (16.7% and 0.8%, respectively). Interestingly, although women were more symptomatic and had more comorbidities, they were less likely to undergo the recommended diagnostic tests (biomarkers, echocardiographic evaluation, coronary angiography). Furthermore, a clear trend was visible toward more frequent CMR and EMB in men.
The main clinical characteristics and management of patients with myocarditis are presented in Table 1.
Outcomes
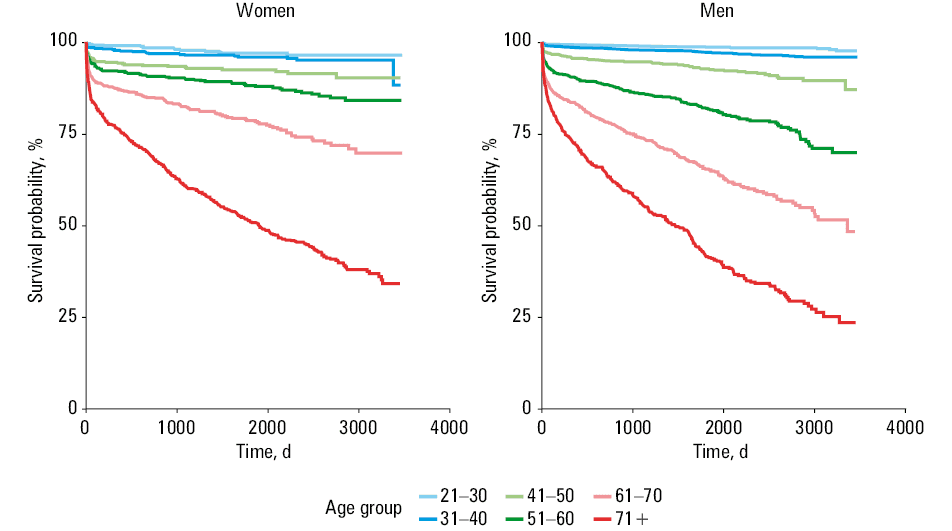
During the 5‑year follow‑up, women were at a higher risk of hospitalization for arrhythmias, autoimmune disease, heart failure and other causes, while men were at a higher risk of rehospitalization for myocarditis (Table 3). The relative survival of patients hospitalized for myocarditis was lower than in the general Polish population, irrespectively of the follow‑up time, age group, or sex. In both men and women, short‑term and long‑term outcomes deteriorated with age. In the youngest age group (21–40 years), the prognosis was poorer in women than in men. In contrast, the 5‑year prognosis was poorer for men in the 61–80‑year age group, and there were no significant differences in survival in the remaining age groups (Table 4). Figure 3 shows the Kaplan–Meier estimation of mortality in the patients hospitalized for myocarditis.
Reason for hospitalization | Women (n = 2193) | Men (n = 5761) | OR (women vs men) | 95% CI | P value |
Data are presented as number (percentage) unless indicated otherwise.
a Any other reason for hospitalization
Abbreviations: see Table 1 | |||||
Atrial fibrillation or atrial flutter | 134 (6.1) | 156 (2.7) | 1.11 | 0.86–1.44 | 0.42 |
Ventricular fibrillation, ventricular flutter or cardiac arrest | 13 (0.6) | 18 (0.3) | 1.19 | 0.55–2.60 | 0.66 |
Other cardiac arrhythmias or paroxysmal tachycardia | 138 (6.3) | 174 (3.0) | 1.91 | 1.49–2.46 | <0.001 |
Atrioventricular block | 13 (0.6) | 30 (0.5) | 0.52 | 0.26–1.03 | 0.06 |
Autoimmune disease | 57 (2.6) | 50 (0.9) | 3.66 | 2.42–5.53 | <0.001 |
Cardiomyopathy or heart failure | 267 (12.2) | 494 (8.6) | 0.71 | 0.59–0.84 | <0.001 |
Myocarditis | 54 (2.5) | 336 (5.8) | 0.68 | 0.50–0.93 | 0.01 |
Ischemic stroke, transient ischemic attack | 86 (3.9) | 100 (1.7) | 0.89 | 0.65–1.22 | 0.48 |
Pericarditis | 5 (0.2) | 11 (0.2) | 0.83 | 0.27–2.62 | 0.76 |
Pulmonary embolism | 12 (0.5) | 23 (0.4) | 1.00 | 0.47–2.13 | 0.99 |
Embolism and arterial thrombosis | 13 (0.6) | 19 (0.3) | 0.78 | 0.37–1.67 | 0.52 |
Other reasonsa | 1513 (69) | 3320 (57.6) | 1.37 | 1.23–1.53 | <0.001 |
Sex | Outcome | Age group | |||||||
Number of deaths (%) | Relative survival | ||||||||
21–40 | 41–60 | 61–80 | 81+ | 21–40 | 41–60 | 61–80 | 81+ | ||
Men | In‑hospital | 31 / 7962 (0.4) | 86 / 2558 (3.4) | 114 / 1347 (8.5) | 25 / 244 (10.3) | – | – | – | – |
30 days | 51 / 7962 (0.6) | 93 / 2558 (3.6) | 133 / 1347 (9.9) | 30 / 244 (12.3) | 0.995 (0.99–0.997) | 0.97 (0.96–0.98) | 0.92 (0.90–0.93) | 0.89 (0.85–0.93) | |
1 year | 86 / 7559 (1.1) | 158 / 2403 (6.6) | 253 / 1299 (19.5) | 80 / 234 (34.2) | 0.99 (0.99–0.99) | 0.95 (0.94–0.96) | 0.85 (0.82–0.87) | 0.76 (0.70–0.83) | |
3 years | 90 / 5697 (1.6) | 164 / 1741 (9.4) | 302 / 1007 (30.0) | 119 / 196 (60.7) | 0.99 (0.99–0.99) | 0.94 (0.93–0.95) | 0.80 (0.77–0.83) | 0.65 (0.55–0.75) | |
5 years | 89 / 3803 (2.3) | 148 / 1115 (13.3) | 310 / 728 (42.6) | 97 / 131 (74.1) | 0.99 (0.99–0.99) | 0.93 (0.92–0.95) | 0.75 (0.71–0.79) | 0.56 (0.42–0.70) | |
Women | In‑hospital | 11 / 1350 (0.8) | 41 / 1169 (3.5) | 82 / 1256 (6.5) | 76 / 433 (17.6) | – | – | – | – |
30 days | 14 / 1350 (1.0) | 50 / 1169 (4.3) | 91 / 1256 (7.3) | 91 / 433 (21.0) | 0.99 (0.99–0.996) | 0.97 (0.95–0.98) | 0.94 (0.93–0.95) | 0.82 (0.79–0.86) | |
1 year | 20 / 1280 (1.6) | 79 / 1116 (7.1) | 161 / 1199 (13.4) | 159 / 416 (38.2) | 0.98 (0.98–0.99) | 0.94 (0.93–0.96) | 0.90 (0.88–0.92) | 0.72 (0.67–0.77) | |
3 years | 26 / 948 (2.7) | 75 / 846 (8.9) | 204 / 953 (21.4) | 200 / 353 (56.7) | 0.97 (0.96–0.98) | 0.93 (0.92–0.95) | 0.85 (0.82–0.88) | 0.64 (0.57–0.71) | |
5 years | 22 / 635 (3.5) | 61 / 602 (10.1) | 184 / 690 (26.7) | 187 / 274 (68.3) | 0.97 (0.96–0.98) | 0.93 (0.91–0.95) | 0.83 (0.80–0.86) | 0.64 (0.54–0.73) | |
Discussion
The current epidemiology of myocarditis is unknown, as no large‑scale analyses have been conducted in recent years. The present nationwide MYO‑PL database provides a new and relevant information regarding population trends, demographics, and the outcomes of patients with myocarditis in routine clinical practice.
In our database, the incidence rate of myocarditis in men and women increased over the last 10 years, and confirmed previously available data showing that myocarditis is a male‑predominant disease. The incidence of myocarditis was age-, sex-, and season‑dependent. The incidence of myocarditis was higher in men than in women in all age groups. The median age at diagnosis was 54 and 35 years in women and men, respectively. Myocarditis occurred most frequently in men aged 21–30 and 31–40 years (Table 2). Moreover, the incidence rate in men showed that major differences in the frequency of myocarditis decreased with age. In contrast, women in all age groups showed more stable incidence rates and an increase of myocarditis diagnosis at postmenopausal age, which may result from a decrease in estrogen levels. Another report regarding the female population with myocarditis showed similarly stable incidence rates.10
The potential mechanisms of developing a greater risk of myocarditis in men are probably mediated by sex hormones. Molecular studies demonstrated that estrogens protected against myocarditis and prevented the apoptosis of cardiomyocytes, cardiac hypertrophy, and fibrosis.11 On the other hand, the pathogenesis of myocarditis is mostly considered to be immune‑mediated, while autoimmune diseases (as in our study) are much more prevalent in women. Conversely, experimental studies indicate that testosterone plays an important role in the development of myocarditis. Testosterone promotes viral replication12 and inhibits anti‑inflammatory cell groups.13 In addition, genetic variations and chromosome‑related factors may contribute to a variability in the incidence of myocarditis.14 One of the studies showed that genetic variations in desmosome structural proteins promoted myocardial seeding by pathogens.15
We also reported the highest rate of hospital admissions due to myocarditis between November and April. The incidence rate was the lowest in the summer and the spring. The difference was best shown in the male population and can be explained by the viral infection season during autumn and winter. Yet another study performed in Finland showed a similar regularity in the seasonal pattern of acute myocarditis. The incidence was the highest between September and December.16 Other authors reported that in the Korean population 50% of cases were reported between January and March.17 Notably, our study showed a higher prevalence of infections in women. Nevertheless, men are more susceptible to myocarditis; therefore, we can assume factors other than infections to be the reasons for the higher myocarditis incidence rate in men. Myocarditis may be of toxic or immune‑mediated origin.18
The presentation of myocarditis is inconsistent, ranging from mild symptoms, such as chest pain or palpitations linked with transient ECG changes, to life‑threatening cardiogenic shock and ventricular arrhythmia.1 In the current study, the men with myocarditis were more often admitted to cardiology wards. In contrast, women were usually admitted to general wards, and no difference was seen in admissions to intensive care units. Such a discrepancy in the type of the admission ward could be explained by the sex‑related difference in clinical manifestations of myocarditis. However, previous studies showed higher prevalence and severity of cardiovascular symptoms, including cardiogenic shock, in the course of myocarditis in women.6 On the other hand, a higher probability of hospitalization in cardiology wards for men may have resulted from the fact that cardiovascular diseases, that is, suspected myocarditis or acute coronary syndrome, are more common in men. Nevertheless, women should have an equal access to advanced cardiac diagnostics, so as not to delay the treatment for myocarditis.
It should also be mentioned that we documented a higher rate of cardiac arrhythmias, such as atrial fibrillation or ventricular tachycardia in women. Other authors also reported similar findings. Shah et al6 found more women with myocarditis suffering from ventricular fibrillation and cardiac arrhythmias during the same hospitalization. A higher occurrence of cardiogenic shock and longer or fluctuating QT interval during menstrual cycle in women may be a plausible reason for the arrhythmias.6 Interestingly, it was shown that testosterone could protect men from arrhythmias by shortening the action potential and decreasing K‑channel expression.19 Moreover, in age‑adjusted rate, women more often presented with heart failure, hypertension, diabetes, stroke, or transient ischemic attack, and other comorbidities on admission.
It should also be noted that the criteria for the diagnosis of myocarditis (as well as the access to advanced diagnostic procedures, that is, CMR and EMB) have changed over time, usually making the diagnosis of myocarditis a diagnosis of exclusion. Myocarditis should be confirmed with EMB, which is a gold standard for a definite diagnosis with current histological, immunohistochemical and molecular techniques. EMB is recommended in all patients with suspected myocarditis (particularly when there are signs of myocardial compromise, progressive or persistent severe cardiac dysfunction and / or life‑threatening ventricular arrhythmias, and / or advanced atrioventricular block with a lack of short‑term [<1–2 weeks] expected response to usual medical treatment), as it allows for providing an adequate disease‑specific treatment and monitoring of the therapy.3,20 However, EMB is still performed only in selected centers worldwide, and still not in all patients that would benefit from the procedure.
During the study period, the use of echocardiography, CMR and EMB in both the men and women was very low, showing that the implementation of the European Society of Cardiology criteria for the diagnosis of myocarditis in clinical practice was highly insufficient. Particularly more attention should be paid to the diagnosis of women with suspected myocarditis. Our study showed that the women aged 21–40 years, with clinically diagnosed myocarditis, had a poorer short- and long‑term prognosis than the corresponding men. Conversely, the 5‑year survival in men with myocarditis was the poorest in the patients aged 61–80 years. When analyzing the entire study group regardless of age, sex, and follow‑up time, the patients with clinically diagnosed myocarditis had a poorer prognosis than the age‑sex‑matched general population. What is more, short- and long‑term outcomes deteriorated with age in both sexes. In the patients with the biopsy‑proven myocarditis, the all‑cause mortality may rise to approximately 20% in a 5‑year follow‑up.21 Common predictors of the poorer prognosis include reduced left ventricular ejection fraction, symptomatic heart failure, ventricular arrhythmias, and specific etiologies of myocarditis (ie, virus‑positive, giant‑cell).3,22 Arrhythmias and underlying comorbidities in the women in our study may partially explain the observed poorer outcomes in this group. The presence of late gadolinium enhancement (LGE) in CMR is also a strong predictor of mortality and cardiovascular risk. The study demonstrated that midwall LGE in the (antero-) septal segments is related to higher incidence of death (including sudden cardiac death) in a >10‑year follow‑up period in the patients with the biopsy‑proven myocarditis.23 On the contrary, the predictors of good outcome included the absence of LGE, decreased LGE over time, LGE in the inferolateral wall, and preserved ejection fraction at baseline.24
Most of the study patients also required hospitalization during the 5‑year observation period. The rate of recurrent hospitalizations due to myocarditis was higher in men. On the other hand, women were admitted to a hospital for arrhythmias, heart failure, and autoimmune disorders. These results point out that not only the diagnosis but also the treatment of myocarditis require a significant improvement. The prognosis of patients with myocarditis may be improved with the disease‑directed treatment.3,25 It seems to be particularly important in light of the presented data on the increasing incidence of myocarditis in the last decade. The data obtained from this nationwide database clearly demonstrate that myocarditis constitutes an emerging challenge for the health care system and decisive steps need to be taken to stimulate further research in the field.
Limitations
The inclusion of real‑life patients allowing for populational analyses is an important advantage of this nationwide database; however, there are several limitations that must be acknowledged. The medical history of the patients was limited to 400 days prior to inclusion in the study, because the database was established in 2009. Moreover, ICD‑9 and ICD‑10 coding errors, misclassifications and incompleteness of data cannot be excluded. As mentioned above, due to the nature of the database (based on ICD‑9 and ICD‑10 codes extracted from the national health care payer) and international clinical practice, the diagnosis of myocarditis was mostly not confirmed by EMB or autopsy (a diagnostic gold standard), and could not be verified. However, this is in line with worldwide data, showing that EMB is still performed only in selected centers, in the minority of patients, and requires significant improvement.
Conclusions
The incidence of myocarditis was age-, sex-, and season‑dependent. Significant improvement is required in the management of myocarditis, including the initial diagnostic process, as well as short- and long‑term therapy, particularly in women. The use of recommended procedures (echocardiography, CMR and EMB) was very low.
- Caforio AL, Pankuweit S, Arbustini E, et al. Current state of knowledge on aetiology, diagnosis, management, and therapy of myocarditis: a position statement of the European Society of Cardiology Working Group on Myocardial and Pericardial Diseases. Eur Heart J. 2013; 34: 2636‑2648. | Crossref
- Ozieranski K, Tyminska A, Kruk M, et al. Occurrence, trends, management and outcomes of patients hospitalized with clinically suspected myocarditis‑ten‑year perspectives from the MYO‑PL Nationwide Database. J Clin Med. 2021; 10: 4672. | Crossref
- Tyminska A, Ozieranski K, Caforio ALP, et al. Myocarditis and inflammatory cardiomyopathy in 2021: an update. Pol Arch Intern Med. 2021; 131: 594‑606. | Crossref
- Ozieranski K, Tyminska A, Jonik S, et al. Clinically suspected myocarditis in the course of severe acute respiratory syndrome novel coronavirus‑2 infection: fact or fiction? J Card Fail. 2021; 27: 92‑96. | Crossref
- Ozieranski K, Tyminska A, Caforio ALP. Clinically suspected myocarditis in the course of coronavirus infection. Eur Heart J. 2020; 41: 2118‑2119. | Crossref
ARTICLE INFORMATION