The role of endoscopic and demographic features in the diagnosis of gastric precancerous conditions
Key words: atrophic gastritis, esophagogastro-duodenoscopy, gastric cancer, gastritis, intestinal metaplasia



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
The role of endoscopic and demographic features in the diagnosis of gastric precancerous conditions
Introduction: The diagnosis of atrophic gastritis (AG) and intestinal metaplasia (IM) is a crucial screening and surveillance strategy for gastric adenocarcinoma.
Objectives: The main objective was to assess the performance of endoscopic diagnosis of gastric precancerous conditions in a real‑life scenario.
Patients and methods: A total of 2099 gastroscopies with biopsy to evaluate gastritis performed in 3 endoscopic centers from March 2018 to October 2019 were retrospectively analyzed. Endoscopic data regarding gastritis, atrophy, and intestinal metaplasia were compared with histopathological reports.
Results: The endoscopic diagnosis sensitivity was 69.5% for AG and 19.4% for IM. The specificity of endoscopic detection of AG was 69.5% and of IM, 97.9%. The endoscopic detection of gastritis was a risk factor for AG and IM diagnosis (odds ratio [OR], 5.1; 95% CI, 1.9–14.1 and OR, 14.5; 95% CI, 5.9–35.8, respectively) and the patient’s age was a risk factor for AG, IM, dysplasia, and advanced stage of AG (ASAG) diagnosis (OR, 1.05; 95% CI, 1.04–1.06; OR, 1.035; 95% CI, 1.03–1.04; OR, 1.04; 95% CI, 1.02–1.06; and OR, 1.05; 95% CI, 1.02–1.09, respectively). The age threshold of 45 or 40 years with endoscopically diagnosed gastritis for obtaining biopsy would result in 96.3% and 95% ASAG or dysplasia diagnosis sensitivity, and in the reduction of the number of biopsies by 20.2% and 20.5%, respectively.
Conclusions: The application of the age threshold with or without an endoscopic diagnosis of gastritis could reduce the number of mapping biopsies to detect advanced stages of atrophic gastritis or dysplasia with high sensitivity.
What's new?
The diagnosis of atrophic gastritis (AG) and intestinal metaplasia (IM) is a crucial factor in the surveillance strategy of gastric cancer. Endoscopic visualization of AG and IM is not yet recommended as the sole diagnosis; however, some data indicate that it could have high accuracy. Mapping biopsy is the gold standard for diagnosing AG and IM, which results in an increased number of biopsies. We found out that endoscopic diagnosis of AG and IM is insufficient to replace the biopsy in a real‑life scenario. Age and endoscopic diagnosis of gastritis are the risk factors for AG, IM, and dysplasia diagnosis. Applying the age criteria with or without an endoscopic diagnosis of gastritis reduces the number of biopsies without significant effect on the diagnosis of AG and IM.
Introduction
Gastric cancer remains a significant health problem, ranking in the top 3 reasons for cancer‑related deaths worldwide.1 Intestinal type gastric cancer according to Lauren classification may develop in a multistep process from gastric precancerous conditions (GPC), such as atrophic gastritis (AG) and intestinal metaplasia (IM) in “Correa cascade.”2,3 Detection of AG and IM may be vital for the risk stratification of gastric cancer development and for indication of the starting point for surveillance programs to detect early lesions that could be treated endoscopically. Such surveillance programs for patients with extensive AG and IM may be cost‑effective even in countries with a moderate prevalence of gastric cancer.4 Accurate endoscopic diagnosis correlating with histopathology reports would be warranted. However, endoscopy is believed to have low sensitivity in the diagnosis of GPC.5,6 The advent of the high definition (HD) era in endoscopy imaging with the use of virtual chromoendoscopy techniques such as narrow‑band imaging (NBI) has significantly enhanced endoscopy performance.7-12 Despite the growing significance of the endoscopic diagnosis, a biopsy is still the standard procedure for the detection of GPC, indispensable in the diagnosis of dysplasia.13 Our study aimed to assess the performance of endoscopic diagnosis of GPC in a real‑life scenario.
Patients and methods
Study design
It was a multicenter, retrospective study in which 2099 patients underwent a complete diagnostic gastroscopy between March 2018 and October 2019, with biopsy samples taken for histopathological evaluation of gastritis. The patients whose examination was incomplete due to previous surgeries, intolerance, inappropriate preparation, or particular anatomical conditions were excluded. In 3 separate endoscopy units, the collected data included the patient’s age and sex, the endoscope type, sedation, inpatient or outpatient setting of the endoscopy, and indication for this examination. Imaging endoscopic data included the presence of gastritis, mucosal atrophy, gastric intestinal metaplasia, and their extent, as well as the location of the biopsies. In addition, data on the presence of a gastric ulcer, polyp, or tumor were recorded. Helicobacter pylori infection was diagnosed when a rapid urease test was positive or detected during a histopathological examination. All examinations were performed with the Olympus Exera III system using GIF‑Q165, GIF‑Q180, GIF‑H180J, and GIF‑HQ190 endoscopes (Hamburg, Germany).
Gastric specimens from all endoscopy units were sent to 3 different histopathological laboratories. Data on the presence and severity of AG, IM, and dysplasia were collected based on histopathological work‑up. Operative links for gastritis assessment (OLGA) and IM assessment (OLGIM) were calculated based on the histopathological reports.14,15 AG of at least a moderate degree in both the corpus and antrum, and IM in both the corpus and antrum, OLGA/OLGIM III/IV were considered advanced stages of AG according to MAPS II guidelines.13 To assess the advanced stages of AG, only examinations with biopsies obtained from the corpus and antrum to separate the containers were evaluated. The gastroscopies with the biopsies obtained from the corpus and antrum to the same container were only evaluated for global IM and AG detection performance. The procedures in which the samples were taken from the corpus or antrum were evaluated for global AG and IM detection and their detection in the corpus or antrum, respectively. The study was conducted with the ethical review board approval (PCN/022/KB/40/21).
Statistical analysis
Qualitative features were presented as frequencies and percentages. Quantitative features were characterized with the mean value and SD. Median and interquartile range (IQR) were applied if a nonparametric test was performed to compare quantitative features in each group. The Shapiro–Wilk test determined, if the quantitative data were normally distributed. The Levene test was used to verify the homogeneity of variance. The ANOVA or the Kruskal–Wallis test with multiple comparisons compared features between more than 2 groups.
Multivariable logistic regression models were computed to determine how selected risk factors, such as age, male sex, use of a HD instrument, outpatient procedure setting, use of sedation, the occurrence of gastritis, gastric polyps, gastric ulcer, influence the odds of occurrence of AG, IM, dysplasia, and advanced stage of AG. The results were reported as odds ratio (OR) with 95% CI.
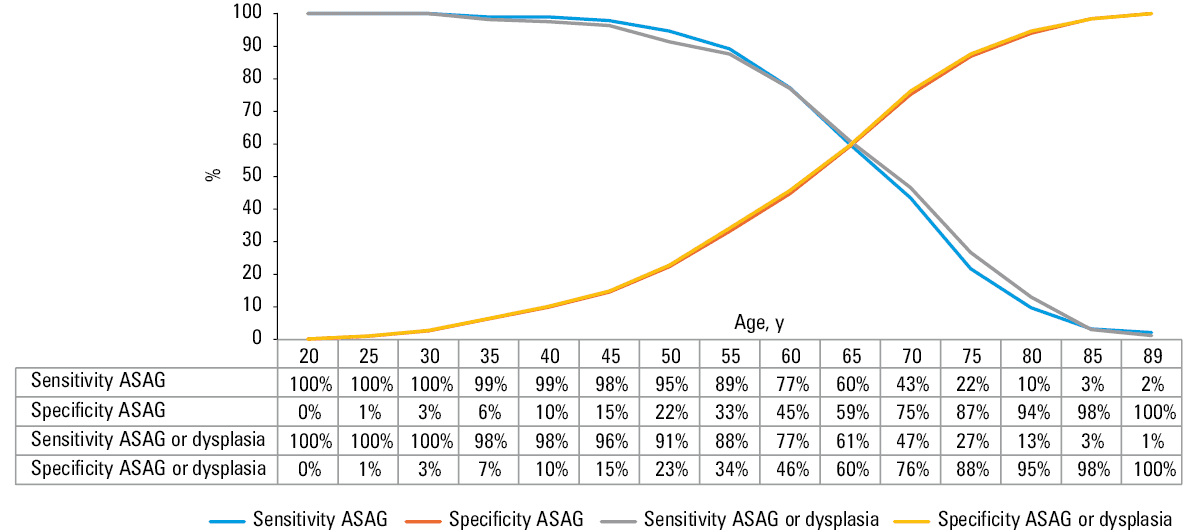
The efficiency of endoscopic diagnosis of GPC and advanced stage of AG were reported as sensitivity, specificity, accuracy, positive / negative likelihood ratio, and positive / negative predictive value. Receiver operating characteristic (ROC) curves and area under the curves were derived. The association between age and corresponding sensitivity, as well as specificity values of advanced stages of atrophic gastritis and dysplasia was generated. The sensitivity of detection of advanced stages of atrophic gastritis and dysplasia was calculated for age groups of 40, 45, 50, and 55 years with or without endoscopic detection of gastritis during the procedure. A potential reduction in the number of biopsies was calculated as the number of the patients in the study from whom the biopsies would not be obtained due to age or age and endoscopic detection of gastritis criteria that were not met.
A P value below 0.05 was considered significant. The collected data were grouped on Microsoft Excel spreadsheets and analyzed with STATISTICA v.13.1 (StatSoft Inc., Tulsa, Oklahoma, United States) for Windows.
Results
General data
Based on histopathological reports of 2099 patients, AG, IM, and dysplasia were diagnosed in 262 (12.5%), 660 (31.4%), and 85 (4%) patients, respectively. The mean age of the patients was 59 years, and 59% were women. Seventy percent of EGDs were conducted as outpatient procedures, and 31.6% were performed under sedation. HD endoscopes were used in 47.6% of the procedures. The endoscopic data are summarized in Table 1. Of 85 patients identified with dysplasia, 79 were classified as low‑grade dysplasia, 1 as high‑grade dysplasia, and 5 as indefinite dysplasia.
Parameter | Value |
Abbreviations: HD, high‑definition | |
Demographic data | |
Patients, n | 2099 |
Age, y, mean (SD) | 59 (15.45) |
Men / women, n | 860/1239 |
Indication for endoscopy, n (%) | |
Malignancy suspicion | 220 (10.5) |
Gastroesophageal reflux disease | 182 (8.7) |
Dyspepsia | 176 (8.4) |
Malabsorption | 164 (7.8) |
Follow‑up of gastritis | 134 (6.4) |
Follow‑up of peptic ulcer | 59 (2.8) |
Other | 1164 (55.5) |
Endoscopic data | |
Sedation, n (%) | 663 (31.6) |
HD / non‑HD endoscopes, n | 999/1100 |
Inpatient / outpatient, n | 630/1469 |
Helicobacter pylori infection, n (%) | 418 (19.9) |
Endoscopic diagnosis, n (%) | |
Gastritis | 1940 (92.4) |
Mucosal atrophy | 743 (35.4) |
Intestinal metaplasia | 159 (7.6) |
Gastric polyps | 285 (13.6) |
Gastric ulcer | 39 (1.9) |
Gastric cancer | 9 (0.4) |
Histopathological data, n (%) | |
Patients with biopsy from the corpus and antrum because of gastritis | 657 (31.3) |
Atrophic gastritis | 262 (12.5) |
Intestinal metaplasia | 660 (31.4) |
Atrophic gastritis or intestinal metaplasia | 118 (18) |
Dysplasia | 85 (4) |
Endoscopic diagnosis of atrophic gastritis and intestinal metaplasia
While atrophy was diagnosed during EGD in 35.4% of all patients, in the histopathological examination AG was diagnosed in 12.5% of all patients. Out of 262 patients with histopathological diagnosis of AG, endoscopy detected this pathology in 182 patients. Contrary to that, IM was endoscopically diagnosed in 7.6% of all patients, while it was found in 31.4% of all patients on the histopathological examination. Of 660 patients with histopathologically diagnosed IM, in only 128 it could be detected by the endoscopy. Both the sensitivity and specificity of endoscopic diagnosis of AG were 69.5%, while the sensitivity of endoscopy to detect IM was much lower, that is, 19.4% with a high specificity of 97.9% (Table 2). The diagnostic accuracy of AG and IM detection in the antrum was higher than in the corpus of the stomach. The sensitivity, specificity, and accuracy of GPC was 55%, 76.9%, and 68.5% in the examinations performed with non‑HD instruments, and 61.5%, 65.3%, and 64% with HD endoscopes.
Endoscopic findings | Sensitivity | Specificity | Accuracy | LR+ | LR– | PPV | NPV | |
Abbreviations: LR+, positive likelihood ratio; LR–, negative likelihood ratio; NPV, negative predictive value; PPV, positive predictive value | ||||||||
Endoscopic diagnosis of gastric precancerous conditions | ||||||||
Atrophy | Total | 0.695 | 0.695 | 0.695 | 2.28 | 0.44 | 0.245 | 0.941 |
Antrum | 0.633 | 0.74 | 0.728 | 2.43 | 0.50 | 0.231 | 0.942 | |
Corpus | 0.614 | 0.773 | 0.755 | 2.705 | 0.499 | 0.258 | 0.940 | |
Intestinal metaplasia | Total | 0.194 | 0.979 | 0.732 | 9.24 | 0.82 | 0.805 | 0.726 |
Antrum | 0.207 | 0.973 | 0.744 | 7.61 | 0.82 | 0.764 | 0.743 | |
Corpus | 0.127 | 0.973 | 0.808 | 4.704 | 0.897 | 0.529 | 0.822 | |
Endoscopic diagnosis of advanced stages of atrophic gastritis | ||||||||
Atrophy or intestinal metaplasia | 0.703 | 0.559 | 0.579 | 1.59 | 0.53 | 0.201 | 0.923 | |
Atrophy | 0.593 | 0.604 | 0.602 | 1.497 | 0.674 | 0.194 | 0.902 | |
Intestinal metaplasia | 0.242 | 0.913 | 0.820 | 2.782 | 0.830 | 0.310 | 0.882 | |
Accuracy of endoscopic diagnosis of gastric precancerous conditions in patients with histologically proven advanced stage of atrophic gastritis
Ninety‑one of the patients were diagnosed with an advanced stage of AG (13.9% of patients whose biopsies were obtained from both the corpus and the antrum). Among them, gastritis was diagnosed during endoscopy in 89 patients, and AG or IM was suspected in 64 patients (70% sensitivity, 55.9% specificity) (Table 2).
Risk factors for histopathological diagnosis of gastric precancerous conditions and dysplasia
Dysplastic foci were found in the histopathological specimens in 85 patients. Based on the endoscopy, 82 patients were diagnosed with gastritis, and AG or IM was recognized in 55 patients.
In the multivariable logistic regression, the patient’s age and endoscopic diagnosis of gastritis were the risk factors for the occurrence of both AG and IM. The outpatient procedure was a risk factor for AG diagnosis but at the same time an opposite risk factor for IM diagnosis. Sedation during the procedure was an opposite risk factor for AG and IM diagnosis. Performing EGD with a HD endoscope was a risk factor for AG diagnosis without any influence on the detection of IM, dysplasia, and advanced stage of AG. Age was the only risk factor for an advanced stage of AG and dysplasia (Table 3).
Diagnosisa | Statistical variables | Demographic and procedure variables | Endoscopic diagnosis | ||||||
Age | Sex (M) | HD endoscope | Outpatient | Sedation | Gastritis | Polyp | Ulcer | ||
Values were considered significant at P <0.05.
a The diagnoses were established based on histopathological report.
Abbreviations: AG, atrophic gastritis; ASAG, advanced stages of atrophic gastritis; IM, intestinal metaplasia; M, male; OR, odds ratio; polyp, gastric polyp; ulcer, gastric ulcer; others, see Table 1 | |||||||||
AG | OR | 1.05 | 1.23 | 1.27 | 1.48 | 0.71 | 5.09 | 0.99 | 0.81 |
95% CI | 1.04–1.06 | 0.87–1.61 | 1.0–1.67 | 1.09–2.13 | 0.51–0.88 | 1.86–14.12 | 0.72–1.37 | 0.34–2.25 | |
P value | <0.001 | 0.17 | 0.043 | 0.006 | 0.015 | 0.002 | 0.96 | 0.69 | |
IM | OR | 1.04 | 1.34 | 0.91 | 0.72 | 0.67 | 14.5 | 1.21 | 0.8 |
95% CI | 1.03–1.04 | 1.05–1.63 | 0.78–1.13 | 0.59–0.91 | 0.48–0.84 | 5.86–35.77 | 0.87–1.53 | 0.39–1.84 | |
P value | <0.001 | 0.02 | 0.49 | 0.006 | <0.001 | <0.001 | 0.29 | 0.65 | |
Dysplasia | OR | 1.04 | 1.54 | 0.78 | 0.64 | 0.60 | 1.89 | 0.69 | 0.58 |
95% CI | 1.02–1.06 | 0.99–2.39 | 0.49–1.23 | 0.40–1.00 | 0.35–1.03 | 0.58–6.14 | 0.34–1.41 | 0.08–4.23 | |
P value | <0.001 | 0.06 | 0.28 | 0.05 | 0.06 | 0.28 | 0.30 | 0.60 | |
ASAG | OR | 1.05 | 1.78 | 0.86 | 1.77 | 0.36 | 0.13 | 1.36 | 18.76 |
95% CI | 1.02–1.09 | 0.79–4.02 | 0.38–1.94 | 0.66–4.77 | 0.09–1.29 | 0.02–1.00 | 0.51–3.61 | 0.78–449.15 | |
P value | 0.003 | 0.16 | 0.70 | 0.25 | 0.12 | 0.05 | 0.54 | 0.06 | |
Age and endoscopic diagnosis of gastritis as conditions for biopsy to evaluate gastric precancerous conditions
Patients with biopsies obtained from the corpus and antrum were divided into 5 groups: (1) advanced stage of AG, (2) dysplasia, (3) GPC in the corpus and antrum classified as nonadvanced AG, (4) GPC in the corpus or antrum, (5) patients without GPC and dysplasia. The median (IQR) age of patients was 66 (60–73), 70 (62–78), 67 (60–79), 63 (53–71), and 58 (49–68) years for groups 1 to 5, respectively. The age of the patients in the group 5 was significantly lower than in the other groups, and the age of the patients in the group 4 was significantly lower than in group 2 (P <0.05).
The ROC curve analysis was performed to assess the targeted age group for a biopsy to evaluate GPC. The area under the ROC curve for age according to advanced stages of gastritis was 0.647 and 0.663, including patients with dysplasia (Figure 1). The highest Youden score for advanced stages of AG was achieved for patients aged 56 years (0.254), and for advanced stages of AG or dysplasia for patients aged 62 years (0.266).
Abbreviations: see Table 3
As endoscopically diagnosed gastritis was another risk factor for detecting AG and IM, we analyzed the diagnostic significance of the combination of age and gastritis. The age threshold of 45 or 40 years and finding of gastritis resulted in at least 95% sensitivity for the diagnosis of advanced stage of AG or dysplasia, with a 20% reduction in the number of patients with biopsies. These data are summarized in Table 4.
Age as prerequisite for biopsy | ||||
Years | 40 | 45 | 50 | 55 |
Sensitivity for advanced stage of atrophic gastritis, % | 98.9 | 97.8 | 94.6 | 89.1 |
Sensitivity for advanced stage of atrophic gastritis and dysplasia, % | 97.5 | 96.3 | 91.3 | 87.6 |
Potential reduction in the number of biopsies, n (%) | 297 (14.1) | 423 (20.2) | 590 (28.1) | 787 (37.5) |
Gastritis and age as prerequisites for biopsy | ||||
Years | 40 | 45 | 50 | 55 |
Sensitivity for advanced stage of atrophic gastritis, % | 97.8 | 96.7% | 93.4 | 87.9 |
Sensitivity for advanced stage of atrophic gastritis and dysplasia, % | 95 | 93.8 | 88.2 | 84.5 |
Potential reduction in the number of biopsies, n (%) | 430 (20.5) | 543 (25.9) | 696 (33.2) | 827 (39.4) |
Discussion
The idea of endoscopic diagnosis of AG emerged over 50 years ago.16 Along with the access to different endoscopic techniques, such as chromoendoscopy, the accuracy of GPC detection has increased.17 Moreover, technological improvements such as HD, magnification, and virtual chromoendoscopy yielded promising results on the efficiency of endoscopic diagnosis in recognizing GPC.7-12 Endoscopic diagnosis of atrophy was identified as a risk factor for gastric cancer development,18,19 however, AG was diagnosed post‑hoc and not during an endoscopic examination in previous studies. It is also known that the endoscopic diagnosis of GPC depends on the operator’s performance and training.20,21
Various guidelines regarding precancerous conditions in the stomach have been published so far.13,22,23 Depending on the geographical diversity of gastric cancer prevalence, different recommendations regarding screening for GPC were suggested,24 however, the histopathological confirmation of GPC is still a mainstay of the surveillance strategy.13,22,23 The goal of our study was to determine whether the endoscopic diagnosis of GPC is adequate for obtaining biopsy only if AG or IM are diagnosed endoscopically. This kind of approach is suggested by the British Society of Gastroenterology guidelines.22
In our study, the sensitivity of endoscopic diagnosis of AG was comparable to other studies.6,24 Although specificity of AG detection in other studies varied significantly, it was generally similar to our results.6,24,25 As in other studies, we found that the endoscopic diagnosis of IM is characterized by low sensitivity and high specificity.5 In certain studies, virtual chromoendoscopy, such as NBI provided promising results regarding the endoscopic diagnosis of IM.8-10,12 However, we did not find a relationship between the use of HD endoscopes equipped with NBI and the detection rate of IM. Nevertheless, due to the retrospective design of our study, examining the impact of NBI on GPC diagnosis may be flawed. Also, HD instruments surprisingly did not improve the accuracy of GPC diagnosis and were marked with higher sensitivity but lower specificity than non‑HD endoscopes.
It is known that the prevalence of GPC is higher in the older population.26 Eshmuratov et al24 reported lower AG prevalence in people under 50 years, and in this population, the endoscopic sensitivity of AG detection was also lower than in the older one. Not only AG but also IM prevalence was shown to increase with age.5 Accordingly, our patients with GPC were older than the patients without mucosal lesions. Lower AG and IM prevalence in younger patients could be explained by the extended time necessary to develop AG during H. pylori infection. We agree with the opinion that obtaining blind biopsies in younger patients would not provide clinically relevant information because of the low prevalence of GPC.
We found that any recognizable endoscopic sign of gastritis may result in high sensitivity of GPC detection. However, endoscopic diagnosis of gastritis was not a risk factor for advanced stage of AG in our study. This might be due to high participation of patients with gastritis (651 of 657 patients in whom biopsies were obtained from the corpus and antrum).
In our study, the prevalence of IM was higher than in a Turkish study26 and in over 100 studies performed in different geographic regions evaluated in a meta‑analysis.27 In contrast to IM, the prevalence of AG in our study was clearly lower than in this meta‑analysis.27 The higher number of patients with IM and lower number of individuals with AG may be explained by a moderate to high prevalence of H. pylori reported in Poland in previous decades and a longer time needed for regression of IM than AG after eradication treatment.28,29 On the other hand, the prevalence of GPC localized in both the corpus and antrum was comparable to other studies.26 Dysplasia was present in 4% of all patients and was not detected endoscopically. In contrast to other data, male sex was not a risk factor for GPC or dysplasia diagnosis in our study.26 The incidence of H. pylori infection was significantly lower in our study than in the Polish data from earlier years.28 Our knowledge of the real significance of H. pylori infection for GPC risk could be restricted by an unknown history of proton pump inhibitors use or recent antibiotic treatment. However, the low prevalence of H. pylori infection in our cohort is consistent with the sharply decreasing prevalence of this infection in our country.30,31 This finding suggests that GPC prevalence will also show a decreasing tendency in our country in the coming years. Therefore, searching for adequate risk stratification without a high number of true negative biopsies is highly justified.
Limitations and conclusions
The main limitation of our study is its retrospective design. For this reason, we could not evaluate AG and IM in relation to clinical data and family history. We were also unable to evaluate the significance of using NBI for the diagnostic performance of endoscopy. Also, we could not evaluate either the exact anatomical locations where the biopsies were collected or the number of specimens.
In conclusion, the endoscopic diagnosis of GPC is still not adequate and insufficient to replace histology in a real‑life scenario, as it provides too many false positive and negative results. However, the number of mapping biopsies may be reduced in patients younger than 45 years or younger than 40 years and without an endoscopic diagnosis of gastritis.
- Bray F, Ferlay J, Soerjomataram I, et al. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018; 68: 394‑424. | Crossref
- Correa P. Human gastric carcinogenesis: a multistep and multifactorial process ‑ first American Cancer Society award lecture on cancer epidemiology and prevention. Cancer Res. 1992; 52: 6735‑6740.
- Lauren P. The two histological main types of gastric carcinoma: diffuse and so‑called intestinal‑type carcinoma. An attempt at a histo‑clinical classification. Acta Pathol Microbiol Scand. 1965; 64: 31‑49. | Crossref
- Areia M, Dinis‑Ribeiro M, Rocha Gonçalves F. Cost‑utility analysis of endoscopic surveillance of patients with gastric premalignant conditions. Helicobacter. 2014; 19: 425‑436. | Crossref
- Lim JH, Kim N, Lee HS, et al. Correlation between endoscopic and histological diagnoses of gastric intestinal metaplasia. Gut Liver. 2013; 7: 41‑50. | Crossref
ARTICLE INFORMATION