Association between the acquisition of antibodies against Lyme disease and the risk of atrial arrhythmias
Key words: atrial arrhythmia, atrial fibrillation, Lyme antibodies, Lyme carditis, Lyme disease



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Association between the acquisition of antibodies against Lyme disease and the risk of atrial arrhythmias
Introduction: The impact of antibodies against Borrelia burgdorferi (BB) on the occurrence of cardiac arrhythmias in patients without typical symptoms of Lyme disease (LD) is largely unknown.
Objectives: We aimed to assess the risk of atrial fibrillation (AF) and other atrial arrhythmias (AAs) in patients who tested positive for anti‑LD antibodies.
Patients and methods: We included consecutive patients referred for the diagnosis and treatment of AAs who had no history of erythema migrans or other symptoms of LD. The presence of anti‑BB antibodies (immunoglobulin [Ig] M and IgG) was assessed in each patient, and the diagnostic workup of cardiac arrhythmias was performed.
Results: Of the 527 patients enrolled in the study, 292 (55%) were diagnosed with AAs, and we detected BB antibodies in 131 individuals (24.8%). The patients with a serological history of Borrelia infection were older (mean [SD], 55.6 [15.7] vs 50.3 [18.6] years; P = 0.01), had a higher probability of developing AF or other supraventricular arrhythmias (SAs) (66.4% vs 51.8%; P = 0.03), and had elevated levels of N‑terminal pro–B‑type natriuretic peptide (NT‑proBNP) (58% vs 47.5%; P = 0.04). We also found an association between the occurrence of AF and other SAs in patients with anti‑BB antibodies and elevated NT‑proBNP values, and the risk of AAs in these patients increased almost 3‑fold (P = 0.01).
Conclusions: Our data indicated an association between the exposure to Borrelia infection and the risk for AF and other AAs in the patients with elevated levels of NT‑proBNP, suggesting the need for a more efficacious diagnostic approach to patients with SAs, especially in LD‑endemic regions.
What's new?
Little is known about the serological history of Borrelia infection and its impact on the cardiovascular system, including the development of cardiac arrhythmias. In this study, we assessed whether patients with antibodies against Lyme disease and with elevated levels of N‑terminal pro–B‑type natriuretic peptide are at an increased risk for atrial fibrillation and other supraventricular arrhythmias. We were able to determine that patients with antibodies against Lyme disease were at a greater risk for atrial arrhythmias, even if they had no history of typical Lyme disease symptoms.
Introduction
Lyme disease (LD), caused by a group of spirochetes classified as Borrelia burgdorferi (BB), is the most prevalent tick‑borne illness in the northern hemisphere.1 The entire country of Poland is regarded as an endemic region for BB, with approximately 8000 to 9000 new cases reported annually.2 Lyme carditis (LC) can be recognized in 1% of untreated patients at an early stage.2 LD can lead to cardiac complications, with conduction disturbances, myocarditis, and pericarditis being the most commonly described. It was hypothesized that LD may also cause dilated cardiomyopathy and heart failure in endemic areas.1 Intraventricular blocks or supraventricular arrhythmias (SAs) and ventricular arrhythmias occur much less frequently in patients with LD.3 Importantly, in some cases, LC can be associated with a skin rash, neurological symptoms, or arthritis, while in others, it is the only manifestation of LD. In these cases, clinical symptoms include syncope, light‑headedness, fainting, shortness of breath, palpitations, and chest pain. Moreover, a large number of patients may be asymptomatic.4 An epidemiological study assessing the prevalence of Borrelia infection in patients with atrial fibrillation (AF) focused on immunoglobulin G (IgG) levels.5
Cardiac manifestations of LC can occur after a median of 21 days from tick exposure.6 The most common clinical feature of LC is transient atrioventricular (AV) block (90%), occurring mainly above the His bundle.6,7 The true incidence of LC may be underestimated as case reports documented abnormalities ranging from first‑degree heart block to myocarditis and acute heart failure.8-10
AV nodal block and slow ventricular response to atrial rhythm can suggest conduction disease within the AV junction. The macro- and microreentrant arrhythmias of the atrium, including atrial flutter (AFL), atrial tachycardia (AT), and AF, most likely develop due to left atrial enlargement and mitral regurgitation or may represent a more widespread conduction disease and suggest simultaneous conduction abnormalities of various etiologies.11
The exact pathophysiological mechanism has not been fully elucidated; however, it is considered that AV block occurs due to the host inflammatory response to the presence of bacteria in the cardiac tissue.4,10,12 The clinical course of LC is generally mild, short‑term, and, in most cases, completely reversible after adequate antibiotic treatment.4
Symptoms of LD can be attributable to residual inflammation in and around tissues that harbor a low burden of persistent host‑adapted spirochetes and / or residual antigens.13 This also explains the decreased efficacy of antibiotic treatment in LD, which may be due to several causes, including inflammatory responses to residual antigens from dead organisms, residual tissue damage after pathogen clearance, and autoimmune responses, possibly elicited by antigenic mimicry.4,13-16 The aim of the study was to determine whether the presence of BB antibodies can increase the risk for AF and other SAs independently or with another trigger. We focused on the dependence of arrhythmia on the level of N‑terminal pro–B‑type natriuretic peptide (NT‑proBNP).
Patients and methods
This study was conducted in a group of 630 patients who were hospitalized in the 1st Department of Heart Rhythm Disorders of the National Institute of Cardiology in Warsaw, Poland, from March 1, 2010 to February 28, 2011, without a history of erythema migrans or other overt symptoms of BB infection, and without a history of LD treatment during the diagnostic workup of cardiac arrhythmias. We excluded 103 patients with acute heart failure, symptomatic coronary heart disease, valves requiring a restorative procedure, and oncological, thyroid, or chronic inflammatory disease, which may be independent factors contributing to the onset of AF. Individuals with a prior cardiosurgical valve replacement were also excluded. Potential predictors of AF, including age, hypertension, and heart failure, were chosen based on a comprehensive review of the literature.
Each patient admitted to our department underwent evaluation of their immunoglobulin M (IgM) and IgG antibodies against BB, as determined by enzyme‑linked immunosorbent assay (ELISA). BB antibodies were detected in 131 patients (24.8%). Atrial arrhythmias (AAs), including AF, AFL, AT, and atrial premature beats (APBs), were diagnosed in 292 patients (55%). It is important to note that the patients treated in our department were referred for arrhythmia ablation, pacing system implantation, or modification of antiarrhythmic treatment. The diagnosis of cardiac arrhythmias was made based on available medical records, including medical history and tests performed during hospitalization. The set of extracted variables included demographic data, medical history, physical examination, resting electrocardiogram (ECG), and routine transthoracic echocardiography. All diagnoses of cardiac arrhythmias were confirmed with at least a single 24‑hour Holter ECG monitoring record before hospitalization, as well as with 24‑hour Holter ECG and telemetry monitoring records during hospitalization. APBs were taken into account if their number exceeded 10 000 beats per day. Patients with hypertension were defined as those who were treated for hypertension during hospitalization or who had previously been admitted to the hospital for this treatment. The study protocol was approved by the ethics committee of our institute.
Diagnosis
All patients underwent laboratory examinations, including measurement of IgG and IgM anti‑BB antibodies and NT‑proBNP level, 12‑lead ECG, and transthoracic echocardiography as part of routine diagnostic workup at our department. A positive anti‑BB antibody level was defined as a value greater than 22 RU/ml. The NT‑proBNP level was considered elevated when it exceeded 125 pg/ml.
Serological tests are fast, easy to perform, and especially suitable for diagnosing LC without erythema migrans. The most commonly used immunoassays are ELISA, immunofluorescence assays, and western blot assays. These assays are designed to detect the presence of IgM and IgG antibodies against BB in serum. ELISA, as a more reliable screening assay than immunofluorescence assays, is recommended as the initial serological examination for the diagnosis of LD.4
Statistical analysis
Continuous variables were reported as mean (SD) or median and interquartile ranges. Between‑group comparisons were performed using the t test or the nonparametric Mann–Whitney test. Normality was assessed using the Shapiro–Wilk test. Categorical variables were reported as numbers and percentages. The χ2 test was used to compare dichotomous variables, and the Cochran–Mantel–Haenszel test was used to compare ordinal variables. Odds ratios (ORs) with 95% CIs for patients with and without arrhythmias were calculated for demographic, clinical, and LD indicators. The homogeneity of the ORs in the subgroups was verified using the Breslow–Day test. A backward multivariable logistic regression analysis was performed to establish the relationship between the patients’ characteristics and the occurrence of APB/AF/AT. Interaction was also tested. We investigated the association between IgG, IgM, sex, hypertension, heart failure, age (≥65 vs <65 years), and NT‑proBNP level (≤125 vs >125 pg/l). A significance level of 0.05 was required for a variable to stay in the model. The Hosmer and Lemeshow goodness‑of‑fit test and percent concordant were calculated. A 2‑sided P value below 0.05 was considered significant. All analyses were performed using SAS statistical software, version 9.4 (SAS Institute, Inc., Cary, North Carolina, United States).
All the patients had access to information about their ELISA anti‑BB antibody test results, and those with levels that exceeded 22 RU/ml were provided with infectious disease counseling.
Results
Of the 630 patients admitted for the treatment of arrhythmias, a total of 527 were included in the final analysis (Table 1). Among them, 49.9% had AF, 50.1% had elevated NT‑proBNP levels, and 43.6% had hypertension. Anti‑BB antibodies were detected in 131 patients (24.9%). There were differences between the groups with and without anti‑BB antibodies. Those with anti‑BB antibodies were older (mean [SD], 55.6 [15.7] vs 50.3 [18.6] years; P = 0.001), more often had AF (60.3% vs 46.5%; P = 0.01) as well as AAs (66.4% vs 51.8%; P = 0.03), and had elevated NT‑proBNP levels (58.0% vs 47.5%; P = 0.04). Moreover, patients diagnosed with AF and other SAs (Table 2) were older (mean [SD], 58.1 [14.7] vs 43.5 [18.7] years; P <0.001) and more of them had hypertension (56.5% vs 27.7%; P <0.001); they also had a larger left atrium (mean [SD], 43.1 [6.8] vs 36.4 [6.8] mm; P <0.001), thicker ventricular septum on echocardiogram (mean [SD], 11.2 [2.0] vs 10.2 [2.0] mm; P <0.001), and more often had elevated levels of NT‑proBNP (65.8% vs 30.6%; P <0.001), and anti‑BB antibodies (29.8% vs 18.7%; P = 0.003).
Parameter | Total (n = 527) | Borrelia (+) (n = 131) | Borrelia (–) (n = 396) | P value |
Data are presented as median (interquartile range) or mean (SD) unless indicated otherwise.
Abbreviations: AF, atrial fibrillation; APB, atrial premature beats; AT, atrial tachycardia; AVNRT, atrioventricular nodal reentry tachycardia; BAC, bradyarrhythmias and conduction blocks; EF, ejection fraction; ICD, implantable cardioverter defibrillator; IVS, intraventricular septum; LA, left atrium; LV, left ventricle; NT‑proBNP, N‑terminal pro–B‑type natriuretic peptide; VEBs, ventricular ectopic beats | ||||
AF, n (%) | 263 (49.9) | 79 (60.3) | 184 (46.5) | 0.01 |
ABP/AT, n (%) | 49 (9.3) | 17 (13.0) | 32 (8.1) | 0.09 |
APB+AT+AF, n (%) | 292 (55.4) | 87 (66.4) | 205 (51.8) | 0.03 |
AVNRT, n (%) | 73 (13.9) | 17 (13) | 56 (14.1) | 0.74 |
Accessory pathway, n (%) | 56 (10.6) | 9 (6.9) | 47 (11.9) | 0.11 |
VEBs, n (%) | 117 (22.2) | 26 (19.8) | 91 (23) | 0.45 |
Hypertension, n (%) | 230 (43.6) | 60 (45.8) | 170 (42.9) | 0.57 |
ICD, n (%) | 36 (6.8) | 8 (6.1) | 28 (7.1) | 0.70 |
Pacemaker, n (%) | 129 (24.5) | 33 (25.2) | 96 (24.2) | 0.83 |
BAC, n (%) | 155 (29.4) | 34 (26.0) | 121 (30.6) | 0.32 |
Female sex, n (%) | 258 (49.0) | 65 (49.6) | 193 (48.7) | 0.86 |
Age, y | 51.6 (18.2) | 55.6 (15.7) | 50.3 (18.6) | 0.001 |
LA, mm | 40.2 (7.6) | 41.3 (6.9) | 39.9 (7.8) | 0.08 |
LV, mm | 50.0 (6.2) | 50.4 (5.6) | 49.8 (6.3) | 0.41 |
EF, % | 61.6 (8.5) | 61.3 (8.9) | 61.8 (8.4) | 0.57 |
IVS, mm | 10.6 (2.1) | 11.,0 (1.9) | 10.7 (2.1) | 0.17 |
Elevated NT‑proBNP, n (%) | 264 (50.1) | 76 (58.0) | 188 (47.5) | 0.04 |
NT‑proBNP, pg/ml | 132 (55−435) | 145 (76–456) | 129 (50−430) | 0.11 |
Parameter | Total (n = 527) | APB/AT/AF (+) (n = 292) | APB/AT/AF (–) (n = 235) | P value |
Data are presented as median (interquartile range) or mean (SD) unless indicated otherwise.
Abbreviations: IgG, immunoglobulin G; IgM, immunoglobin M; others, see Table 1 | ||||
Borrelia infection, n (%) | 131 (24.9) | 87 (29.8) | 44 (18.7) | 0.003 |
Borrelia IgG(+), n (%) | 93 (17.6) | 65 (22.3) | 28 (11.9) | 0.002 |
Borrelia IgM(+), n (%) | 64 (12.1) | 38 (13.0) | 26 (11.1) | 0.5 |
Borrelia IgG, RU/l | 6.8 (3.8–14.3) | 8.1 (4.1–17.0) | 5.8 (3.6–10.8) | 0.002 |
Borrelia IgM, RU/ml | 5.3 (3.2–10.4) | 5.0 (3.1–10.4) | 5.4 (3.4–10.2) | 0.54 |
Hypertension, n (%) | 230 (43.6) | 165 (56.5) | 65 (27.7) | <0.001 |
Female sex, n (%) | 258 (49.0) | 117 (40.1) | 141 (60) | <0.001 |
Age, y | 51.6 (18.2) | 58.1 (14.7) | 43.5 (18.7) | <0.001 |
LA, mm | 40.2 (7.6) | 43.1 (6.8) | 36.4 (6.8) | <0.001 |
LV, mm | 50.0 (6.2) | 50.4 (5.8) | 49.4 (6.5) | 0.08 |
EF, % | 61.6 (8.5) | 61.1 (8.1) | 62.4 (9.0) | 0.12 |
IVS, mm | 10.6 (2.1) | 11.2 (2.0) | 10.2 (2.0) | <0.001 |
Elevated NT‑proBNP, n (%) | 264 (50.1) | 192 (65.8) | 72 (30.6) | <0.001 |
NT‑proBNP, pg/ml | 132 (54.9–434.8) | 239.1 (95.6–662.6) | 70.8 (39.6–169.9) | <0.001 |
Analysis of the relationship between anti‑BB antibodies and risk factors for the occurrence of AF revealed an increased risk for AF and other SAs in female patients with anti‑BB antibodies (2.4‑fold higher risk; P = 0.003), patients aged over 65 years (4.3‑fold higher risk; P = 0.01), those with NT‑proBNP levels higher than 125 pg/ml (2.8‑fold higher risk; P = 0.004), and those with hypertension (3.3‑fold higher risk; P = 0.004). A correlation was found between the presence of anti‑BB antibodies and the level of NT‑proBNP (P for heterogeneity of OR = 0.047, Table 3). The level of anti‑BB IgG antibodies was also significant for the risk of AF occurrence (P = 0.003; Table 4).
Parameter | % | OR (95% CI) | P value | Parameter | % | OR (95% CI) | P value | P value for heterogeneity of OR |
Differences were significant at P <0.05.
Abbreviations: BB, Borrelia burgdorferi; OR, odds ratio; others, see Table 1 | ||||||||
Men (n = 269) | Women (n = 258) | |||||||
Any anti‑BB antibodies | 24.5 | 1.449 (0.792–2.652) | 0.229 | Any anti‑BB antibodies | 25.2 | 2.410 (1.354–4.291) | 0.003 | 0.23 |
IgG anti‑BB antibodies | 18.6 | 1.895 (0.937–3.833) | 0.075 | IgG anti‑BB antibodies | 16.7 | 2.344 (1.193–4.604) | 0.013 | 0.67 |
Age <65 years (n = 388) | Age ≥65 years (n = 139) | |||||||
Any anti‑BB antibodies | 23.5 | 1.469 (0.916–2.357) | 0.111 | Any anti‑BB antibodies | 28.8 | 4.299 (1.409–13.116) | 0.010 | 0.08 |
IgG anti‑BB antibodies | 15.5 | 1.716 (0.980–3.004) | 0.059 | IgG anti‑BB antibodies | 23.7 | 3.135 (1.018–9.652) | 0.046 | 0.35 |
NT‑proBNP >125 pg/ml (n = 264) | NT‑proBNP ≤125 pg/ml (n = 263) | |||||||
Any anti‑BB antibodies | 28.8 | 2.838 (1.398–5.762) | 0.004 | Any anti‑BB antibodies | 20.9 | 1.111 (0.605–2.041) | 0.734 | 0.047 |
IgG anti‑BB antibodies | 21.2 | 3.181 (1.367–7.402) | 0.007 | IgG anti‑BB antibodies | 14.1 | 1.288 (0.637–2.604) | 0.481 | 0.1 |
Hypertension | Without hypertension (n = 297) | |||||||
Any anti‑BB antibodies | 26.1 | 3.279 (1.459–7.367) | 0.004 | Any anti‑BB antibodies | 23.9 | 1.416 (0.829–2.419) | 0.203 | 0.09 |
IgG anti‑BB antibodies | 19.1 | 2.942 (1.179–7.343) | 0.021 | IgG anti‑BB antibodies | 16.5 | 1.816 (0.980–3.368) | 0.058 | 0.39 |
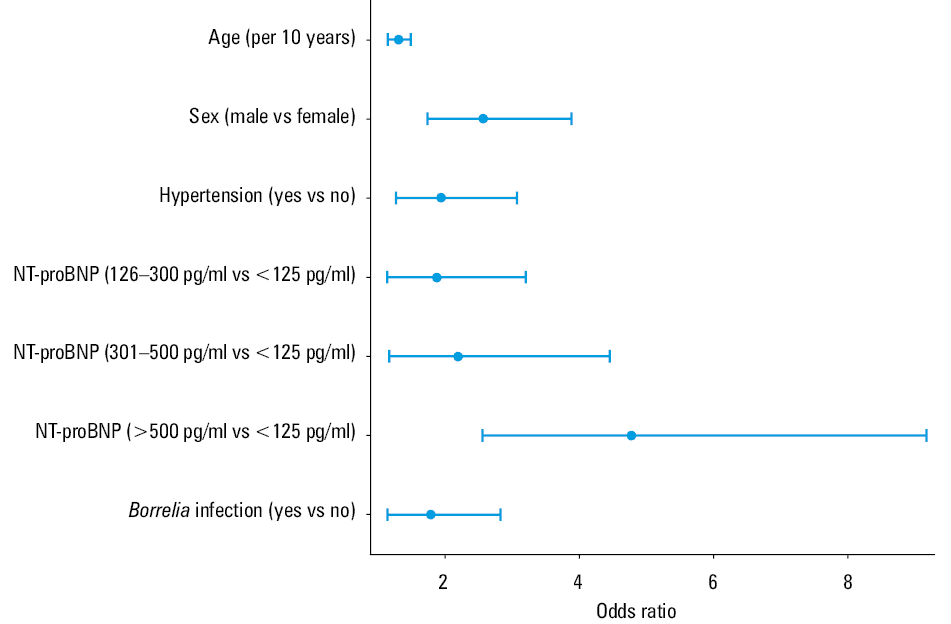
In the first model of multivariable analysis (including all elevated NT‑proBNP values), the indexed ORs (95% CIs) for hypertension, male sex, elevated levels of NT‑proBNP, and left atrial dimension were 2.223 (1.394– 3.548), 1.937 (1.195–3.139), 2.509 (1.559–4.037), and 1.102 (1.060–1.145), respectively (Table 5). Furthermore, the second statistical model (taking into account the ranges of the NT‑proBNP level) revealed the importance of anti‑BB antibody presence in the prediction of AF/AT/ABP (Figures 1 and 2).
Variablea | Univariable analysis | Multivariable analysis | ||
OR (95% CI) | P value | 95% CI | P value | |
a Dependent variable: APB/AT/AF
| ||||
Any anti‑BB antibodies | 1.842 (1.219–2.783) | 0.004 | 2.073 (1.219–3.524) | 0.007 |
Anti‑BB IgG antibodies | 2.116 (1.308–3.425) | 0.002 | – | – |
Anti‑BB IgM antibodies | 1.203 (0.707–2.046) | 0.496 | – | – |
Hypertension | 3.398 (2.352–4.908) | <0.001 | 2.223 (1.394–3.548) | <0.001 |
Male sex | 2.244 (1.580–3.186) | <0.001 | 1.937 (1.195–3.139) | 0.007 |
Age (per 1‑year increase) | 1.051 (1.039–1.063) | <0.001 | – | – |
LA, mm | 1.159 (1.121–1.199) | <0.001 | 1.102 (1.060–1.145) | <0.001 |
LV, mm | 1.028 (0.997–1.060) | 0.077 | – | – |
EF, % | 0.982 (0.960–1.005) | 0.122 | – | – |
IVS, mm | 1.330 (1.191–1.484) | <0.001 | – | – |
Elevated NT‑proBNP | 4.347 (3.009–6.280) | <0.001 | 2.509 (1.559–4.037) | <0.001 |
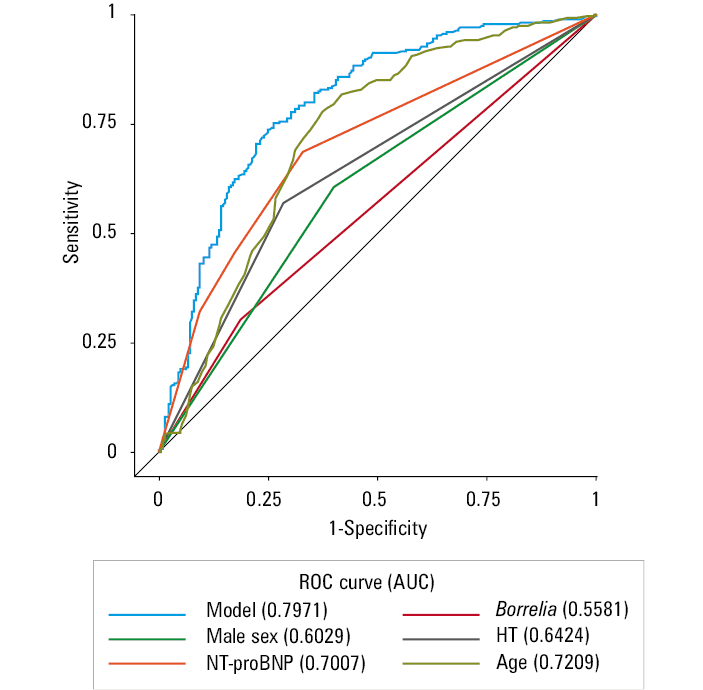
Abbreviations: AUC, area under the curve; HT, hypertension; others, see Table 1
In the multivariable analysis including interactions of risk factors (Table 6), the presence of anti‑BB antibodies increased the risk of AF/AT/ABP almost 3‑fold (OR, 2.906; 95% CI, 1.381–6.112) in patients with elevated NT‑proBNP values, while in the group of patients without elevated NT‑proBNP values, the presence of antibodies was not significant for the occurrence of these arrhythmias (OR, 0.995; 95% CI, 0.513–1.927).
Step | Independent variable | OR (95% CI) | P value |
a AUC = 0.791; 95% CI, 0.751–0.8300
| |||
Main effect | |||
1 | Age (per 1‑year increase) | 1.032 (1.018–1.047) | <0.001 |
2 | Male sex | 2.454 (1.645–3.662) | <0.001 |
3 | Hypertension | 1.750 (1.119–2.739) | 0.01 |
4 | Elevated NT‑proBNP values | 1.992 (1.228–3.232) | <0.001 |
5 | Presence of antibodies against Lyme disease | 0.995 (0.513–1.928) | 0.98 |
Interaction | |||
6 | Elevated NT‑proBNP values + presence of antibodies against Lyme disease | 2.921 (1.084–7.870) | 0.03 |
Discussion
Little is known about the acquisition of anti‑BB antibodies and their possible long‑term impact on the cardiovascular system, especially on the occurrence of cardiac arrhythmias in patients without the typical symptoms of LD or a history of its treatment. Moreover, there is no available report on the long‑term risk for SAs in patients with LD and elevated levels of NT‑proBNP. There are only a few case descriptions of AF which presented as LC,7,17,18 probably due to the effect of sudden and advanced conduction disorders. Only a single study assessed the prevalence of Borrelia infection in patients with AF.5
In the current study, we showed that the presence of antibodies against BB can increase the risk of AF and other SAs but only in the patients with elevated levels of NT‑proBNP. The incidence of AV blocks in patients with BB was investigated in previous studies.1,6,7 The present study is the first to report a greater risk for AF and other SAs in patients with elevated levels of NT‑proBNP who acquired antibodies against BB, even without a history of the typical symptoms of LD.
The presence of inflammation in the heart or systemic circulation can predict the onset of AF and its recurrence in the general population.19 Chronic inflammation associated with the systemic response to LD, particularly in patients who produced antibodies, may similarly increase the risk of AF. Importantly, the conduction disorders of the left atrium caused by spirochetes can facilitate the formation of microreentry waves responsible for AAs. We hypothesize that local inflammatory mediators may promote the activation of ectopic foci in the left atrium and pulmonary vein ostia. In the long period after the end of acute inflammation, fibrosis may occur in the left atrium, aggravating conduction abnormalities and increasing the risk of AF episodes. This is based on the number of antibodies against LD, implicating the body’s immune response to spirochete infection and, consequently, indicating a higher risk of developing AF.
The single reports of patients with damaged heart valves as well as heart failure can also draw attention to the other causes of AF in patients with BB antibodies. It is possible that a long‑lasting inflammatory reaction increases the risk of AF during a slow degenerative process in the valves or causes heart failure even with preserved ejection fraction (ie, diastolic heart failure); however, this is only a hypothesis requiring further study and testing. Meanwhile, it is worth noting that the increase in the NT‑proBNP level in patients with anti‑BB antibodies increased the risk of AAs, including AF. The level of anti‑BB IgG antibodies was also statistically significant for the risk of AF occurrence.
Interesting results were demonstrated in patients with known risk factors for AF, such as hypertension. In these patients, the presence of anti‑BB antibodies was shown to definitely increase the risk of AF as compared with patients without such antibodies. Moreover, the patients aged over 65 years with anti‑BB antibodies present had an increased risk for AF in our analysis.
The question arises whether the treatment of LD in patients with AF and anti‑BB antibodies would be an effective solution. In regions that are highly endemic for LD, a high level seroprevalence of specific antibodies is present in the general population, and its relevance to clinical disease has been questionable. Of note, LD is primarily a clinical diagnosis; therefore, serological analysis is only supportive in the diagnostic workup.21 Antibiotic therapy can be used even without waiting for antibody test results in patients with new‑onset AF with high‑degree AV block in regions endemic for LD, which may even prevent the need for an implantable pacemaker in these patients.7,17,18
Chronic post- or peri‑infective states causing discrete conduction disturbances and inflammatory conditions localized in AF‑prone parts of the heart can lead to AAs, such as AF. It is unknown whether the treatment of LD, such as antibiotic therapy, should be indicated to reduce the risk of recurrent AF, especially when the patient has no other symptoms of LD.
Study limitations
LD is primarily a clinical diagnosis; serological analysis is, thus, supportive in the diagnostic process.20 Confirmation of the presence of this disease is often difficult. However, morphologically intact spirochetes were readily detected in the affected heart sections by immunohistochemistry, even with negative culture results, in patients with confirmed LC who died from sudden cardiac failure.13,20 Moreover, false negative results may occur at the early stage of the disease, which does not exclude the diagnosis. In such cases, if the diagnosis is clinically suspected, ELISA may be repeated within 2 to 6 weeks.4 However, false positive results are common in LD‑endemic areas, where seropositivity rates may be even 4% to 5% among the general population4; thus, the relevance to clinical disease is questionable.17 Approximately 40% of patients who develop LC will have an erythema migrans rash, as compared with 70% of patients with other LD manifestations.18,21 This means that approximately 60% of patients have no noticeable symptoms. Although it is well known that LC is regarded as a “disorder with many faces,” it still represents a diagnostic challenge for clinicians.4 However, the etiology of BB infection should be definitely considered in patients with treatment‑resistant AF and other AAs, especially in those with elevated NT‑proBNP levels who are living in BB‑endemic regions.
- Piccirillo BJ, Pride YB. Reading between the Lyme: is Borrelia burgdorferi a cause of dilated cardiomyopathy? The debate continues. Eur J Heart Fail. 2012; 14: 567‑568. | Crossref
- Steere AC. Lyme disease. N Engl J Med. 2001; 345: 115‑125. | Crossref
- Konopka M, Kuch M, Braksator W, et al. Unclassified cardiomyopathy or Lyme carditis? A three‑year follow‑up. Kardiol Pol. 2013; 71: 283‑285. | Crossref
- Kostić T, Momčilović S, Perišić ZD, et al. Manifestations of Lyme carditis. Int J Cardiol. 2017; 232: 24‑32. | Crossref
- Szymanska A, Platek AE, Dluzniewski M, Szymanski FM. History of Lyme disease as a predictor of atrial fibrillation. Am J Cardiol. 2020; 125: 1651‑1654. | Crossref
ARTICLE INFORMATION