A 39‑year‑old man was admitted to the hospital for altered mental status. One week prior to the admission, the patient had a moped accident. His past medical history was remarkable for polysubstance abuse, alcoholism, chronic pancreatitis with multiple exacerbations, peripancreatic pseudocysts, inferior mesenteric vein thrombosis, and chronic splenic vein thrombosis.
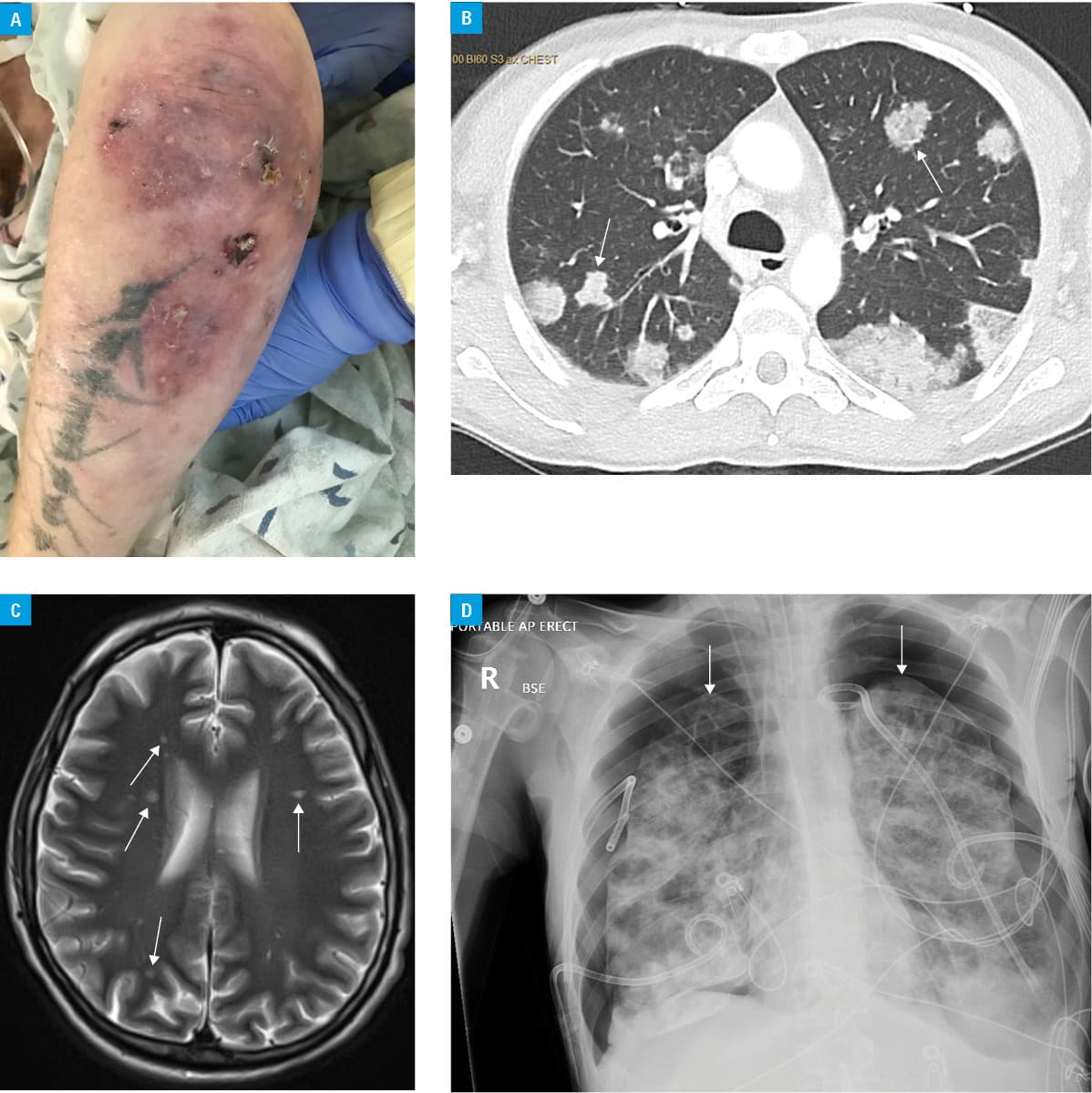
At initial presentation, the body temperature was 35.1 °C, blood pressure 76/51 mm Hg, heart rate 114 bpm, and oxygen saturation as measured by pulse oximetry 92% on room air. The physical examination demonstrated bilateral crackles on auscultation and hepatosplenomegaly. Notably, the dorsal surface of the left forearm was indurated and erythematous with purulent discharge (Figure 1A). Biochemical tests revealed a normal white blood cell count, thrombocytopenia, and elevated lactic acid and serum creatinine levels. The urinalysis was consistent with a urinary tract infection. Computed tomography (CT) demonstrated multiple consolidations throughout the lung parenchyma bilaterally (Figure 1B). Magnetic resonance imaging (MRI) of the brain showed numerous showering emboli (Figure 1C).
The patient was intubated for acute hypoxic and hypercapnic respiratory failure and samples were collected for bacterial cultures. Broad spectrum antibiotics, intravenous fluids, and norepinephrine drip were initiated.
The differential diagnosis of CT findings included, but was not limited to, cavitary pulmonary metastases, necrobiotic lung nodules (seen in rheumatoid arthritis and inflammatory bowel disease), granulomatosis with polyangiitis, and pulmonary embolism.1 The MRI findings included embolism originating from left cardiac chambers. Additionally, paradoxical embolism across a patent foramen ovale or ventricular septal defects could be considered.
Blood, left upper extremity wound, tracheal aspirate, and urine cultures grew methicillin‑resistant Staphylococcus aureus (MRSA). Left upper extremity vascular duplex ultrasound showed extensive acute deep venous thrombosis. Transesophageal echocardiogram did not show evidence of intracardiac thrombi, mass, vegetations, or intracardiac shunt. Serological diagnostic testing results were negative for rheumatoid factor, antiproteinase 3 and antimyeloperoxidase antibodies, antiglomerular basement membrane, anti‑Smith, anti‑Smith/RNP, and anti‑SSA/SSB antibodies. Complement C3 and C4 levels were within the normal range. Electroencephalography showed burst suppression but no seizure activity.
The hospital course was complicated by bilateral tension pneumothoraces (Figure 1D) and left‑sided chorioretinal abscess with left eye endophthalmitis. A chest tube was inserted emergently, and intravitreal injection of vancomycin was performed by an ophthalmologist.
Ventilation support became ineffective due to a large air leak and the patient’s family decided to pursue comfort measures. The patient was extubated and passed away a few hours later.
To the best of our knowledge, this is the first reported case of simultaneous multiple septic emboli in the lungs, the brain, and the retina secondary to upper extremity MRSA thrombophlebitis.
Cerebral septic emboli usually originate from left‑sided endocarditis with or without mitral valve vegetations.2,3 There are few case reports of retinal septic emboli secondary to endocarditis or following dental surgery.4,5
Interestingly, left‑sided endocarditis or valvular vegetations, which could explain septic emboli in the brain and the retina, were not found. An assumption was made that microorganism‑containing thrombi caused a mechanical obstruction and inflammatory reaction that resulted in right‑to‑left shunt and pulmonary capillary vessel breakdown. In consequence, translocation of the infected thrombi to the left heart resulted in emboli in the brain and the retina. The proposed pathomechanism could explain the small size of cerebral microthrombi.
This is an interesting and unusual case of an upper extremity thrombophlebitis with septic emboli in the lungs, the brain, and the retina without coexisting endocarditis or intracardiac septal defects.
- Aberle DR, Gamsu G, Lynch D. Thoracic manifestations of Wegener granulomatosis: diagnosis and course. Radiology. 1990; 174: 703‑709. | Crossref
- Pruitt AA, Rubin RH, Karchmer AW, et al. Neurologic complications of bacterial endocarditis. Medicine (Baltimore). 1978; 57: 329‑343. | Crossref
- Özbek C, Yetkin U, Bademci M, et al. Ring annuloplasty and successful mitral valve repair in a staphylococcal endocarditis case with bilobular saccular mycotic aneurysm at cerebral artery and frontal region infarction. Secondary to septic emboli. Arch Med Sci. 2008; 4, 1: 94‑99.
- Wathek C, Rannen R. Ocular manifestations of endocarditis. In: Firstenberg MS, ed. Contemporary Challenges in Endocarditis. London: IntechOpen; 2016. | Crossref
- Kilmartin DJ, Barry P. Recurrent septic retinal emboli following dental surgery. Br J Ophthalmol. 1996; 80: 1111‑1112. | Crossref
ARTICLE INFORMATION