Adjuvant combined therapy with trastuzumab in patients with HER2‑positive breast cancer and cardiac alterations: implications for optimal cardio‑oncology care
Key words: adjuvant setting, cardiotoxicity, HER2-positive breast cancer, trastuzumab



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Adjuvant combined therapy with trastuzumab in patients with HER2‑positive breast cancer and cardiac alterations: implications for optimal cardio‑oncology care
Introduction: Recently, the prognosis of patients with HER2‑positive breast cancer (BC) has improved significantly owing to the use of combined treatment modalities. However, systemic treatment is associated with increased risk of cardiotoxicity.
Objectives: We aimed to assess subclinical cardiac alterations during the final stage of adjuvant combined therapy, that is, trastuzumab therapy (TT), as potential predictors of late cardiac complications in patients with HER2‑positive BC.
Patients and methods: We enrolled 251 patients with HER2‑positive BC treated with a radical local therapy, adjuvant chemotherapy (anthracyclines or anthracyclines + taxanes), and immunotherapy (trastuzumab). Patients underwent 6 echocardiographic examinations: at baseline, during TT, and after TT, with assessment of left ventricular ejection fraction (LVEF), degree of valvular regurgitation, and cardiac chamber diameters.
Results: Valvular fibrosis (28.4% of patients) was associated with older age, hypertension at baseline, and a higher degree of regurgitation during TT. Reduced LVEF, greater regurgitation, and larger cardiac chamber diameters were noted during TT. The patients who received higher anthracycline doses showed a greater degree of aortic insufficiency and a larger right ventricular diameter. Reduced LVEF during TT was associated with radiotherapy or chemotherapy and the degree of valvular regurgitation. Significantly larger diameters were observed in older patients and in those with comorbidities at baseline, high body mass index, and regurgitation.
Conclusions: Asymptomatic subclinical cardiac alterations during TT may predict late cardiac complications; however, longer follow‑up is necessary to confirm this hypothesis. Patients with HER2‑positive BC should be closely monitored for possible cardiac alterations during and after therapy to ensure optimal care and guide therapeutic decision‑making.
What's new?
In this study, we used echocardiography to identify a number of subclinical cardiac alterations that might serve as predictors of cardiotoxicity and premature cardiac death in women with HER2‑positive breast cancer during and a few months after a radical combined treatment (chemotherapy, radiotherapy, immunotherapy, and hormone replacement therapy). Interestingly, we observed that some patients who did not receive radiotherapy developed mitral and / or aortic valve fibrosis with secondary valvular insufficiency. However, patients treated with radiotherapy developed valvular fibrosis earlier than expected. In some patients, we also noted functional mitral regurgitation due to slight enlargement and geometrical changes of the left ventricle and atrium. Finally, we observed development or progression of tricuspid regurgitation. Close monitoring for cardiac alterations during and after radical combined treatment with trastuzumab is strongly recommended to guide therapeutic decisions and ensure optimal care in patients with HER2‑positive breast cancer.
Introduction
Over the past 10 years, there have been significant advances in the radical treatment of HER2‑positive breast cancer (BC).1 The use of targeted anti‑HER2 therapy in combination with chemotherapy (anthracyclines, taxanes) has vastly improved the prognosis of patients. At the same time, progress in local treatment modalities (surgery, radiotherapy) allowed clinicians to minimize damage to healthy tissues without compromising the efficacy of the radical treatment.2-4 However, systemic treatment is a known risk factor for early and late cardiac complications, which, in turn, increase the risk of premature cardiac death.5
The aim of the study was to use standard echocardiographic examinations to assess subclinical changes in the heart as potential predictors of symptomatic cardiotoxicity and premature cardiac death.
Patients and methods
This was a retrospective cohort study including 251 women with BC treated at the Institute of Oncology in Kraków, Poland, with adjuvant trastuzumab between 2008 and 2019. The inclusion criteria were the diagnosis of HER2‑positive BC and absence of contraindications to chemotherapy and radiotherapy. Patients with a left ventricular ejection fraction (LVEF) of less than 50% and significant cardiac contraindications to immunotherapy (eg, acute coronary syndrome, ventricular tachycardia) were excluded.
All patients showed HER2 receptor overexpression, underwent radical surgery (mastectomy or breast‑conserving surgery), adjuvant chemotherapy and immunotherapy (trastuzumab) as well as radiotherapy (202 patients, depending on individual indications), and received hormone therapy (in the case of positive hormone receptors). HER2 expression was assessed by immunohistochemistry (HercepTest; F. Hoffmann‑La Roche, Basel, Switzerald). If the test results were equivocal, amplification of the ERBB2 gene by fluorescent in situ hybridization was additionally assessed.6 According to the protocol, trastuzumab was administered for 12 months. Treatment was discontinued within 1 year since the development of significant cardiac complications. Cardiotoxicity was defined as a reduction in LVEF below 50% or more than 10 percentile points from baseline. In these cases, treatment was always discontinued. For the purpose of this study, the term “significant cardiac complications” was defined as cardiac complications that were considered a significant contraindication to the continuation of trastuzumab therapy (TT), at the physician’s discretion. The women with cardiac complications received treatment with angiotensin‑converting enzyme inhibitors (ACEIs), angiotensin II‑receptor antagonists, β-adrenergic blocking agents, aldosterone inhibitors, and diuretics, as appropriate. Doses were gradually uptitrated according to blood pressure, and electrolyte and creatinine levels. During the therapy, effective contraception (accepted in BC) was recommended in all women.
Our center provides complex cardio‑oncology care. Our team includes a highly qualified cardiologist (E.K.) with access to appropriate noninvasive diagnostic equipment as well as experience in managing cardiac complications and consulting complex cases. Other cardiology consultants are also available at our center. In the future, we are going to cooperate with the Department of Cardiology that employs the main consultant for cancer patients requiring hospitalization.
Radiotherapy was applied after completing chemotherapy. For radiotherapy after breast‑conserving surgery, tangential fields were used for whole‑breast irradiation, while in patients with nodal involvement, the monoisocentric technique was used for breast and regional nodal irradiation. Additionally, all patients received an amended boost to the tumor bed. For radiotherapy administered after mastectomy, the monocentric technique with mixed photon‑electron beam was used to irradiate the target volume, including the chest wall with the postoperative scar as well as internal mammary, axillary, supraclavicular, and infraclavicular lymph nodes. The radiotherapy was performed with a linear accelerator with the application of megavoltage photon and electron beams. In all patients, the radiotherapy was planned on the basis of computed tomography scans and a 3‑dimensional radiotherapy technique with delineation of the target and organ‑at‑risk volumes. In the patients with a pacemaker, the device and the electrode were delineated on radiographs, and the dose for these areas was estimated in a radiotherapy plan. Before the radiotherapy, the patients underwent a cardiac consultation and their cardiac function was monitored during the radiotherapy implementation.
Clinical examination
Before the initiation of TT, all patients were assessed for the presence of cardiovascular risk factors (increased body mass index [BMI], hypertension [HA], ischemic heart disease [IHD], diabetes mellitus [DM]) according to our standard protocol. At baseline, all participants underwent subjective and objective clinical examination. HA was defined as a blood pressure of 140/90 mm Hg or higher (on at least 2 separate measurements) or the use of antihypertensive drugs for elevated blood pressure. DM was defined according to the current guidelines.7 In all patients, echocardiography was performed.
Echocardiography
Complete echocardiographic examination was performed using a GE VIVID S‑6 ECHO unit (GE Medical System, Boston, Massachusetts, United States), equipped with a multifrequency harmonic transducer (2.5–4 MHz). Most patients were examined by the same experienced operator (E.K.). Echocardiography was performed at baseline (before TT), every 3 months during immunotherapy (TT), and a few (3–6) months after TT. The mean values of 3 consecutive measurements were recorded. Left ventricular (LV) systolic function was assessed on the basis of LVEF measurement using the Simpson method. Cardiac chamber quantification was performed according to the recommendations of the American Society of Echocardiography and the European Association of Cardiovascular Imaging.8 Left atrial (LA) diameter was expressed as body surface area–indexed LA volume. Right atrial (RA) diameter was defined as RA volume calculated using a single‑plane area‑length or disk summation method in an apical 4‑chamber view. LV sizes were expressed as diastolic and systolic dimensions as well as LV volumes normalized by the body surface area. Right ventricular (RV) diameters were obtained in a standard position, and RV systolic function was assessed by tricuspid annular plane systolic excursion as well as tissue Doppler imaging–derived tricuspid lateral annular systolic velocity. Valvular regurgitation was evaluated according to the recommendations of the European Association of Cardiovascular Imaging, in which native valvular regurgitation is classified as mild, mild / moderate, moderate, moderate to severe, or severe.9 In our study, all degrees were considered in the analysis in order to assess a patient’s tendency to have either a higher or a lower degree of valvular regurgitation. At baseline, some patients presented with the first or second degree functional mitral insufficiency, tricuspid insufficiency, and aortic insufficiency. Changes in the degree of valvular insufficiency during treatment vs baseline were also assessed. Valvular fibrosis was assessed visually by an experienced cardiologist. The results of all echocardiographic examinations were recorded, and the results of each subsequent examination were compared with baseline. Fibrosis was identified by assessing differences in the echogenicity of the valve leaflets and changes in their mobility. Doubtful cases were examined and discussed by 2 experienced investigators until a consensus was reached.
The primary study end point was defined as subclinical changes in the heart (assessed by echocardiography) during the combined radical treatment of HER2‑positive BC. The secondary end point was defined as the occurrence of significant valvular insufficiency and cardiac enlargement during treatment.
Statistical analysis
The following tests were applied for statistical analysis: 1) the Pearson χ2 or Fisher test to assess the independence of categorical variables presented using a contingency Table; and 2) the repeated measures analysis of variance (repeated measures ANOVA) for differences in the mean degree of LVEF or cardiac chamber diameter measured at 6 time points (at baseline, every 3 months during TT, and after the therapy) according to variables including the presence of valvular insufficiency, cardiac complications (myocardial dysfunction, cardiac arrhythmias, LVEF reduction <50% or >10 percentile points), DM, HA, IHD, chemotherapy regimen, as well as the use of radiotherapy and hormone replacement therapy; 3) the Friedman test for valvular regurgitation measured at 6 time points and the Mann–Whitney test to assess differences between groups at the same time point (according to variables including age, the presence of valvular insufficiency, HA, chemotherapy regimen). A P value lower than 0.05 was considered significant. The STATISTICA v.10.0 software (StatSoft, Inc., Tulsa, Oklahoma, United States) was used for all calculations.
Ethical issues
The study was approved by the Independent Ethics Committee at the Regional Medical Chamber in Kraków (decision as of December 4, 2013, no. 2013/09/B/NZ5/00764; to J.N.). This was a retrospective study with no direct patient contact, no modification of diagnostic or treatment procedures, and no disclosure of personal patient data. Therefore, the patient consent was not required for this study.
Results
The patients with valvular fibrosis diagnosed at baseline (before TT) or during TT were significantly older than those without fibrosis (P <0.001) (Table 1). Moreover, the absence of valvular fibrosis was the most common in the patients without HA (P = 0.01) (Table 1). Additionally, during TT, we noted a higher degree of mitral regurgitation in women with valvular fibrosis (Table 2). Detailed associations between the clinical parameters and the valvular fibrosis are presented in Table 1.
Parametera | Valvular fibrosis | |||
Absent (n = 180) | Present (n = 71) | P valuee | ||
Data are presented as number (percentage) of patients unless otherwise indicated.
a A mismatch in the number of cases results from the lack of data for some parameters.
b The following cardiac complications were noted: LVEF reduction by more than 10 percentile points vs baseline or LVEF reduction below 50%; heart failure (NYHA functional class III/IV); grade III/IV (mild / severe) valvular insufficiency; arrhythmia (atrial fibrillation, ventricular arrhythmias); LVEF reduction by more than 10 percentile points vs baseline plus heart failure (NYHA functional class III/IV); and LVEF reduction by more than 10 percentile points vs baseline plus arrhythmia.
c All patients with hypertension received ACEIs, β-blockers, and thiazides.
d All patients with ischemic heart disease received ACEIs, β-blockers, antiplatelet drugs.
e P value from analysis of variance or from the Fisher (2 × 2 contingency Table) or Person χ2 test
Abbreviations: ACEI, angiotensin‑converting enzyme inhibitor; BMI, body mass index; LVEF, left ventricular ejection fraction; NYHA, New York Heart Association | ||||
Age, y, mean (SD) | 52.5 (10.1) | 59.8 (7.8) | <0.001 | |
Baseline BMI, kg/m2, mean (SD) | 27.3 (5.0) | 27.8 (5.5) | 0.51 | |
Cardiac complicationsb | Not present | 155 (72.1) | 60 (27.9) | 0.54 |
Present | 25 (71.4) | 10 (28.6) | ||
Diabetes mellitus | Not present | 173 (72.7) | 65 (27.3) | 0.28 |
Present | 8 (61.5) | 5 (38.5) | ||
Hypertensionc | Not present | 133 (76.9) | 40 (23.1) | 0.01 |
Present | 47 (61.0) | 30 (39.0) | ||
Ischemic heart diseased | Not present | 167 (72.9) | 62 (27.1) | 0.24 |
Present | 14 (63.6) | 8 (36.4) | ||
Radiotherapy | No | 34 (69.4) | 15 (30.6) | 0.38 |
Yes | 147 (72.8) | 55 (27.2) | ||
Chemotherapy | Anthracyclines ≤300 mg/m2 | 65 (69.1) | 29 (30.9) | 0.39 |
Anthracyclines >300 mg/m2 | 33 (67.3) | 16 (32.7) | ||
Anthracyclines and taxanes | 78 (76.5) | 24 (23.5) | ||
Hormone replacement therapy | No | 76 (66.1) | 39 (33.9) | 0.04 |
Yes | 105 (77.2) | 31 (22.8) | ||
Parameter | Patients, n | Degree of regurgitation, median (IQR)a | P valueb | P valuec | ||||||
Baseline before TT | During treatment | After TT | ||||||||
3 months | 6 months | 9 months | 12 months | |||||||
a 0 for absence of regurgitation, 1 for mild (degree I), 1.5 for mild / moderate (degree I/II), 2 for moderate (degree II); 2.5 for moderate / severe (degree II/III); 3 for severe (degree III)
b Difference between the 2 groups (the Mann–Whitney test for differences between groups at the same time point)
c Difference between subsequent measurements (the Friedman test)
P value: d <0.001; e 0.001; f 0.004; g 0.003; h 0.05; i 0.02; j 0.04; k 0.002; l 0.01
Abbreviations: IQR, interquartile range; TT, trastuzumab therapy | ||||||||||
Whole group | 243 | 0.0 (0.0–0.1) | 0.0 (0.0–1.0) | 0.0 (0.0–0.1) | 1.0 (0.0–0.1) | 1.0 (0.0–0.1) | 1.0 (0.0–0.1) | – | <0.001 | |
Regurgitation | Present only during and / or after TT | 107 | 0.0d (0.0–0.0) | 0.0d (0.0–1.0) | 1.0d (0.0–1.0) | 1.0d (0.0–1.5) | 1.0e (0.0–1.0) | 1.0d (0.0–1.0) | d<0.001; e 0.001 | <0.001 |
Present before and during and / or after TT | 63 | 1.0 (1.0–1.5) | 1.0 (1.0–1.75) | 1.0 (1.0–2.0) | 1.0 (1.0–2.0) | 1.0 (1.0–2.0) | 1.0 (1.0–2.0) | 0.91 | ||
Hypertension | No | 167 | 0.0 (0.0–0.0) | 0.0 (0.0–1.0) | 0.0f (0.0–1.0) | 0.0 (0.0–1.0) | 1.0 (0.0–1.0) | 0.0g (0.0–1.0) | f 0.004;
g 0.03 | <0.001 |
Yes | 76 | 0.0 (0.0–1.0) | 0.0 (0.0–1.0) | 1.0 (0.0–1.5) | 1.0 (0.0–1.0) | 1.0 (0.0–1.0) | 1.0 (0.0–1.0) | <0.001 | ||
Age | ≤54 years | 114 | 0.0 (0.0–0.0) | 0.0 (0.0–1.0) | 0.0d (0.0–1.0) | 0.0d (0.0–1.0) | 0.0d (0.0–1.0) | 0.0a (0.0–1.0) | d <0.001 | <0.001 |
>54 years | 129 | 0.0 (0.0–0.0) | 0.0 (0.0–1.0) | 1.0 (0.0–1.5) | 1.0 (0.0–1.5) | 1.0 (0.0–1.5) | 1.0 (0.0–1.5) | <0.001 | ||
Valvular fibrosis | Absent | 170 | 0.0 (0.0–0.0) | 0.0 (0.0–1.0) | 0.0e (0.0–1.0) | 1.0h (0.0–1.0) | 1.0 (0.0–1.0) | 1.0 (0.0–1.0) | e 0.001;
h 0.05 | <0.001 |
Present | 69 | 0.0 (0.0–1.0) | 0.0 (0.0–1.0) | 1.0 (0.0–2.0) | 1.0 (0.0–2.0) | 1.0 (0.0–1.5) | 1.0 (0.0–1.0) | <0.001 | ||
Tricuspid regurgitation (no regurgitation in 159 cases), median (IQR) | ||||||||||
Whole group | 244 | 0.0 (0.0–0.0) | 0.0 (0.0–0.0) | 0.0 (0.0–0.0) | 0.0 (0.0–0.0) | 0.0 (0.0–0.0) | 0.0 (0.0–1.0) | – | <0.001 | |
Regurgitation | Present only during and / or after TT | 70 | 0.0ad (0.0–0.0) | 0.0d (0.0–0.0) | 0.0i (0.0–1.0) | 1.0j (0.0–1.0) | 1.0 (0.0–1.0) | 1.0 (0.0–1.0) | d<0.001; i0.02;
j0.04 | <0.001 |
Present before and during and / or after TT | 15 | 1.0 (1.0–2.0) | 1.0 (1.0–2.0) | 1.0 (0.5–2.0) | 1.0 (1.0–2.0) | 1.0 (1.0–2.0) | 1.0 (0.5–2.0) | 0.94 | ||
Aortic regurgitation (no regurgitation in 211 cases), median (IQR) | ||||||||||
Whole group | 246 | 0.0 (0.0–0.0) | 0.0 (0.0–0.0) | 0.0 (0.0–0.0) | 0.0 (0.0–0.0) | 0.0 (0.0–0.0) | 0.0 (0.0–0.0) | – | <0.001 | |
Regurgitation | Present only during and / or after TT | 24 | 0.0d (0.0–0.0) | 0.0k (0.0–1.0) | 1.0l (0.0–1.0) | 1.0l (0.0–1.0) | 1.0 (1.0–1.0) | 1.0l (0.0–1.0) | d<0.001; k0.002;
l0.01 | <0.001 |
Present before and during and / or after TT | 11 | 1.0 (1.0–1.5) | 1.0 (1.0–1.5) | 1.0 (1.0–1.5) | 1.0 (1.0–1.5) | 1.0 (1.0–1.5) | 1.75 (1.0–2.0) | 0.22 | ||
Anthracycline | ≤300 mg/m2 | 187 | 0.0 (0.0–0.0) | 0.0 (0.0–0.0) | 0.0 (0.0–0.0) | 0.0 (0.0–0.0) | 0.0 (0.0–0.0) | 0.0 (0.0–0.0) | – | 0.004 |
>300 mg/m2 | 55 | 0.0 (0.0–0.0) | 0.0 (0.0–0.0) | 0.0 (0.0–0.0) | 0.0 (0.0–0.0) | 0.0 (0.0–0.0) | 0.0 (0.0–0.0) | <0.001 | ||
Valvular fibrosis | Absent | 172 | 0.0 (0.0–0.0) | 0.0 (0.0–0.0) | 0.0 (0.0–0.0) | 0.0 (0.0–0.0) | 0.0 (0.0–0.0) | 0.0 (0.0–0.0) | – | 0.001 |
Present | 69 | 0.0 (0.0–0.0) | 0.0 (0.0–0.0) | 0.0 (0.0–0.0) | 0.0 (0.0–0.0) | 0.0 (0.0–0.0) | 0.0 (0.0–0.0) | 0.004 | ||
The degree of mitral, tricuspid, and aortic regurgitation at baseline, during, and after TT depending on the type and presence of regurgitation is presented in Table 2. During TT, the degree of mitral, tricuspid, and aortal regurgitation increased (P <0.001, Table 2). Higher degrees of mitral, tricuspid, and aortic regurgitation were found in the patients with valvular insufficiency diagnosed at baseline, during, and after TT as compared with those with valvular regurgitation observed only during or after TT (Table 2).
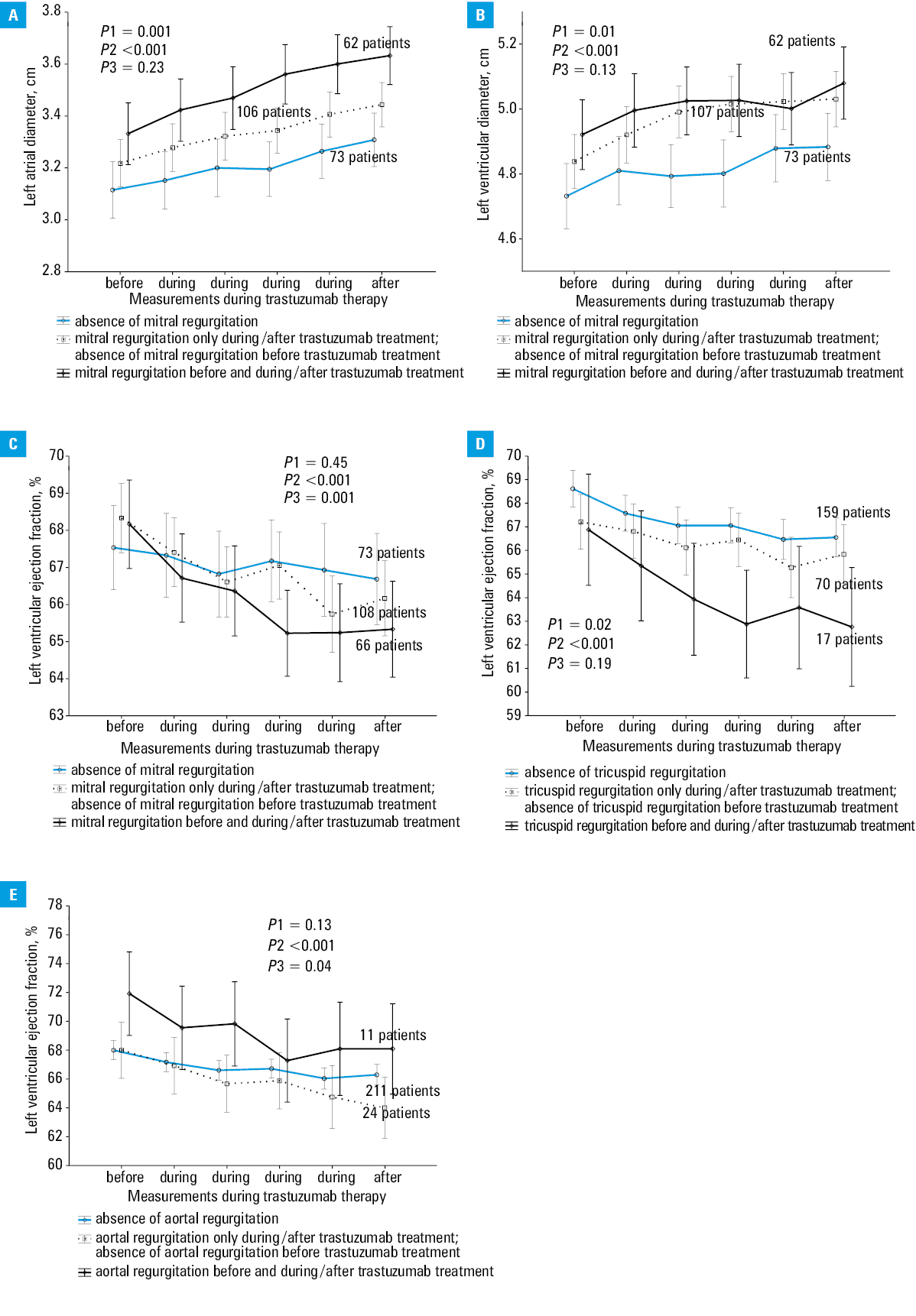
Changes in the mean LA, LV, and RV diameters during TT according to clinical parameters are presented in Table 3. During TT, an increase in LA, LV, and RV diameters was observed (all P <0.001, Table 3). At each time point, LA and LV diameters were smaller in the patients without mitral insufficiency than in those with insufficiency both at baseline and during or after TT (Figure 1A and 1B).
Parameter | Cardiac chamber diameter, cm, mean (SD) | P valuea | P valueb | P valuec | |||||||
Patients, n | Baseline before TT | During TT | After TT | ||||||||
3 months | 6 months | 9 months | 12 months | ||||||||
An increase in heart chamber diameters during TT was calculated as a sum of correlation coefficients (R of a series of 6 measurements done for each patient before, during [4 measurements], and after TT) and 3 heart chambers (R of the left ventricle + R of the left atrium + R of the right atrium – calculated for each patient). The cutoff point for this variable was set at 1.9 (the upper quartile).
P values were calculated using repeated measure analysis of variance.
a Difference between the 2 groups
b Difference between subsequent measurements
c Difference in the slope of the plots representing the 2 groups
| |||||||||||
Left atrial diameter, cm, mean (SD) | |||||||||||
Whole group | 243 | 3.2 (0.5) | 3.3 (0.5) | 3.3 (0.5) | 3.4 (0.5) | 3.4 (0.5) | 3.4 (0.5) | – | <0.001 | – | |
IHD | No | 221 | 3.2 (0.5) | 3.2 (0.5) | 3.3 (0.5) | 3.3 (0.5) | 3.4 (0.5) | 3.4 (0.5) | 0.003 | <0.001 | 0.27 |
Yes | 21 | 3.5 (0.3) | 3.6 (0.4) | 3.6 (0.4) | 3.6 (0.3) | 3.6 (0.3) | 3.7 (0.3) | ||||
Hypertension | No | 167 | 3.1 (0.5) | 3.2 (0.4) | 3.2 (0.5) | 3.2 (0.4) | 3.3 (0.4) | 3.3 (0.4) | <0.001 | <0.001 | <0.001 |
Yes | 74 | 3.4 (0.5) | 3.5 (0.5) | 3.5 (0.5) | 3.6 (0.5) | 3.7 (0.5) | 3.7 (0.5) | ||||
Diabetes mellitus | No | 230 | 3.2 (0.5) | 3.3 (0.5) | 3.3 (0.5) | 3.3 (0.5) | 3.4 (0.5) | 3.4 (0.5) | 0.04 | <0.001 | 0.27 |
Yes | 12 | 3.5 (0.6) | 3.4 (0.5) | 3.6 (0.4) | 3.7 (0.4) | 3.7 (0.4) | 3.6 (0.5) | ||||
Age | ≤54 years | 115 | 3.1 (0.4) | 3.2 (0.5) | 3.2 (0.5) | 3.2 (0.4) | 3.3 (0.4) | 3.3 (0.4) | <0.001 | <0.001 | 0.69 |
>54 years | 126 | 3.3 (0.5) | 3.4 (0.5) | 3.4 (0.5) | 3.5 (0.5) | 3.5 (0.5) | 3.6 (0.5) | ||||
BMI | ≤25 kg/m2 | 87 | 3.0 (0.5) | 3.1 (0.5) | 3.1 (0.5) | 3.1 (0.4) | 3.2 (0.4) | 3.2 (0.4) | <0.001 | <0.001 | 0.37 |
>25 kg/m2 | 155 | 3.3 (0.5) | 3.4 (0.5) | 3.4 (0.5) | 3.5 (0.5) | 3.5 (0.5) | 3.6 (0.4) | ||||
Left ventricular diameter, cm, mean (SD) | |||||||||||
Whole group | 245 | 4.8 (0.4) | 4.9 (0.5) | 4.9 (0.4) | 5.0 (0.5) | 5.0 (0.5) | 5.0 (0.5) | – | <0.001 | – | |
Hypertension | No | 176 | 4.8 (0.4) | 4.9 (0.5) | 4.9 (0.4) | 4.9 (0.4) | 4.9 (0.4) | 4.9 (0.4) | 0.008 | <0.001 | 0.37 |
Yes | 78 | 4.9 (0.4) | 5.0 (0.4) | 5.0 (0.4) | 5.1 (0.5) | 5.1 (0.5) | 5.1 (0.5) | ||||
BMI | ≤25 kg/m2 | 92 | 4.7 (0.4) | 4.8 (0.5) | 4.8 (0.4) | 4.8 (0.4) | 4.8 (0.4) | 4.8 (0.4) | <0.001 | <0.001 | 0.90 |
>25 kg/m2 | 163 | 4.9 (0.4) | 5.0 (0.4) | 5.0 (0.4) | 5.0 (0.5) | 5.0 (0.5) | 5.1 (0.5) | ||||
Cancer progression | No | 210 | 4.8 (0.4) | 4.9 (0.5) | 5.0 (0.4) | 5.0 (0.4) | 5.0 (0.4) | 5.0 (0.5) | 0.03 | <0.001 | 0.87 |
Yes | 35 | 4.7 (0.5) | 4.8 (0.5) | 4.8 (0.4) | 4.8 (0.5) | 4.9 (0.5) | 4.9 (0.4) | ||||
Right ventricular diameter, cm, mean (SD) | |||||||||||
Whole group | 240 | 2.6 (0.5) | 2.6 (0.6) | 2.7 (0.5) | 2.7 (0.5) | 2.7 (0.6) | 2.7 (0.5) | – | <0.001 | – | |
IHD | No | 228 | 2.5 (0.6) | 2.6 (0.6) | 2.6 (0.5) | 2.7 (0.5) | 2.7 (0.6) | 2.7 (0.5) | 0.02 | <0.001 | 0.83 |
Yes | 22 | 2.8 (0.5) | 2.8 (0.5) | 2.9 (0.5) | 2.9 (0.5) | 3.0 (0.6) | 2.9 (0.5) | ||||
Anthracycline | ≤300 mg/m2 | 180 | 2.5 (0.6) | 2.5 (0.6) | 2.6 (0.5) | 2.6 (0.5) | 2.6 (0.6) | 2.7 (0.5) | <0.001 | <0.001 | 0.82 |
>300 mg/m2 | 55 | 2.8 (0.5) | 2.8 (0.5) | 2.9 (0.5) | 3.0 (0.5) | 3.0 (0.5) | 3.0 (0.5) | ||||
BMI | ≤25 kg/m2 | 92 | 2.5 (0.6) | 2.5 (0.5) | 2.6 (0.5) | 2.6 (0.5) | 2.6 (0.5) | 2.6 (0.6) | 0.02 | <0.001 | 0.88 |
>25 kg/m2 | 158 | 2.6 (0.6) | 2.6 (0.6) | 2.7 (0.5) | 2.7 (0.5) | 2.8 (0.6) | 2.8 (0.5) | ||||
Abbreviations: see Table 2
Changes in the mean LVEF during the study depending on the use of radiotherapy and chemotherapy regimen are shown in Table 4. During TT, a significant decrease in LVEF was observed in the whole group (Table 4). Moreover, the women receiving radiotherapy (202 patients [81%]) showed a significantly lower mean LVEF and a greater difference in LVEF between the subsequent measurements than those who did not receive the radiotherapy (Table 4). Lower LVEF at each time point during TT was found in the patients who received anthracyclines and taxanes in the adjuvant setting (as compared with those who received only anthracyclines) (P <0.001, Table 4), the patients with mitral or tricuspid regurgitation both at baseline and during or after TT (as compared with those with no regurgitation or regurgitation only during or after TT) (Figure 1C and 1D), and the patients with no aortic regurgitation or with regurgitation only during or after TT (as compared with those with aortic regurgitation both at baseline and during or after TT) (Figure 1E).
Parameter | Left ventricular ejection fraction, %, mean (SD) | P valuea | P valueb | P valuec | ||||||
Patients, n | Baseline before TT | During TT | After TT | |||||||
3 months | 6 months | 9 months | 12 months | |||||||
Abbreviations: see Table 2 | ||||||||||
Whole group | 249 | 68.1 (4.9) | 67.2 (4.9) | 66.6 (5.0) | 66.6 (4.8) | 66.0 (5.4) | 66.1 (5.3) | – | 0.004 | – |
Use of radiotherapy | ||||||||||
Whole group | 249 | 68.1 (4.9) | 67.2 (4.9) | 66.6 (5.0) | 66.6 (4.8) | 66.0 (5.4) | 66.1 (5.3) | – | – | – |
No radiotherapy | 47 | 68.4 (4.7) | 67.5 (4.7) | 68.0 (4.4) | 67.8 (3.6) | 67.9 (4.0) | 67.6 (4.3) | 0.06 | <0.001 | 0.003 |
Radiotherapy | 202 | 68.0 (5.0) | 67.1 (4.9) | 66.3 (5.1) | 66.3 (5.1) | 65.5 (5.7) | 65.8 (5.5) | |||
Use of anthracyclines | ||||||||||
Whole group | 242 | 68.0 (5.0) | 67.1 (4.9) | 66.5 (5.0) | 66.5 (4.9) | 65.9 (5.5) | 66.1 (5.4) | – | – | – |
Anthracyclines | 141 | 68.6 (4.8) | 68.0 (4.7) | 67.4 (4.9) | 67.2 (4.7) | 66.8 (5.3) | 66.7 (5.2) | 0.002 | <0.001 | 0.43 |
Anthracyclines + taxanes | 101 | 67.3 (5.1) | 66.0 (5.0) | 65.3 (4.8) | 65.6 (4.9) | 64.6 (5.5) | 65.1 (5.5) | |||
Finally, we assessed the associations between cardiovascular risk factors and the degree of valvular regurgitation and cardiac diameters. Older age was related to the presence of valvular fibrosis (59.8 [7.8] years vs 52.2 [10.1] years, P <0.001; Table 1), a higher degree of mitral regurgitation (P <0.001, Table 2), and a larger LA diameter (P <0.001, Table 3). HA was related to valvular fibrosis (P = 0.01, Table 1), a higher degree of mitral regurgitation (Table 2), a larger LA diameter at each time point during TT (P <0.001, Table 3), a higher increase in LA diameter (a greater difference between subsequent measurements) (P <0.001, Table 3), and a larger LV diameter at each time point during TT (P = 0.01, Table 3). IHD was related to a larger LA diameter during TT (P = 0.003, Table 3) and a larger RV diameter (P = 0.02, Table 3) at each time point. DM was related to a larger LA diameter at each time point during TT (P = 0.04, Table 3). Finally, high BMI was related to larger LA, LV, and RV diameters at each time point during TT (P <0.001, P <0.001, and P = 0.02, respectively, Table 3).
The patients who received high doses of anthracyclines showed a higher mean degree of aortic regurgitation during TT and a larger RV diameter during TT (P <0.001, Table 3).
No relationship between the valvular fibrosis and chemotherapy regimen or the use of radiotherapy and hormone replacement therapy was found.
Discussion
Myocardial and valvular fibrosis is the major process that contributes to impaired mechanical function of cardiomyocytes. Moreover, it affects heart muscle contraction and relaxation, influences the conduction system, and induces arrhythmia.10-14 It was postulated that cardiac fibrosis may be caused by the use of certain drugs or by some conditions such as HA, myocardial infarction, inflammation, or aging.15-17 In our study, valvular fibrosis was diagnosed during or after TT in 28.4% of patients with HER2‑positive BC who received trastuzumab as well as chemotherapy and radiotherapy in the adjuvant setting. In 15.6% of the women, fibrosis was found only after TT, while in 32 individuals (12.8%), it was diagnosed during and after TT. Valvular fibrosis did not resolve in any of the patients after completion of TT. However, the limitation of our study is the lack of data on cardiac fibrosis before the administration of the adjuvant chemotherapy. We noted no relationship between valvular fibrosis and chemotherapy regimen or the use of radiotherapy and hormone replacement therapy. Therefore, valvular fibrosis in our patients was most probably caused by degenerative processes related to aging and comorbidities rather than by the therapy itself. Nevertheless, fibrotic processes may be aggravated by the therapy, because 15.6% of the patients in our study developed fibrosis after TT. This hypothesis is also corroborated by a higher frequency of valvular fibrosis in older patients and individuals with HA. However, the lack of a clear relationship between the therapies used and valvular fibrosis diagnosed during or after TT does not exclude the possibility of late fibrotic complications or other damage to chest structures that may occur many years after anticancer treatment irrespective of the presence of early valvular fibrosis. Therefore, asymptomatic patients who receive chemotherapy, immunotherapy (trastuzumab in the adjuvant setting), or radiotherapy require close monitoring for possible cardiac complications.18-21
Another important issue in patients with HER2‑positive BC is the search for predictors of late cardiotoxicity. Among the studied treatment modalities, radiotherapy was identified as a significant risk factor for heart, valvular, pericardial, endocardial, and lung damage. Moreover, it was reported that patients who receive anthracyclines and irradiation of the mediastinum and heart are at high risk of valvular heart disease.22-26 However, progress in radiotherapy techniques allowed clinicians to use this modality with high accuracy, to protect the heart and lungs, as well as to lower the risk of cardiotoxicity. Importantly, in our study, the dosimetric parameter V30 did not exceed the safety level.
We observed that the patients who received a high dose of anthracyclines (>300 mg/m2) showed a larger RV diameter. This is in line with the findings of other authors,27,28 who reported anthracyclines to be associated with increased LV diastolic size and reduced wall thickness but not with aortic stenosis. Accordingly, it was hypothesized that myocardial toxicity of anthracyclines leads to ventricular dysfunction and secondary or functional valvular regurgitation. This is in agreement with our study, as we noted an increase in all cardiac chamber diameters (LV, LA, and RV) during TT. Moreover, LA and LV diameters were larger in the patients with mitral regurgitation, which is due to a change in LV geometry (LV dilatation), possibly with a concomitant increase in LV end‑diastolic pressure. Thus, in line with the hypothesis proposed by Aleman et al27 and Lund et al,28 it can be assumed that valvular insufficiency results from the valve annular dilatation, which is secondary to the dilatation of cardiac chambers and may by caused by cardiac edema. Moreover, in our study, the women with valvular fibrosis showed statistically higher degree of mitral regurgitation during TT. This is supported by Dickstein et al,12 who reported fibrosis to be related to asymptomatic followed by symptomatic heart failure. In our study, during TT (and at the same time after radiotherapy), we observed enlargement of all cardiac chambers (ie, an increase in LA, LV, and RV diameters), a decrease in LVEF, as well as a more prominent increase in the degree of valvular regurgitation (only in patients with regurgitation diagnosed during TT). Moreover, the presence of valvular insufficiency before, during, or after TT was associated with a larger LA and LV diameter during TT, as well as lower LVEF. Importantly, a decrease in LVEF during TT was also reported by other investigators.29,30
Some authors described subclinical changes after 3 months of TT, including deterioration of LV diastolic function and a small decrease in LVEF (with no overt symptoms).31,32 Furthermore, according to the literature, asymptomatic diastolic dysfunction may develop before the onset of LV contraction disorders.33 Increased heart chamber diameters, a reduction in LVEF, and an increase in the degree of valvular regurgitation observed during TT in our study might be due to radiotherapy- and chemotherapy‑induced cardiac damage. Early effects of both these treatments (applied before TT in our study group) include generation of reactive oxygen species leading to oxidative stress, followed by apoptosis, necrosis, cardiovascular damage, increased vascular permeability, and ultimately connective tissue edema.34-36 On the other hand, stromal edema might cause an increase in the diameter of all heart chambers. The edema of the cardiac wall (and an increase in its diameter) might be also due to increased transforming growth factor-β1 levels following radiotherapy or chemotherapy. This factor induces the synthesis of enzymes responsible for degradation of collagen, elastin, and other extracellular matrix components as well as deposition of large amounts of proteoglycan and glycosaminoglycan. These changes impair the homeostasis of the entire extracellular matrix that forms the connective tissue of the heart, ultimately leading to connective tissue edema. Fibrosis might constitute the late complication of the above process.37,38 In summary, stromal edema, as an early effect of radiotherapy and chemotherapy, might be responsible for an increase in heart chamber diameters and the resultant weakness of the heart muscle leading to a decrease in LVEF, as observed in our study. Cardiac dysfunction might be enhanced by the administration of trastuzumab, which blocks the HER2‑dependent cardioprotective pathway, thus leading to a further increase in heart chamber dimensions and a reduction in LVEF in the course of treatment, as confirmed by our study.5,39-41
The above mechanisms underlying therapy‑induced alterations in the heart are further confirmed by our finding that LVEF was lower both in the women receiving radiotherapy and in those receiving anthracyclines and taxanes (as compared with anthracyclines alone). According to the literature, taxanes increase the cardiotoxicity of anthracyclines, which is consistent with our results.42 Another finding that supports these observations is the fact that a larger RV diameter was related to the administration of high‑dose anthracyclines. Interestingly, in the patients with mitral, aortic, and tricuspid regurgitation diagnosed before TT, the degree of regurgitation remained stable during TT despite the fact that the baseline degree was higher than in the patients without valvular regurgitation at baseline. Consequently, in patients with regurgitation diagnosed during TT, a more prominent increase in the degree of valvular regurgitation was observed. Valvular regurgitation remained stable during TT in patients with regurgitation at baseline, which can be explained by the fact that they received cardioprotective drugs before and during TT. The patients diagnosed with HA usually received β-blockers and ACEIs. The remaining patients received low‑dose ACEIs as cardioprotection, and in selected patients (about 30%), low‑dose β-blockers were additionally used. It was reported that a therapy with ACEIs, β-blockers, and aldosterone receptor inhibitors as well as supervised physical training of moderate intensity during TT reduces heart remodeling and therefore the risk of death from heart failure.43,44 Thus, based on our findings and those of other authors, we may conclude that cardiac surveillance in patients with BC along with early pharmacological intervention is beneficial. The need for close monitoring of cancer patients after radiotherapy and chemotherapy was supported by Aleman et al,27 who studied patients with Hodgkin lymphoma treated with a combination therapy (mediastinal radiotherapy and anthracycline‑containing chemotherapy). After a median follow‑up of 18.7 years, the incidence of myocardial infarction and heart failure was significantly increased (standardized incidence ratios of 3.6 and 4.9, respectively) as compared with the general population. Concomitant administration of anthracycline chemotherapy increased the incidence of heart failure by 29%. In a Norwegian study of patients with Hodgkin lymphoma treated with radiotherapy and anthracyclines, 31% of participants had moderate valvular insufficiency at 10 years, and after a mean follow‑up of 22 years, progressive valvular disease was revealed.28,45 Of patients with moderate regurgitation at first assessment, 33% developed severe regurgitation or required valve replacement. In addition, 39% of these patients had aortic stenosis (severe in some cases).
In our study, older age (>54 years) was associated with a significantly higher degree of mitral regurgitation and more dynamic changes in regurgitation, as well as a significantly larger LA diameter. Moreover, the patients with valvular fibrosis were significantly older than those without it. Our results suggest that women older than 50 years are at the highest risk of severe valvular disease during cancer treatment. Therefore, they require careful and regular monitoring as part of a long‑term care. This conclusion is also supported by other researchers.46
In our study, a slight but significant increase in the RV diameter was observed during TT. It was previously reported that 40% of patients treated with TT (with or without anthracyclines) who developed cardiotoxicity (diagnosed based on LVEF reduction) had RV dysfunction. The coexistence of LV and RV dysfunction was associated with a greater difficulty to restore ventricular function.47 This suggests that the adverse effects of cancer treatment influence the entire myocardium. Therefore, the assessment of cardiac mechanical function on the basis of LVEF alone (regardless of the diagnostic tools used, such as echocardiography, perfusion scintigraphy, and others) is not sufficient to identify subtle subclinical changes in the whole myocardium, as suggested by previous research.48 This is confirmed by our study, as we observed numerous such changes in cardiac structure and function.
We identified the following risk factors for the development of early asymptomatic cardiac dysfunction during cancer therapy: age, HA, IHD, DM, high BMI, and valvular insufficiency. Moreover, older age (defined as a higher mean age of patients) and HA were related to valvular fibrosis, a significantly higher degree of mitral insufficiency during TT, and larger LA and LV diameters during TT. Finally, the patients with IHD, DM, and high BMI had a significantly larger diameter of all heart chambers during TT. These findings are in line with a previously described profile of high‑cardiovascular‑risk women aged over 50 years with comorbidities who received an aggressive treatment (radiotherapy with irradiation of the heart, chemotherapy with anthracyclines), resulting in a high risk of cardiac complications.46
In conclusion, this study identified subclinical cardiac changes in patients with HER2‑positive BC during and after TT. Although asymptomatic, these changes may predict significant late cardiac complications. Early identification of cardiotoxicity can improve the patient prognosis by a proper therapeutic decision‑making in terms of subsequent chemotherapy as well as adequate pharmacological and nonpharmacological interventions aimed at preventing cardiac complications. Multidisciplinary teams including cardiologists, physical therapists, and oncologists are needed to provide optimal care to individuals with BC at risk of cardiotoxicity. Finally, successful treatment of HER2‑positive BC requires careful cardiac monitoring both during and after the therapy.47,49,50
- Denduluri N, Chavez‑MacGregor M, Telli ML, et al. Selection of optimal adjuvant chemotherapy and targeted therapy for early breast cancer: ASCO clinical practice guideline focused update. J Clin Oncol. 2018; 36: 2433‑2443. | Crossref
- Slamon D, Eiermann W. Robert N, et al; Breast Cancer Inernational Reaserch Group. Adjuvant trastuzumab in HER2‑positive breast cancer. N Engl J Med. 2011; 365: 1273‑1283. | Crossref
- Perez EA, Romond EH, Suman VJ, et al. Trastuzumab plus adjuvant chemotherapy for human epidermal growth factor receptor 2‑positive breast cancer: planned joint analysis of overall survival from NSABP B‑31 and NCCTG N9831. J Clin Oncol. 2014; 32: 3744‑3752. | Crossref
- Moja L, Tagliabue L, Balduzzi S, et al. Trastuzumab containing regimens for early breast cancer. Cochrane Database Syst Rev. 2012; 2012: CD006243. | Crossref
- Martín M, Esteva FJ, Alba E, et al. Minimizing cardiotoxicity while optimizing treatment efficacy with trastuzumab: review and expert recommendations. Oncologist. 2009; 14: 1‑11. | Crossref
ARTICLE INFORMATION