A rare case of aortic involvement in microscopic polyangiitis evaluated using contrast‑enhanced ultrasound, superb microvascular imaging, and magnetic resonance imaging



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
A rare case of aortic involvement in microscopic polyangiitis evaluated using contrast‑enhanced ultrasound, superb microvascular imaging, and magnetic resonance imaging
Aortitis is a broad term comprising numerous conditions leading to inflammatory infiltration of the aorta. Clinical presentations vary among the etiologies, with Takayasu disease and giant cell arteritis being the most common entities that affect large vessels. Limited evidence supports the possibility of aortic involvement in antineutrophil cytoplasmic antibody (ANCA)–associated small‑vessel vasculitis, for example, microscopic polyangiitis (MPA). Early diagnosis may be challenging; however, it is of particular importance in light of possible life‑threatening complications.1
We present the case of a 79‑year‑old male patient with MPA diagnosed in 2018, with pulmonary and renal involvement and strongly positive perinuclear ANCA (p‑ANCA) titer. After induction of a remission therapy (glucocorticoids, mycophenolate mofetil [MMF]), a negative conversion of p‑ANCA occurred. Three years later, the patient reported recurrent night‑time sweats with fever up to 39 oC, and substantial weight loss (4 kg) 3 months prior to readmission. Blood and urine samples were negative for major pathogens. Laboratory indices were as follows: C‑reactive protein, 80 mg/l (reference range, 0–5 mg/l), sedimentation rate, 69 mm/h (reference range <15 mm/h), p‑ANCAs, 33.7 U (positive result >30 U).
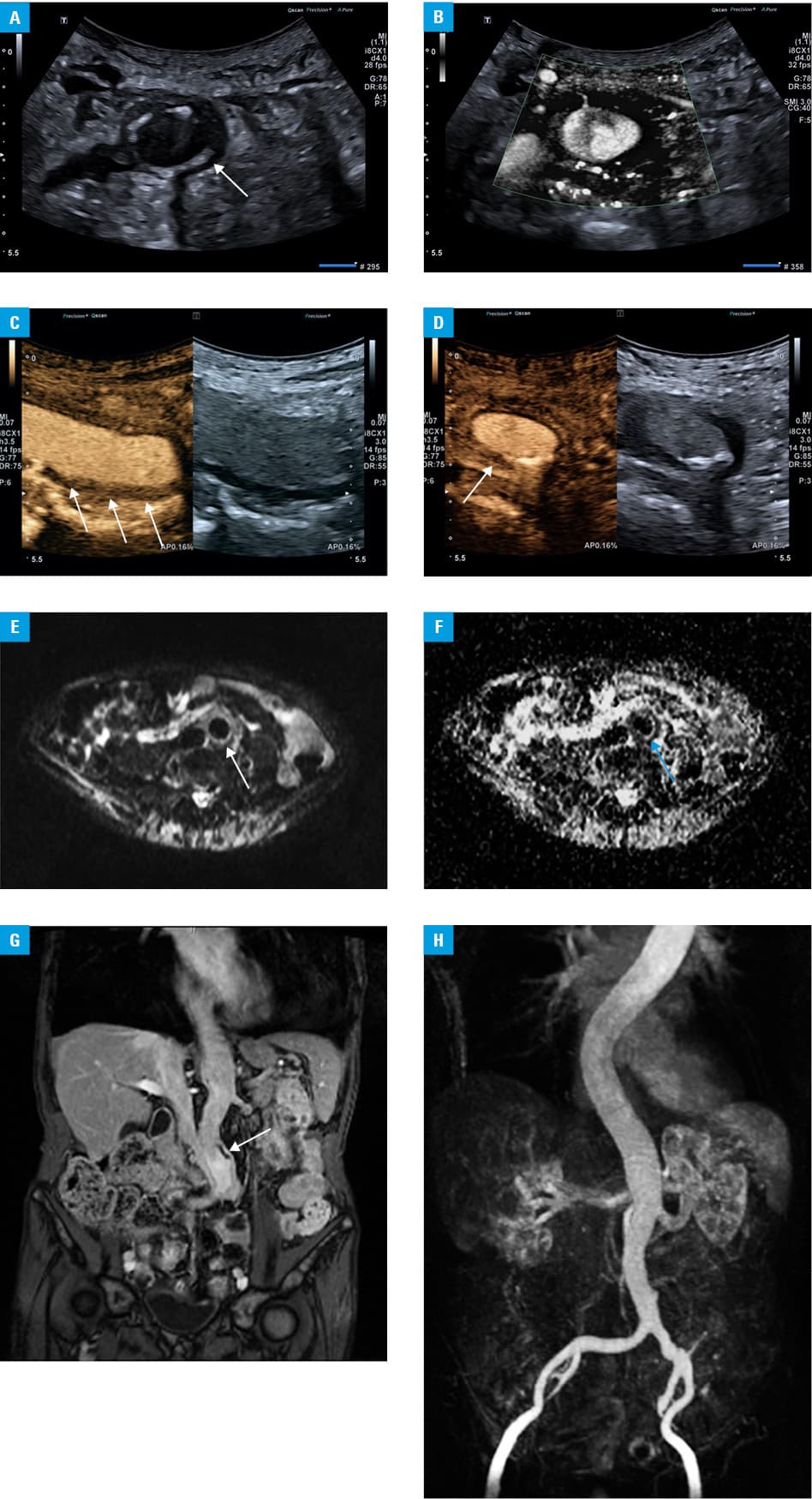
Computed tomography (CT) of the chest confirmed a stable aneurysm of the ascending aorta (54 mm in diameter) diagnosed previously. Abdominal ultrasound (US) and magnetic resonance imaging (MRI) were applied to evaluate the involvement of the descending aorta and its major branches, among others. US was performed using Canon Aplio i700 (Canon Medical Systems, Otawara, Japan) with a 4.0 MHz i8CX1 transducer, and standard abdominal and vascular presets. B‑mode presentation revealed hypoechoic wall thickening (up to 5 mm) along the distal aorta and the proximal left common iliac artery, consistent with inflammatory infiltration (Figure 1A). No‑flow signals were observed within the aortic wall on Doppler imaging. However, superb microvascular imaging (SMI) visualized singular signals indicative of neovascularization (Figure 1B). Next, 1.5 ml of a contrast agent (SonoVue, Bracco, Milan, Italy) followed by 10 ml of 0.9% saline flush were administered intravenously to perform contrast‑enhanced US (CEUS), which showed robust enhancement within the hypoechoic aortic rim (Figure 1C and 1D), suggestive of an active inflammation. The aortic and iliac lumina were preserved, with no pathological dilatation or stenosis. The US findings were verified with MRI, which showed restricted diffusion within the aortic wall, as well as pathological contrast enhancement (Figure 1E–1G). Maximum intensity projection reconstructions of contrast‑enhanced 3‑dimensional images confirmed normal lumen and patency of the affected vascular segments (Figure 1H).
The patient was treated with intravenous methylprednisolone (total dose, 320 mg), oral prednisone, MMF, and low‑dose aspirin. He was discharged home in a stable condition, with recommendations to continue aspirin, MMF, and prednisone.
The diagnosis of p‑ANCA–associated aortitis is based on detection of ANCAs by the enzyme‑linked immunosorbent assay and indirect immunofluorescence, as well as diagnostic imaging—most often contrast‑enhanced MRI/CT, MRI/CT angiography, and Doppler ultrasonography. In the presented case, CEUS complemented with SMI proved to be at least equally efficient as MRI in assessing the disease burden within the descending aorta and its major branches, showing a high diagnostic efficacy of this modality in the diagnosis of inflammatory vascular lesions.
To our best knowledge, this is the first description of a confirmed p‑ANCA–associated aortitis documented with CEUS, SMI, and MRI. Until 2019, merely 10 cases of aortic involvement in ANCA‑associated vasculitis (AAV) were reported in the literature. AAV is a necrotizing inflammation primarily affecting small vessels, thus presenting as multi‑organ disease.2 Large vessels are rarely affected, and the pathomechanism resembles small‑vessel disease. Although there is a possibility of overlap, initial involvement of the intima advocates for a different origin of AAV than of large‑vessel vasculitis, in which the media and adventitia are primarily affected. Additionally, periaortic infiltration is characteristic of AAV.3
- Shchetynska‑Marinova T, Amendt K, Sadick M, et al. Aortitis – an interdisciplinary challenge. In Vivo. 2021; 35: 41‑52. | Crossref
- Skeik N, Hari G, Nasr R. Aortitis caused by antineutrophil cytoplasmic antibodies (ANCA)-associated vasculitis: a case‑based review. Rheumatol Int. 2019; 39: 1983‑1988. | Crossref
- Tariq E, Nishanth K, Arshid A, et al. Aortic involvement in antineutrophil cytoplasmic antibodies vasculitis, a coincidence or a real association? Cureus. 2020; 12: e9690. | Crossref
ARTICLE INFORMATION