Dyslipidemia as an important risk factor for gastric adenomatous polyps in patients with gastric polyps



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Dyslipidemia as an important risk factor for gastric adenomatous polyps in patients with gastric polyps
Introduction
As a true neoplasm, gastric adenomatous polyp (GAP) is a precursor of gastric cancer and is closely associated with synchronous or metachronous gastric adenocarcinoma.1 To obtain an early diagnosis of GAP, patients with gastric polyps should undergo precise endoscopic examination, including magnifying endoscopy, chromoendoscopy, endoscopic ultrasonography, and endoscopic biopsy. In addition, complete removal of GAP is warranted to prevent gastric tumorigenesis.2 Although endoscopic biopsy significantly improves the diagnostic accuracy for GAPs, the discrepancy rate between the results of histopathological analysis of the endoscopic forceps biopsy specimens and the resected gastric polyps, including GAPs, is 39.2%.3 Therefore, in some patients with GAPs, endoscopic biopsy with forceps may not be sufficient to serve as a basis for a precise diagnosis and therapeutic planning. Further investigation is needed to identify the potential factors related to GAPs, which may facilitate the diagnosis and help prevent gastric cancer. Metabolic syndrome is a well‑known risk factor for the development of gastric cancer. Since GAP is one of the precancerous diseases potentially leading to gastric cancer, it is important to explore its relationship with metabolic syndrome. Few studies have been carried out on the risk factors for GAPs, especially ones incorporating the indicators of metabolic syndrome. The aim of our study was to identify the risk factors for GAPs, and particularly, to study the relationship between GAPs and biomarkers of metabolic syndrome, including serum levels of apolipoprotein A1 (APOA1), apolipoprotein B (APOB), triglycerides, and total cholesterol (TC).
Patients and methods
The study was approved by the Ethics Committee of the Suining Central Hospital and all participants were informed about the study by telephone. We conducted a retrospective, cross‑sectional survey of inpatients with gastric polyps treated at the Suining Central Hospital between 2019 and 2020. A total of 1064 inpatients were enrolled, including 106 patients with histopathologically diagnosed GAPs and 958 patients with histopathologically diagnosed gastric nonadenomatous polyps (GNAPs). All participants underwent precise endoscopic examination and complete endoscopic resection of the gastric polyps. Detailed clinical characteristics and laboratory data were obtained by our clinical specialists. The GAP group and the control group were matched for age and sex at a ratio of 1:4.
Statistical analysis
Univariable analysis and multivariable logistic regression analysis were performed to identify the risk factors for GAPs, using the χ2 test and a forward stepwise logistic regression model, respectively. All participants were divided into 4 groups, according to the quartile values of serum APOA1 levels. The χ2 test was used to check the association between the prevalence of GAPs and the quartiles of serum APOA1 levels. The receiver operating characteristic (ROC) curves were used to evaluate the cutoff value of serum APOA1 levels for predicting GAP. Descriptive data were presented as a mean (SD) or median (interquartile range [IQR]), depending on the distribution of the variables. Normally distributed continuous variables were compared between the groups using the unpaired t test. The Mann–Whitney test was used for comparisons of non‑normally distributed data. Categorical variables were compared using the χ2 test. P values lower than 0.05 were considered significant. The SPSS software, version 26.0 was used for data analysis (IBM SPSS Inc., Chicago, Illinois, United States).
Results
A total of 106 patients with GAPs and 958 patients with GNAPs were included in the present study (Supplementary material, Figure S1). After matching for age (+/– 5 years) and sex, 424 patients with GNAP were selected as a control group. The GAP group and the control group had the same distribution of sex (P = 0.13) and there were no significant differences in age between the 2 groups (median [IQR], 57.1 [49.9–66.4] years vs 59.5 [50.4–68.0] years; P = 0.28).
To determine the differences in serum APOA1 levels between the patients with GAPs and controls, we compared the serum levels of APOA1 in both groups (a subpopulation of 530 participants). The results indicated that the peak serum level of APOA1 was significantly higher in the GAP group than in the control group, suggesting the distribution of serum APOA1 levels has shifted toward higher values in the patients with GAPs as compared with controls (Supplementary material, Figure S2A). When the mean serum APOA1 levels in the 2 groups were compared, they were found to be significantly higher in the GAP group (mean [SD], 1.54 [0.253] vs 1.431 [0.250] g/l, P <0.01, Supplementary material, Figure S2B).
Data from all participants (n = 1064) served to construct an ROC curve (Supplementary material, Figure S3), which reflected the cutoff value of the serum APOA1 level for GAP, with an area under the ROC curve of 0.627.
Univariable analysis and multivariable logistic regression analysis were performed in the subpopulation of 530 participants. Univariable analysis (Figure 1A) showed that, among the factors evaluated, APOA1 equal or greater than 1.6 g/l (odds ratio [OR], 2.184; 95% CI, 1.399–3.408), TC equal or greater than 5.7 mmol/l (OR, 0.242; 95% CI, 0.109–0.537), Helicobacter pylori infection (OR, 2.246; 95% CI, 1.459–3.459), and alcohol consumption (OR, 2.493; 95% CI, 1.617–3.844) were all significantly associated with GAP. Multivariable analysis (Figure 1B) showed that APOA1 equal or greater than 1.6 g/l (OR, 2.408; 95% CI, 1.501–3.861), TC equal or greater than 5.7 mmol/l (OR, 0.259; 95% CI, 0.114–0.591), H. pylori infection (OR, 1.959; 95% CI, 1.249–3.071), and alcohol consumption (OR, 2.199; 95% CI, 1.398–3.460) were independent predictors of GAP. Based on the data from all 1064 participants, H. pylori–positive patients showed slightly higher APOA1 values than those without the infection (mean [SD], 1.435 [0.256] vs 1.423 [0.245] g/l) but the difference was not significant (P = 0.44).
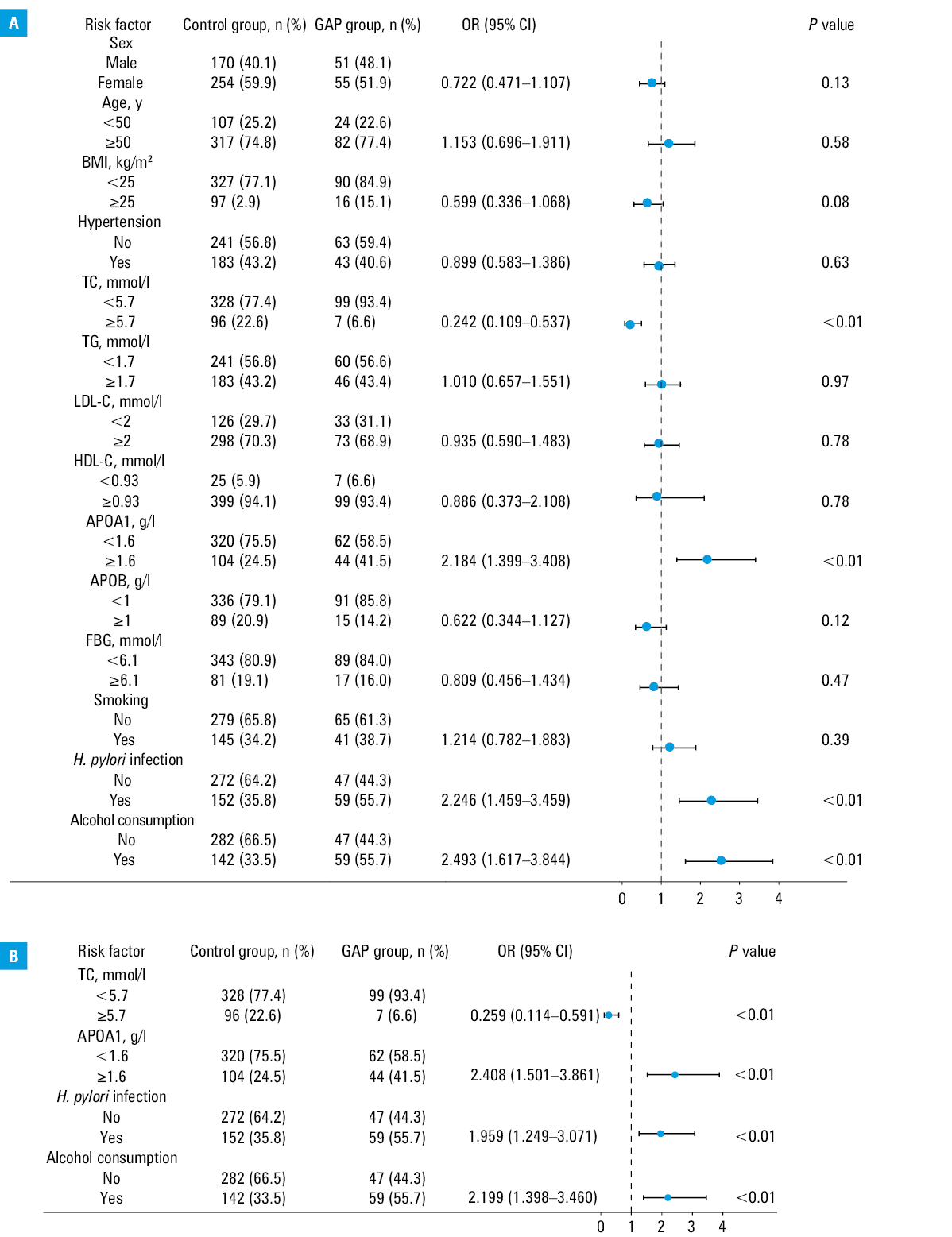
Abbreviations: APOA1, apolipoprotein A1; APOB, apolipoprotein B; BMI, body mass index; FBG, fasting blood glucose; GAP, gastric adenomatous polyps; HDL‑C, high‑density lipoprotein cholesterol; LDL‑C, low‑density lipoprotein cholesterol; TC, total cholesterol; TG, triglycerides
To further clarify the association between the serum APOA1 level and the prevalence of GAP in the hospitalized patients with gastric polyps, all 1064 participants were divided into 4 groups according to quartile values of serum APOA1 levels: up to 1.27, between 1.28 and 1.44, between 1.45 and 1.60, and equal or greater than 1.61 g/l for quartiles 1, 2, 3, and 4, respectively. A positive association between the prevalence of GAP and quartiles of serum APOA1 levels was observed. The prevalence of GAPs among the participants with serum APOA1 levels in the first and second quartiles was 5.6% and 7.6%, respectively. However, the prevalence in the participants with serum APOA1 levels in quartile 3 and 4 tended to be higher, namely, 10.2% and 16.7%, respectively (P <0.01, Supplementary material, Table S1).
Discussion
Our hospital‑based observational study was the first to investigate the relation between GAP and indicators of metabolic syndrome in patients with gastric polyps. A prior study performed to determine the risk factors for gastric neoplasm found that patients with GAP had a higher frequency of metabolic syndrome, including dyslipidemia.4 Our findings based on data from the patients with gastric polyps suggested that dyslipidemia, alcohol consumption, and H. pylori infection may independently predict the risk of GAP development, and serum APOA1 levels may be useful in the diagnosis of GAP.
APOA1, the major protein component of high‑density lipoprotein cholesterol, is a cofactor for lecithin cholesterol acyl transferase, which may promote the formation of plasma cholesteryl esters and induce cholesterol efflux from peripheral tissues to the liver for excretion.5 Recent studies revealing alterations of APOA1 levels during the progression of various types of tumor suggest that the serum APOA1 level may represent a potential biomarker for better estimation of early cancer diagnosis and cancer risk.6-9 In our study, the elevated serum level of APOA1 was demonstrated to be associated with the incidence of GAP; therefore, it can be considered an independent predictor of an increased risk of GAP in patients with gastric polyps. Ma et al10 found that the preoperative APOB to APOA1 ratio was a prognostic factor for gastric cancer. In our study, the control group of patients with GNAPs had a higher APOB to APOA1 ratio than the group of patients with GAP (data not shown). However, we could not determine whether the APOB to APOA1 ratio was a prognostic indicator for GAP because the length of follow‑up from the time of GAP diagnosis was too short. Although there are many studies suggesting an inverse association of serum APOA1 levels with the progression of various cancers, a significant positive relationship between serum APOA1 levels and early‑stage gastric adenocarcinoma has been observed.11 Because early‑stage gastric adenocarcinoma and its obligate precursors, GAPs, have many similar biological features, serum APOA1 levels may also be upregulated in patients with GAPs. Additionally, our results suggested an inverse relationship between serum TC levels and the risk of GAPs (data not shown). This result might be partly due to the elevated serum level of APOA1 in the patients with GAPs.
Some studies showed that alcohol consumption is a significant risk factor for gastric neoplasms, including gastric adenoma.12,13 In our study, a positive relationship between alcohol consumption and GAPs was found, which is in line with previous literature reports. The relationship between H. pylori infection and GAPs is controversial. It was observed that H. pylori–positive individuals tended to have a higher frequency of foveolar‑type gastric adenoma and that H. pylori infection might promote the progress of gastric adenoma.14 On the contrary, some studies did not confirm any association between H. pylori infection and gastric adenoma.15 Our data suggested that H. pylori infection was positively associated with GAPs, but the exact pathogenesis needs further investigation.
The main limitation of the current study is the small sample size, due to which we might have failed to identify some significant risk factors for GAPs. Owing to the relatively low prevalence of GAPs, it was difficult to find a great number of patients eligible for inclusion in this study. For this reason, further multicenter studies with larger samples are needed. The present data are not sufficient to support the hypothesis that the level of apolipoproteins is related to the size of polyps, histological structure, dysplasia, or atrophic gastritis. Additional studies in larger populations may help establish these links. Also, histopathological examination of the gastric mucosa should be incorporated in subsequent research studies. Based on our results, it can be inferred that APOA1 may be related to the malignant progression of GAPs. Patients with synchronous and metachronous gastric cancer should be included in further analyses. Moreover, subsequent longitudinal, observational studies in patients with an increased risk for GAPs and gastric cancer after GAP removal should be performed to evaluate the necessity of endoscopic follow‑up.
In conclusion, our study showed that dyslipidemia, alcohol consumption, and H. pylori infection independently increased the risk of GAP development and the serum APOA1 level showed a close positive relation with the prevalence of GAPs in the patients with gastric polyps. Further studies on the mechanism of this relation may be of great clinical importance for the diagnosis, prevention, and management of GAPs.
- Borch K, Skarsgård J, Franzén L, et al. Benign gastric polyps: morphological and functional origin. Dig Dis Sci. 2003; 48: 1292‑1297. | Crossref
- Choi CW, Kang DH, Kim HW, et al. Endoscopic submucosal dissection as a treatment for gastric adenomatous polyps: predictive factors for early gastric cancer. Scan J Gastroenterol. 2012; 47: 1218‑1225. | Crossref
- Sung HY, Cheung DY, Cho S‑H, et al. Polyps in the gastrointestinal tract: discrepancy between endoscopic forceps biopsies and resected specimens. Eur J Gastroenterol Hepatol. 2009; 21: 190‑195. | Crossref
- Park MJ, Kim DH, Lim SH, et al. Features of gastric neoplasm detected during the screening examination. Gut Liver. 2007; 1: 33‑39. | Crossref
- Flores R, Jin X, Chang J, et al. LCAT, ApoD, and ApoA1 expression and review of cholesterol deposition in the cornea. Biomolecules. 2019; 9: 785 | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION