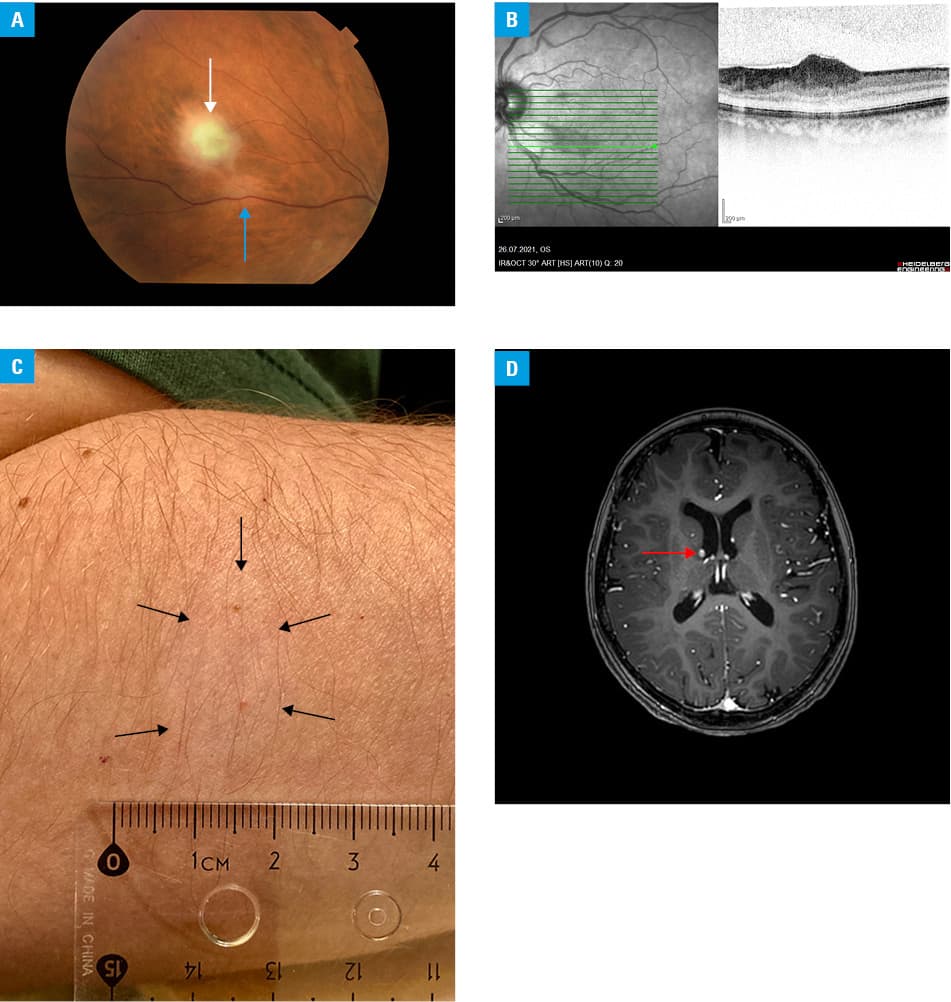
A 53‑year‑old woman was urgently referred to the hospital with a suspicion of chorioretinitis after retinal lesions had been found by an ophthalmologist during a routine eye examination. On admission, full visual acuity in both eyes (20/20) was noted. The anterior segments of both eyes did not show any symptoms suggesting ongoing or past inflammation, and there were no inflammatory cells in the vitreous chamber. In the fundus examination, 3 grayish areas were observed in the right eye and a single similar area was found in the left eye. The lesions were the size of 1.5 disc diameters, were domed in shape, and had blurred margins. In the left eye, there was also a round area of hypopigmentation observed in the retina (Figure 1A). Optical coherence tomography confirmed that the described changes were located in the retinal nerve fiber layer (Figure 1B). During history taking, the patient stated that she had been diagnosed with “some disease” as a child but did not remember any details. The disease did not cause any ailments; therefore, she did not see the need to expand the diagnostics or to continue with follow‑up visits with any specialists.
Further diagnostic workup was planned, and tuberous sclerosis complex (TSC) was suspected based on the fact that the retinal lesions morphologically resembled hamartomas. TSC is an autosomal dominant disorder caused by mutations in the TSC1 or TSC2 gene.1 According to current recommendations, the diagnosis should be made based on clinical criteria (Supplementary material, Table S1). TSC is characterized by a high variability of symptoms, most of which are not pathognomonic. To make a definite diagnosis, a patient must present at least 2 major features, or 1 major and 2 minor features at the same time. Genetic testing may be useful to confirm the diagnosis in individuals who do not fulfill the definitive clinical criteria.2
Our patient met 3 major and 1 of the minor criteria. On detailed general examination, she was found to have 7 hypomelanotic macules / spots with a diameter of several millimeters in various places on the skin (Figure 1C). She also had subependymal nodules along the wall of the ependymal lining of the lateral and third ventricles on magnetic resonance imaging of the brain (Figure 1D). The dome‑shaped retinal lesions, primarily described as retinal inflammation, were in fact multiple retinal hamartomas—specific enough to be considered a major TCS criterion. A round area of hypopigmentation in the retina, found in the left eye, was a retinal achromic patch, one of the minor criteria for TCS diagnosis. No changes in the lungs or kidneys were found on imaging studies (computed tomography and magnetic resonance imaging). Regular follow‑up was recommended. Additionally, both the patient and her immediate family were referred for genetic testing.
The severity of TSC varies, and the symptoms of the disease are age‑dependent; for example, epilepsy, facial angiofibroma, and hypomelanotic macules usually occur in children, while renal angiomyolipoma and pulmonary lymphangioleiomyomatosis typically manifest in adulthood.1 Our patient was not a typical, textbook case of TSC. In the sixth decade of life, she still did not experience most of the serious symptoms. Although the disease was probably diagnosed in childhood, the patient was not under medical supervision. An accidental finding during an ophthalmological examination enabled the final diagnosis and further necessary diagnostic procedures.
- Henske EP, Józwiak S, Kingswood JC, et al. Tuberous sclerosis complex. Nat Rev Dis Prim. 2016; 2: 16035. | Crossref
- Northrup H, Krueger DA; International Tuberous Sclerosis Complex Consensus Group. Tuberous sclerosis complex diagnostic criteria update: recommendations of the 2012 International Tuberous Sclerosis Complex Consensus Conference. Pediatr Neurol. 2013, 49: 243‑254.
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION