Atherosclerotic cardiovascular disease burden in patients with familial hypercholesterolemia: interpretation of data on involvement of different vascular beds
Key words: atherosclerosis, cardiovascular disease, familial hypercholesterolemia



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Atherosclerotic cardiovascular disease burden in patients with familial hypercholesterolemia: interpretation of data on involvement of different vascular beds
Familial hypercholesterolemia (FH) is a monogenic, autosomal dominant disorder that results in a rise of low‑density lipoprotein cholesterol (LDL‑C) and markedly increased risk of premature atherosclerotic cardiovascular disease. FH is relatively common, treatable, and its clinical course can be improved through early detection and timely initiation of lipid‑lowering medications. The clinical picture of FH is highly variable, with a heterogeneous phenotype even within a single family, ranging from patients with very early onset of major cardiovascular events to those who do not develop overt cardiovascular disease even at an old age. We summarized studies indicating that atherosclerotic involvement in the coronary arteries and lower extremities is higher in FH patients than in the general population. There is a paucity of data regarding the relationship between FH and the incidence of atherosclerosis in other vascular beds. There are no studies systematically evaluating several vascular beds in asymptomatic patients with FH. Providing a systematic characteristic of patients with FH with respect to the presence and extent of atherosclerotic lesions in different vascular beds may have implications for daily practice not only for patients with FH but also for a larger number of patients with very high plasma LDL‑C concentrations.
Introduction
Atherosclerotic cardiovascular disease (ASCVD) remains the leading cause of death worldwide and current guidelines emphasize a fundamental role of primary prevention of ASCVD.1,2 Familial hypercholesterolemia (FH) is a monogenic, autosomal dominant disorder that from birth results in elevated low‑density lipoprotein cholesterol (LDL‑C) and markedly increased risk of premature ASCVD.3 In contrast to earlier reports, contemporary epidemiological studies propose that FH is twice as common as previously suggested and affects more than 25 million people worldwide. A recent extensive systematic review and meta‑analysis of 62 studies with over 7.3 million patients indicated an overall incidence of FH of 1:311 in the general population, with no significant differences between various geographical regions of the world.4 In a meta‑analysis of 6 population‑based studies in Poland, prevalence of FH based on the Dutch Lipids Clinics Network (DLNC) criteria was estimated as 1 in 250 adults.5 In a study that included a representative sample of adult patients with hypercholesterolemia in outpatient clinics in Poland, FH based on DLNC criteria was diagnosed in 3.6% of the examined patients.6
Once FH was recognized a common and treatable disease, whose clinical course can be improved through early detection and timely initiation of lipid‑lowering medications, WHO prepared a report in 1998 focused on the implementation of multiple approaches to FH patients.4,7 However, despite the recommendations to raise awareness and provide effective treatment, FH remains usually undiagnosed and untreated worldwide, with only about 1% of potential cases detected.4,7
Early reports, based on selected populations, limited number of data and different diagnostic criteria provided substantial variations in the prevalence, diagnostic and treatment patterns, and clinical status of FH patients.4,7 However, a few countries, including the United Kingdom and the Netherlands, implemented nationwide programs based on more systematic approaches to identify and treat individuals with FH. Also, international registries, including the European Atherosclerosis Society Familial Hypercholesterolemia Studies Collaboration (FHSC) and the Cascade Screening for Awareness and Detection (CASCADE) are valuable resources to increase FH awareness, identify care gaps, and monitor outcomes. The FHSC global registry provided a unique platform for worldwide surveillance of FH. It revealed that FH is diagnosed late, and that the control of LDL‑C levels falls far below the recommendations, partly due to inadequate drug treatment.8
FH is most often due to causal variants within the genes regulating low‑density lipoprotein receptor (LDLR) pathway, including LDLR, apolipoprotein B (APOB), and proprotein convertase subtilisin / kexin type 9 (PCSK9).3,9 A population‑based study from Denmark published in 2016 found that LDLR, APOB, and PCSK9 mutations affect 1 in 217 people in the general population. The most optimal threshold for plasma LDL‑C concentration to discriminate between the mutation carriers and noncarriers was 4.4 mmol/l (170 mg/dl).10 A mutation in the gene encoding the LDLR protein is the most common and accounts for over 75%–95% cases with a documented genetic background.11,12 Other mutations are less common: APOB 2%–11% and PCSK9 below 1%. In some patients (10%–40%) with a clinical diagnosis of FH none detectable causal mutations are found.13 A study from Poland showed that in a group of 193 unrelated adult patients with a clinical diagnosis of FH based on DLCN criteria, LDLR or APOB mutations were found in 41% of the examined individuals.14
However, contemporary, large, genetic studies documented factors other than the LDLR pathway that must be involved in the regulation of plasma LDL‑C concentration. It was reported that the pathogenic variants in the key genes of the LDLR pathway account for only a small portion of even severe hypercholesterolemia. Therefore, it may be concluded that a genetic diagnosis of FH does not correspond to FH revealed clinically and vice versa, that is, FH identified clinically does not correspond to FH diagnosed based on LDL‑C concentration.3
Of note, LDL‑C concentration may be within normal range or only modestly elevated in patients with causal genetic variants, indicating that the major factor affecting the LDLR pathway function remains unknown. Therefore, it may be suggested that the recent studies demonstrating little overlap between the 3 FH defining characteristics challenge the conventional definition of FH linking clinical characteristics, genetic variant status, and marked hypercholesterolemia.15
Familial hypercholesterolemia and coronary artery disease
Most data on the association between FH and ASCVD refer to the development of atherosclerotic lesions within the coronary arteries and their consequences, that is, myocardial infarction and death. The risk of developing the coronary artery disease (CAD) in FH patients is approximately 13‑fold higher than in the general population.13,16,17 CAD is evident in patients with FH from the age of 17 in men and the age of 25 in women, and up to 25% of the adolescents with FH present coronary artery calcification.17,18
A few studies systematically assessed FH patients for the presence and severity of atherosclerotic coronary lesions. They usually employed calcium artery calcium score (CACS) for assessment of the presence and calculation of number of coronary segments with atherosclerotic lesions for evaluation of coronary atherosclerosis severity.19-25
Although a few new plaque characteristic features associated with atherosclerosis progression and culprit lesions are now identified, these characteristics were not sufficiently evaluated in patients with FH.26-28 In patients with FH and established ASCVD, CACS higher than 0 is found in almost all individuals (96%).29 However, 40%–45% of middle aged (36 to 51 years) FH patients without ASCVD showed CACS equal to 0.29,30
Despite the above, it must be noted that arterial calcification index of 0 does not exclude the presence of noncalcified atherosclerotic plaques. It should be also stressed that the addition of CACS to the ASCVD event risk evaluation in FH patients improves the risk assessment.29
Only a small number of studies systematically assessed the severity of atherosclerotic coronary lesions in FH patients. Neefjes et al21 included 101 asymptomatic patients with FH and 126 patients with nonanginal chest pain (mean age, 53 and 56 years, respectively). Only 15% of patients with FH did not have any signs of CAD, as compared with 33% of patients in the control group. Also, the severity and extent of coronary atherosclerosis on a per patient and per segment basis were significantly higher in FH patients. Asymptomatic obstructive CAD was found in 26% of FH individuals.
A study of statin‑treated asymptomatic FH patients aged 40 years and older demonstrated that LDLR‑negative patients, as compared with LDLR‑positive patients, had a higher median number of diseased coronary segments (4 vs 2), higher median integrated sum of stenosis severity (score 1–3), and higher number of coronary artery lesions (11 vs 6). This study showed that despite statin treatment, asymptomatic middle‑aged FH patients exhibited a high extent of coronary atherosclerosis. The difference in the extent of coronary atherosclerotic lesions in the patients with and without the LDL‑R gene mutation may be due to the fact that the study included asymptomatic patients over 40 years of age, and excluded those individuals with the LDL‑R gene mutation and severe atherosclerotic lesions in whom ASCVD was diagnosed before the age of 40.31
The study by Tada et al32 that included FH patients without overt ASCVD showed that coronary artery plaque burden was associated with coronary events in the follow‑up. Almost 1 in 3 patients in this cohort was characterized by a plaque burden score of 3.35 or higher (raw score, 28.5) that was identified as an optimal cutoff for a worse prognosis. The authors also documented that coronary atherosclerosis may start to develop on an average age of 23 to 34 years in men and women with FH. A Spanish study33 included 259 patients with genetically confirmed FH without overt clinical cardiovascular disease. The median coronary plaque burden was 25% and the major cardiovascular risk factors, that is, smoking, hypertension, and especially diabetes mellitus were found to modify the plaque burden. Additionally, a long‑term 3‑year follow‑up showed a correlation between the baseline plaque burden and the risk of cardiovascular events. It is of interest that patients with genetically confirmed diagnosis of FH are characterized by a higher frequency and burden of coronary atherosclerotic plaques than the patients without confirmed mutations but with clinical diagnosis of FH.34
A large UK Biobank study35 included patients at comparable levels of LDL‑C at baseline with monogenic FH, polygenic hypercholesterolemia, and hypercholesteremia of undetermined cause. The patients with monogenic FH were significantly more likely to experience ASCVD event at the age of 55 years or earlier than those without monogenic FH. Moreover, in the patients with comparable plasma LDL‑C concentrations vs those with hypercholesterolemia without an identified genetic cause, both monogenic and polygenic hypercholesterolemia were significantly associated with a higher risk of ASCVD events.
Of note, higher prevalence of coronary ectasia in heterozygous FH vs other patients with coronary atherosclerosis was reported.36 This study and a more recent one37 revealed that the presence of coronary ectasia, among other factors such as hypertension and body mass index, significantly and independently correlated with higher low- to high‑density lipoprotein cholesterol ratio.
Familial hypercholesterolemia and aortic valve calcification and stenosis
Aortic valve calcification (AoVC) occurs in over 50% of people aged 75 years and older and is associated with an increased risk of cardiovascular events. Furthermore, the grade of AoVC correlates with the severity and progression of aortic valve stenosis (AVS), well‑recognized in FH patients.38 Ten Kate et al39 documented increased AoVC in asymptomatic patients with heterozygous FH as compared with controls. Smith et al40 showed that genetic predisposition to high plasma LDL‑C concentration was associated with an increased risk of AoVC and further development of AVS. It was proved that elevated plasma LDL‑C and lipoprotein(a) (Lp[a]) concentrations in patients with FH may both contribute to the initiation and progression of AVS involving lipid infiltration, inflammation, fibrosis, and calcification.38,39 Several studies documented a major impact of Lp(a) on the progression of AVS, which may explain why statins and ezetimibe, lowering plasma concentration of LDL‑C but not Lp(a), have limited effect on the prevention of AVS development.38,42
Recent studies investigated the frequency and predictors of severe AVS requiring aortic valve replacement (AVR) in patients with molecularly defined FH. The SAFEHEART long‑term prospective cohort study in an FH population showed that the need for AVR due to AVS was significantly higher in FH patients, particularly in those who were older, had previous ASCVD, hypertension, and long‑term increased plasma concentration of LDL‑C Lp(a) and Lp(a).38
In summary, in FH patients a targeted management of elevated plasma Lp(a) concentration remains an important therapeutic goal. PCSK9 inhibitors and specific therapies that lower plasma Lp(a) concentration are needed to address the residual risk attributed to ASCVD and AVS in FH patients.43 Further studies are needed to evaluate the effect of specific Lp(a) lowering treatment(s) on preventing ASCVD and progression of AVS.38
Familial hypercholesterolemia and carotid artery involvement
Atherosclerosis can be visualized by carotid artery ultrasonography as the presence of intima‑media thickness (IMT) or the presence of plaques, both associated with ASCVD. Increased carotid IMT and the presence of plaques in particular may serve as predictors of ASCVD in the general population. Available studies evaluating atherosclerotic lesions in carotid arteries of FH patients are scant and only a few reports documented increased IMT in FH individuals as compared with the control groups.44
IMT was also shown as an intermediate phenotype for ASCVD risk assessment in FH patients and was used to evaluate treatment efficacy of lipid‑lowering regimens in those patients.44 Moreover, carotid IMT and the frequency of carotid plaques did not differ between the long‑term statin‑treated heterozygous FH patients and healthy controls, which may indicate that the long‑term statin treatment decreases carotid atherosclerosis to a degree of a healthy population.45 Another study reported that in statin‑treated FH patients plasma Lp(a) concentration failed to be a risk factor for ASCVD, as plasma Lp(a) levels were not associated with carotid IMT and the presence of plaques.46
Data on the incidence of carotid plaques in FH patients are conflicting, as some studies showed a higher prevalence of carotid plaques in FH patients than in controls, and other studies showed no differences in the prevalence. A recent review47 highlighted that although the obtained data indicate that FH patients are potentially at a higher risk of developing carotid atherosclerotic lesions, sufficient evidence to support a definite association is missing.
Familial hypercholesterolemia and atherosclerotic involvement of renal arteries
There are limited data on the prevalence and severity of atherosclerotic lesions in the renal arteries in FH patients. To date, only a few case reports documented atherosclerotic renal artery stenosis in such patients. Yagi et al48 demonstrated a relatively frequent involvement of atherosclerotic lesions in noncoronary vascular beds. Their study confirmed the presence of plaques in renal arteries in almost 33% of patients, and in this group renal artery stenosis was nonsignificant (<25%) in 64% of the studied individuals. However, this study included FH patients with indications for coronary angiography, which may have translated into the inclusion of patients with more severe atherosclerosis.
Familial hypercholesterolemia and abdominal aortic aneurysm
Population‑based studies confirmed an association between plasma LDL‑C and triglyceride levels and the development of abdominal aortic aneurysms. Therefore, it was postulated that FH patients might be characterized by a higher incidence of abdominal aortic aneurysms. However, as pointed out in a recent review,47 this association cannot be clearly confirmed due to a paucity of data regarding the association of FH with abdominal aortic aneurysms.
Familial hypercholesterolemia and peripheral artery disease
FH patients were shown to have a 4–10 times greater risk of developing peripheral artery disease (PAD) than the general population.47,49 Studies assessing the prevalence of PAD based on clinical symptoms (intermittent claudication) in FH patients found PAD in 8%–16% of FH patients, and those assessing PAD by means of Doppler ultrasound estimated its prevalence at 35%–40%.49 A significant variation in PAD prevalence of 17%–65% was found in the studies using the ankle‑brachial index.47
The SAFEHEART study50 showed that patients with molecularly diagnosed FH are characterized by a significantly higher prevalence of peripheral arteriosclerosis (intermittent claudication defined as a classic symptom and at least 1 positive result of the ankle‑brachial index <0.9 or stenosis >50% on angiography or ultrasonography or abdominal aortic aneurism), than their unaffected relatives (1.4% vs 0.2%, respectively).
Of note, studies performed so far confirmed a higher prevalence of PAD in FH patients with overt cardiovascular disease than in the FH patients without overt cardiovascular disease.47
Familial hypercholesterolemia and atherosclerotic cardiovascular disease
Familial hypercholesterolemia is not a rare disease, and it may affect up to 150 000 Polish patients, of whom only a small proportion achieve target LDL‑C levels, as in other countries.13 Furthermore, the FH patients constitute a part of a much larger group of individuals with severe hypercholesterolemia. It is estimated that even 1:20 individuals in the general population may present with plasma LDL‑C levels equal or above 190 mg/dl, which may translate into almost 2 million Poles characterized by very high plasma LDL‑C concentration.51
Based on the contemporary definition, FH is a common autosomal dominant disorder of lipoprotein metabolism. In consequence, severely elevated plasma levels of LDL‑C in FH individuals from birth onward substantially increase the risk for premature cardiovascular disease.
Recent large studies15 clearly documented a graded relationship between LDL‑C concentration and prevalence of CAD, the most common manifestation of ASCVD in FH patients.
The clinical picture of FH is highly variable, with a heterogeneous patient phenotype even within a single family, ranging from patients with very early onset of major cardiovascular events (eg, myocardial infarction in the third or fourth decade of life) to those who do not develop overt cardiovascular disease even at an old age.7,15 The risk of ASCVD is more pronounced in individuals 20–40 years old and the clinical course of CAD in FH is variable, as it is driven not only by elevated LDL‑C burden but also by the presence of other classic ASCVD risk factors. Research is underway to identify the factors associated with a more severe course of FH as expressed by the incidence of premature ASCVD.4,15
These findings underscore the necessity of early detection and identification of FH cases among patients with premature CAD to start cascade testing. However, available data show that the diagnosis of FH was made too late at the mean age of 44.4 years, and only 2.1% of patients were identified in childhood or adolescence.7,15 Therefore, introduction of screening strategies earlier in life may provide a more effective prevention and implementation of the statin treatment in childhood. This strategy proved efficient by bringing a reduction in ASCVD during a 20‑year follow‑up in adults who started their statin treatment in childhood, as compared with their parents who began the treatment as adults.15,52
Therefore, primary ASCVD prevention in patients with very high LDL‑C concentrations should be based on early detection, screening of family members, and effective pharmacological therapy. The assessment of the key risk modifying factors and evaluation of the presence and extent of asymptomatic atherosclerotic lesions is also important.3,15,53-55
Contrary to CAD, no graded relationship between LDL‑C and vascular diseases other than CAD was observed, indicating no similar trend for either PAD or stroke.
The association between FH and increased incidence of cerebrovascular events has not been clearly confirmed. The SAFEHART study showed no difference in the incidence of cerebrovascular disease between FH patients and unaffected relatives.50 Also, a study from Norway56 did not confirm a higher incidence of stroke in FH patients in comparison with the general population.
Another analysis49 found that the presence of an FH‑causing mutation was not associated with a higher risk of stroke, contrary to plasma LDL‑C concentration of 190 mg/dl or higher.
It was postulated that the factors likely to be associated with higher extent of atherosclerosis in patients with FH and higher ASCVD risk are not limited to classic cardiovascular risk factors, such as male sex, overlapping hypertension, diabetes, chronic kidney disease, lower high‑density lipoprotein cholesterol and higher triglyceride levels, or smoking.7,15 A few newly identified risk factors, such as plasma Lp(a) concentration or increased concentrations of inflammation markers were shown to correlate with the extent of atherosclerosis or ASCVD risk in FH patients.47,57-60
The studies discussed above pointed out that atherosclerotic involvement in the coronary arteries and lower extremities is higher in FH patients than in the general population. There is a paucity of data regarding the relationship between FH and incidence of atherosclerosis in other vascular beds (Figure 1).
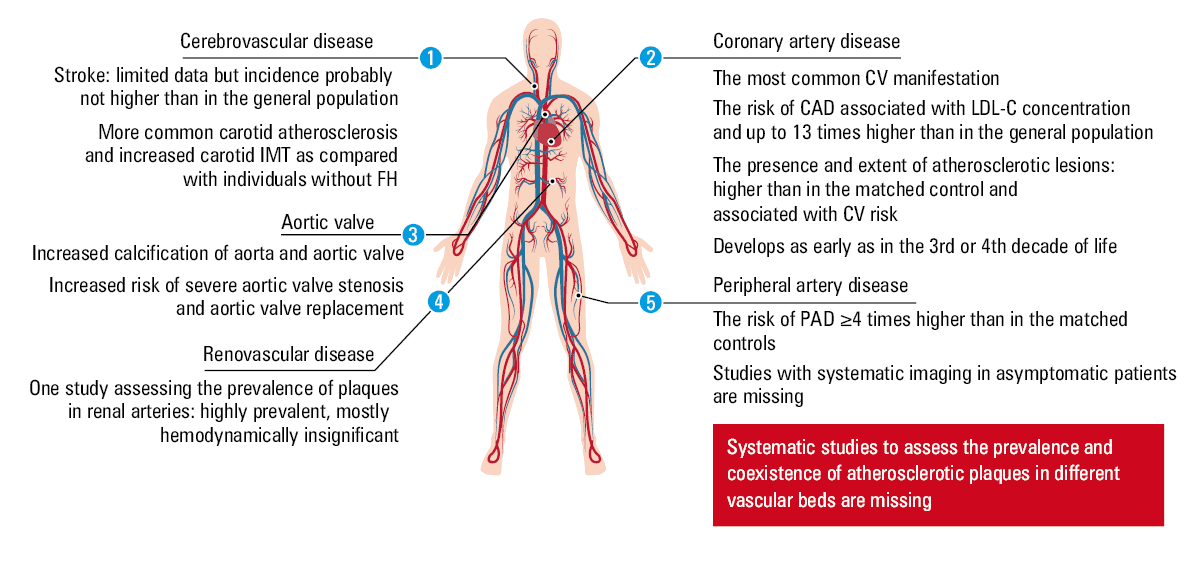
Abbreviations: CAD, coronary artery disease; CV, cardiovascular; FH, familial hypercholesterolemia; IMT, intima‑media thickness; LDL‑C, low‑density lipoprotein cholesterol; PAD, peripherial artery disease
Contrary to previous reviews47 that evaluated the prevalence of atherosclerotic changes in different vascular beds, we also showed that there are no studies systematically and simultaneously evaluating several vascular beds in asymptomatic FH patients. Such studies would broaden the current knowledge regarding the relationship between the elevated LDL‑C and the development of atherosclerosis in individual vascular beds.48,61-63
Despite recent progress in the availability of more effective LDL‑C–lowering therapies, FH remains unrecognized and undertreated.7 Moreover, there is no sufficient evidence on the effectiveness of currently recommended therapeutic strategies on atherosclerosis prognosis in various vascular beds except for coronary arteries.
Providing a systematic and in‑depth characteristic of FH patients with respect to the presence and extent of atherosclerotic lesions in different vascular beds may have important implications for daily practice not only for the FH patients but also for a larger number of people with very high plasma LDL‑C concentrations.
- Visseren FLJ, Mach F, Smulders YM, et al. 2021 ESC Guidelines on cardiovascular disease prevention in clinical practice. Eur Heart J. 2021; 42: 3227‑3337.
- Pająk A, Jankowski P, Zdrojewski T. The burden of cardiovascular disease risk factors: a current problem. Kardiol Pol. 2022; 80: 5‑15. | Crossref
- Sniderman AD, Glavinovic T, Thanassoulis G. Key questions about familial hypercholesterolemia: JACC review topic of the week. J Am Coll Cardiol. 2022; 79: 1023‑1031. | Crossref
- Hu P, Dharmayat KI, Stevens CAT, et al. Prevalence of familial hypercholesterolemia among the general population and patients with atherosclerotic cardiovascular disease: a systematic review and meta‑analysis. Circulation. 2020; 141: 1742‑1759. | Crossref
- Pajak A, Szafraniec K, Polak M, et al. Prevalence of familial hypercholesterolemia: a meta‑analysis of six large, observational, population‑based studies in Poland. Arch Med Sci. 2016; 4: 687‑696. | Crossref
ARTICLE INFORMATION