Complete unilateral duplication of the right ureter with ectopic orifice into the prostatic urethra found by transrectal ultrasound



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Complete unilateral duplication of the right ureter with ectopic orifice into the prostatic urethra found by transrectal ultrasound
A 50‑year‑old male patient was admitted to the urology department due to a stabbing pain with increasing intensity in the right lumbar region, spreading to the right groins, lasting for 3 days. Ultrasound examination revealed a duplication of the right ureter with indistinct supernumerary ureter of a tortuous course and significant widening of the right upper pelvicalyceal system. Hyperechogenic masses (suggestive of urinary deposits) were observed in the lower part of the distended ectopic ureter (megaureter). Transrectal ultrasound was performed since the orifice of the ectopic ureter was unidentifiable on transabdominal ultrasound examination. It revealed an ectopic ureter orifice in the posterior part of the prostate and stones in the distal part of the ureter (Figure 1A).
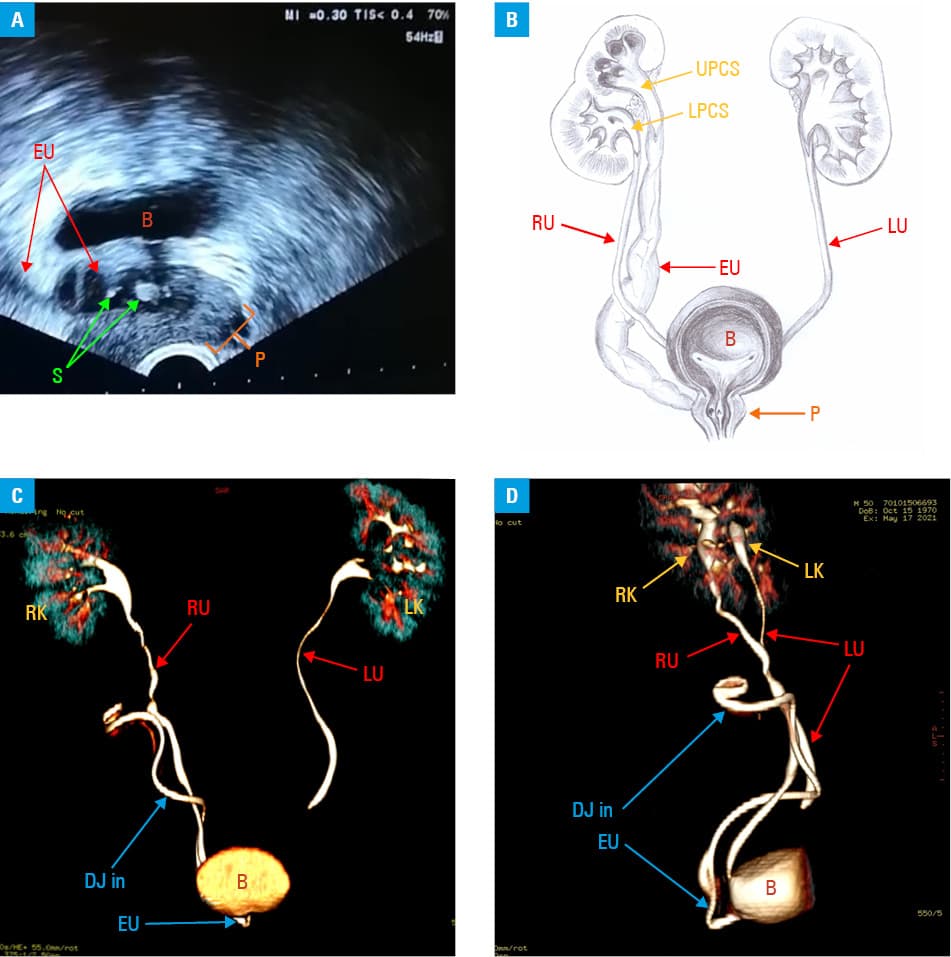
Abbreviations: B, urinary bladder; DJ, double J catheter; EU, ectopic ureter; LK, left kidney; LU, left ureter; RK, right kidney; RU, right ureter
The patient was referred for ureterorenoscopic lithotripsy (URSL). The stones were disintegrated using a holmium laser, and a double J catheter was inserted into the ectopic ureter. Computed tomography (CT) scan confirmed the anatomical anomaly: a complete duplication of the right pelvicalyceal system and ureter. The distal orifice of the ureter draining the upper pelvicalyceal system was abnormally located in the prostatic urethra, while the ureter draining the lower system entered the urinary bladder trigone on the right side (Figure 1B–1D). The upper pelvicalyceal system did not show contrast enhancement and was not visible on the CT scan (Figure 1C and 1D). For this reason, the course of the ectopic ureter was traced based on the course of the inserted double J catheter.
After the URSL procedure, the patient developed several lower urinary tract symptoms and was consequently treated for recurrent urinary tract infections. Finally, due to the anatomical anomaly, pyonephrosis developed. Therefore, laparoscopic heminephrectomy was conducted, involving the involuted upper part of the kidney with the upper pelvicalyceal system and widened ectopic ureter. During the 1‑year follow‑up, lower urinary tract symptoms receded completely.
Duplication of the ureter is a congenital abnormality of the kidney and urinary tract, with a reported frequency of 0.3% to 3.0%.1 The sex ratio is 2 to 6 women to 1 man.2 The anomaly is caused by double ureteric buds forming as 2 separate structures, each of which developing individual pelvicalyceal systems (upper and lower), ureters, and distal orifices.3 This anomaly may predispose to obstruction and megaureter formation, which may consequently cause recurrent urinary tract infections. Other potential complications include vesicoureteral reflux, urine retention leading to urolithiasis, and pyelonephritis.4 This report aimed to draw attention to the rare variant of ureter ectopy since this anomaly can cause diagnostic and surgical complications (especially during radical prostatectomy). Appropriate visualization of the ectopic ureter and its orifice out of the bladder may be challenging, leading to difficulties in imaging diagnostics and the need to apply various imaging techniques. A total of 16% of ectopic ureters cannot be detected by intravenous pyelogram due to the absence of an upper pole calyx or very thin and dysplastic renal parenchyma. Therefore, further imaging modalities, such as CT, magnetic resonance imaging, or dimercaptosuccinate scintigraphy are required.5 Careful history‑taking and physical examination remain the key diagnostic steps.
- Houat AP, Guimarães CTS, Takahashi MS, et al. Congenital anomalies of the upper urinary tract: a comprehensive review. Radiographics. 2021; 41: 462‑486. | Crossref
- Gangopadhyaya AN, Uoadhayaya VD, Panday A, et al. Single system ectopic ureter in females: a single centre study. J Indian Assoc Pediatr Surg. 2007; 4: 202‑205. | Crossref
- Arumugam S, Subbiah NK, Mariappan Senthiappan A. Double ureter: incidence, types, and its applied significance‑a cadaveric study. Cureus. 2020; 12: e7760. | Crossref
- Steyaert H, Lauron J, Merrot T, et al. Functional ectopic ureter in case of ureteric duplication in children: initial experience with laparoscopic low transperitoneal ureteroureterostomy. J Laparoendosc Adv Surg Tech A. 2009; 19 (Suppl 1): S245‑S247. | Crossref
- Hansonb GR, Gattia JM, Gittesa GK, Murphy JP. Diagnosis of ectopic ureter as a cause of urinary incontinence. J Pediatr Urol. 2007; 3: 53‑57. | Crossref
ARTICLE INFORMATION