A 56‑year‑old woman was referred to the emergency department with symptoms of drooping eyelids, double vision, and slurred, gibberish speech lasting for several hours. The patient reported consumption of stale canned food 2 days earlier. There were no abdominal symptoms. Based on the patient’s medical history and findings of the neurological examination, the initial diagnosis of foodborne botulism was established. The local Sanitary and Epidemiological Station was informed, and stool and serum samples were obtained for further epidemiological investigation. Twenty‑four hours after admission to the hospital, 50 ml of intravenous equine antitoxin (antibodies against type A, B, and E toxins) was administered but the patient’s condition worsened. Bilateral ptosis, bilateral total ophthalmoplegia (pupil diameter, 4 mm; nonresponding), drooping head, palatal paralysis, tongue muscle weakness, and symmetrical descending paresis leading to quadriparesis were observed. Neurological examination showed no weakening of sensory findings, except for persistent double vision. Due to aggravating symptoms of respiratory failure (partial pressure of carbon dioxide, 53 mm Hg), tracheal intubation was performed, and the patient was connected to a ventilator. She was referred for treatment in the Intensive Care Unit (ICU).
Peristalsis was present during the initial days of the ICU stay. The patient passed stool; therefore, the gastrointestinal tract decontamination was limited to the enema and stomach decompression via a nasogastric tube. Five days after admission to the hospital, computed tomography (CT) was performed due to elevated serum levels of inflammatory parameters (C‑reactive protein, 340.35 mg/l [reference range, 0.0–5.0 mg/l]; procalcitonin, 0.74 ng/ml [reference range, 0.0–0.5 ng/ml]). The CT scan showed dilatation of the stomach, intestines, and colon without any apparent mechanical cause, which confirmed adynamic ileus (Figure 1A). The stomach wall was thickened with the presence of intramural gas (Figure 1B). The pneumatosis was also observed in the duodenum and proximal part of the jejunum (Figure 1C). Based on CT imaging, upper gastrointestinal tract ischemia and necrosis were suspected. Moreover, portal venous gas was visualized, which is associated with the risk of sepsis and a high mortality rate (Figure 1D).
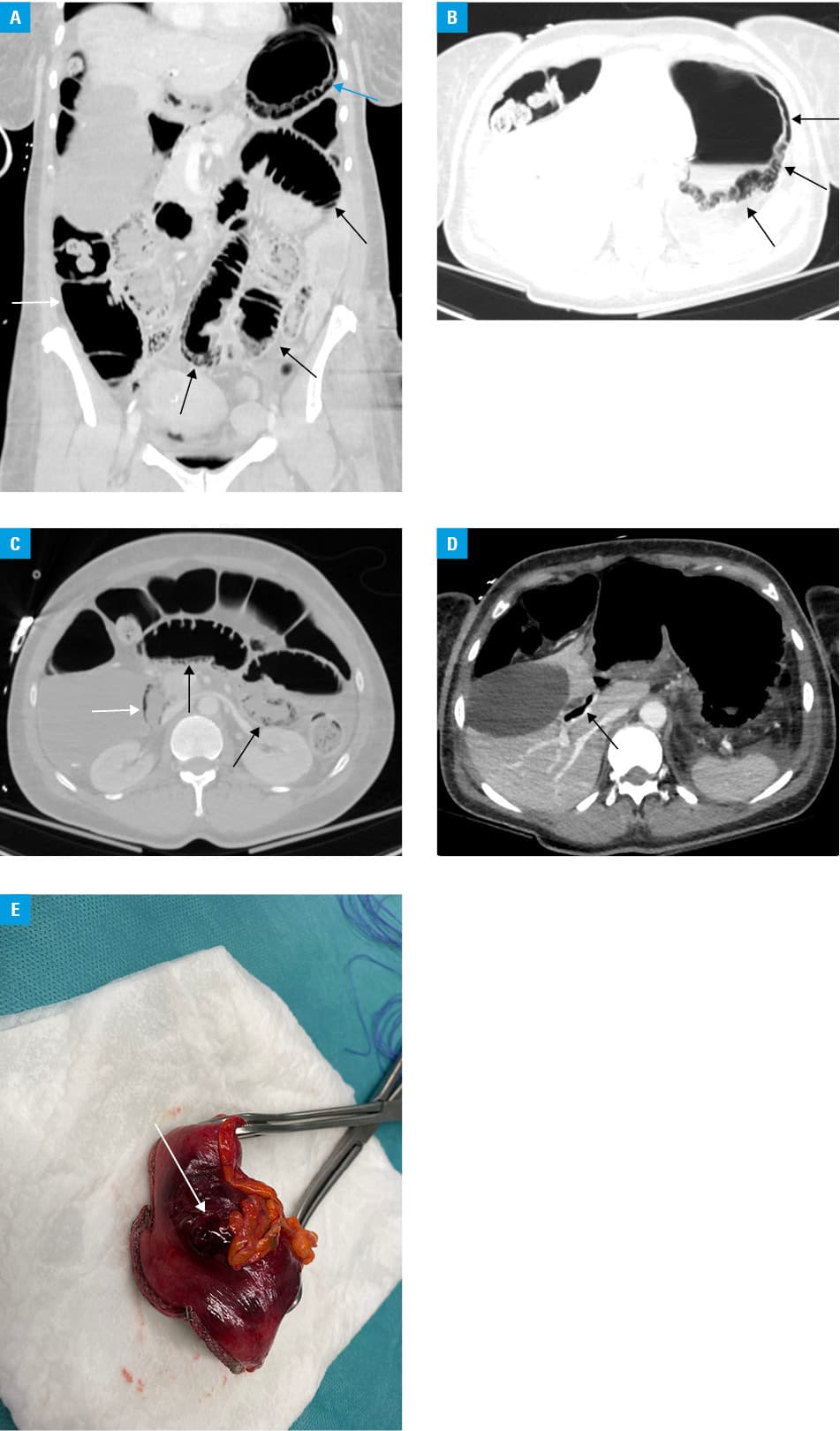
The patient was referred for emergency laparotomy. During the exploratory procedure, the fundus of the stomach was resected because of necrosis (Figure 1E). The first loop of the jejunum was ischemic but without full‑thickness necrosis of the wall; therefore, a second‑look laparotomy was scheduled to inspect the jejunum. The procedure was conducted on the following day; 20 cm of the jejunum distal to the ligament of Treitz was resected and primary side‑to‑side anastomosis was performed. The final histopathological report revealed necrosis of the mucosa and submucosa in both the stomach and jejunum specimens. At the time of the article submission, the patient has been hospitalized in the ICU for 45 days; however, there has been no need for mechanical ventilation. We have not observed significant complications following the surgical interventions.
Botulism is a very rare condition caused by botulinum neurotoxin, which is elaborated by vegetative forms of Clostridium botulinum. Typical symptoms of botulism are caused by inhibition of acetylcholine release at the neuromuscular junction, resulting in flaccid paralysis. The clinical presentation is highly distinctive, with symmetrical cranial nerve palsies.1 In more severe cases, symmetrical descending flaccid paralysis with respiratory failure is present.2 Foodborne botulism is rare, with a median number of 23 cases per year in the United States between 1990 and 2000.3 The annual incidence rate in Poland is 0.02 per 100 000 inhabitants (data as of 2021). The differential diagnosis of botulism includes the Miller–Fisher syndrome (variant of the Guillain–Barré syndrome), stroke, myasthenia gravis, tetrodotoxin poisoning, and the Lambert–Eaton myasthenic syndrome.
A study on the animal model conducted by Dack et al4 confirmed that exposure to botulinum toxin can cause necrosis of the stomach wall. A case reported by Nimeri et al5 indicates that there is a risk of stomach necrosis due to direct injection of botulinum toxin for the treatment of obesity. To the best of our knowledge, this is the first description of necrosis of the stomach and jejunum caused by severe foodborne botulism. Nevertheless, the possibility of such a diagnosis should not be disregarded in patients presenting with acute gastrointestinal complaints associated with even mild neurological symptoms.
- Starin WA, Dack GM. Pathogenicity of clostridium botulinum. J Infect Dis. 1925; 36: 383‑412. | Crossref
- Sobel J. Botulism. Clin Infect Dis. 2005; 41: 1167‑1173. | Crossref
- Sobel J, Tucker N, Sulka A, et al. Foodborne botulism in the United States, 1990–2000. Emerg Infect Dis. 2004; 10: 1606‑1611. | Crossref
- Dack GM, Gibbard J. Studies on botulinum toxin in the alimentary tract of hogs, rabbits, guinea‑pigs and mice. J Infect Dis. 1926; 39: 173‑180. | Crossref
- Nimeri A, Zaman MB, Maasher A, et al. Endoscopic intra‑gastric botulinum toxin injection for obesity leading to total gastrectomy and Roux en Y esophago‑jejunostomy. Surg Obes Relat Dis. 2016; 12: 116. | Crossref
ARTICLE INFORMATION