Obscure-overt gastrointestinal bleeding: a review
Key words: colonoscopy, endoscopy, enteroscopy, obscure overt gastrointestinal bleeding, video capsule endoscopy



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Obscure-overt gastrointestinal bleeding: a review
Obscure gastrointestinal (GI) bleeding (OGIB) is defined as small bowel bleeding of unknown etiology after negative endoscopic evaluation including esophagogastroduodenoscopy and colonoscopy with endoscopic evaluation of the terminal ileum. The presentation of OGIB may be either overt or occult. The former refers to persistent or recurrent visible GI bleeding (eg, melena and / or hematochezia, and rarely hematemesis), while the latter indicates the presence of persistently positive results of fecal occult blood testing, iron deficiency anemia, or both, without evidence of visible GI bleeding. This review focuses exclusively on obscure‑overt GI bleeding and presents entities that should be considered as part of the differential diagnosis in patients with this type of bleeding, as well as details the role of endoscopic and radiographic techniques in the evaluation and treatment.
Introduction
Gastrointestinal (GI) bleeding may originate anywhere from the mouth to the rectum or anus. Overt clinical manifestations of GI bleeding include hematemesis, melena, and / or hematochezia. Approximately 50% of the GI bleeding episodes originate in the upper GI tract (esophagus, stomach, and / or duodenum—proximal to the ligament of Treitz), 40% are from the lower GI tract (colon and rectum), and 10% are from the small bowel. Small bowel bleeding is defined as a bleeding that starts anywhere between the ligament of Treitz and the ileocecal valve.1,2
Obscure GI bleeding (OGIB) is defined as small bowel bleeding of unknown etiology after negative endoscopic evaluation including esophagogastroduodenoscopy (EGD) and colonoscopy with endoscopic evaluation of the terminal ileum. The presentation of OGIB may be either overt or occult. Obscure‑overt GI bleeding refers to persistent or recurrent visible GI bleeding (eg, melena and / or hematochezia, and rarely hematemesis), while obscure‑occult GI bleeding is characterized by persistently positive results of fecal occult blood tests, iron deficiency anemia, or both, without evidence of visible GI bleeding. This review focuses exclusively on the overt presentation of OGIB.
Causes of obscure‑overt gastrointestinal bleeding
The etiologies of upper and lower GI bleeding can be diagnosed and treated by EGD and colonoscopy, respectively. The differential diagnosis of upper GI bleeding most commonly includes peptic ulcer, esophageal and gastric varices, Mallory–Weiss tear, and Dieulafoy lesions, while lower GI bleeding is most commonly due to diverticulosis, hemorrhoids, angioectasia, colitis, and neoplasms.3,4
The differential diagnosis of OGIB can be stratified based on the patient’s age. For example, in patients younger than 40 years, OGIB is more likely to be due to malignancy (eg, lymphoma), polyposis syndromes, Meckel’s diverticulum, inflammatory bowel disease, or Dieulafoy lesions.1 In older patients (≥40 years), OGIB is more often caused by angioectasias or a nonsteroidal anti‑inflammatory drug (NSAID)-induced ulcer. The most common causes of OGIB are summarized in Table 1 and described in more detail below.
Rare causes | Common causes | |
≥40 years of age | <40 years of age | |
Abbreviations: FAP, familial adenomatous polyposis; NSAID, nonsteroidal anti‑inflammatory drug | ||
Henoch–Schoenlein purpura | Angioectasia | Inflammatory bowel disease |
Amyloidosis | Dieulafoy lesions | Dieulafoy lesions |
Aorto‑enteric fistula | Neoplasia | Neoplasia |
Hemosuccus entericus | NSAID‑induced ulcers | Meckel’s diverticulum |
Osler–Weber–Rendu disease | ||
Kaposi sarcoma with HIV | ||
Blue rubber bleb nevus syndrome | ||
Plummer–Vinson syndrome | ||
Inherited polyposis syndromes (FAP, Peutz–Jeghers syndrome) | ||
Small bowel varices and / or portal hypertensive enteropathy | ||
Hematobilia | ||
Angioectasia
Angioectasia is the formation of aberrant blood vessels found throughout the GI tract that can develop in advanced age or as a consequence of related comorbidities (eg, chronic renal disease, cirrhosis, rheumatologic disorders, and severe cardiovascular disease). These lesions can cause overt or occult GI bleeding in adults, particularly in the elderly, especially in those treated with antiplatelet agents and / or anticoagulants.
Angioectasias may involve any segment of the GI tract, and the lesions are usually multiple in any given segment of the intestine. On endoscopy, angioctasia appears as a 2- to 10‑mm erythematous lesion, with arborizing ectatic blood vessels that emanate from a central vein (Figure 1).

Meckel’s diverticulum
Meckel’s diverticulum is a congenital, blind intestinal pouch that is usually located in the distal ileum. It is characterized by “the rule of 2s”: it occurs in 2% of the population, is found within 2 feet of the ileocecal valve, is 2 inches long in size, results in complications in 2% of cases, consists of 2 types of ectopic tissue (gastric or pancreatic), usually presents clinically at the age of 2 years, and has a male‑to‑female ratio of more than 2:1. The most common complications of Meckel’s diverticulum are bleeding, bowel obstruction, and diverticulitis. The most widely used diagnostic test for this anomaly is 99m technetium pertechnetate scintigraphy; however, its sensitivity is between 75% and 100% with bleeding. Cross‑sectional imaging (computed tomography [CT] and magnetic resonance imaging) may also be of diagnostic value. Additionally, video capsule endoscopy (VCE) may aid in the diagnosis.4
Nonsteroidal anti‑inflammatory drug–induced small intestinal erosions and ulcers
Erosions and ulcers can develop in 25% to 55% of patients who take high doses of nonselective NSAIDs. Patients treated with selective cyclooxygenase (COX)-2 inhibitors have lower rates of small bowel mucosal ulcers.5
Small intestinal neoplasms
The most common small intestinal neoplasms are benign adenomas (usually duodenal), adenocarcinomas, carcinoid tumors, GI stromal tumors, lymphomas, hamartomas, and juvenile polyps.
Dieulafoy lesion
This type of lesion is most commonly found in the stomach; however, it can also present in any part of the GI tract. In younger individuals it is usually localized in the small intestine (duodenum, jejunum, and ileum), whereas in older persons it is more often found in the stomach.5
Rare etiologies
Although the abovementioned conditions are the most common causes of GI bleeding found in the majority of OGIB cases, there are a few rare etiologies that may also lead to OGIB. Among these rare causes are hereditary hemorrhagic telangiectasia, blue rubber bleb nevus syndrome, hereditary polyposis syndromes (familial adenomatous polyposis, Peutz–Jeghers syndrome), small bowel varices and / or aorto‑enteric fistula, and several others that are beyond the scope of this review (Table 1).
Diagnosis of obscure gastrointestinal bleeding
The approach to further evaluation of patients with OGIB depends on several factors: whether the bleeding is occult or overt, whether the patient has signs of severe ongoing bleeding, and whether comorbidities allow for additional endoscopic evaluations. Ohmiya et al6 reported an association between the stool color and the anatomical location of OGIB. The authors reported that tarry stools were mostly associated with bleeding from the upper GI, jejunal, or proximal ileal site, whereas bright or dark red stool were often observed in cases of distal ileal or colorectal bleeding.6
The flowchart of the diagnostic workup of OGIB is presented in Figure 2. The tools used in the diagnosis are described below.
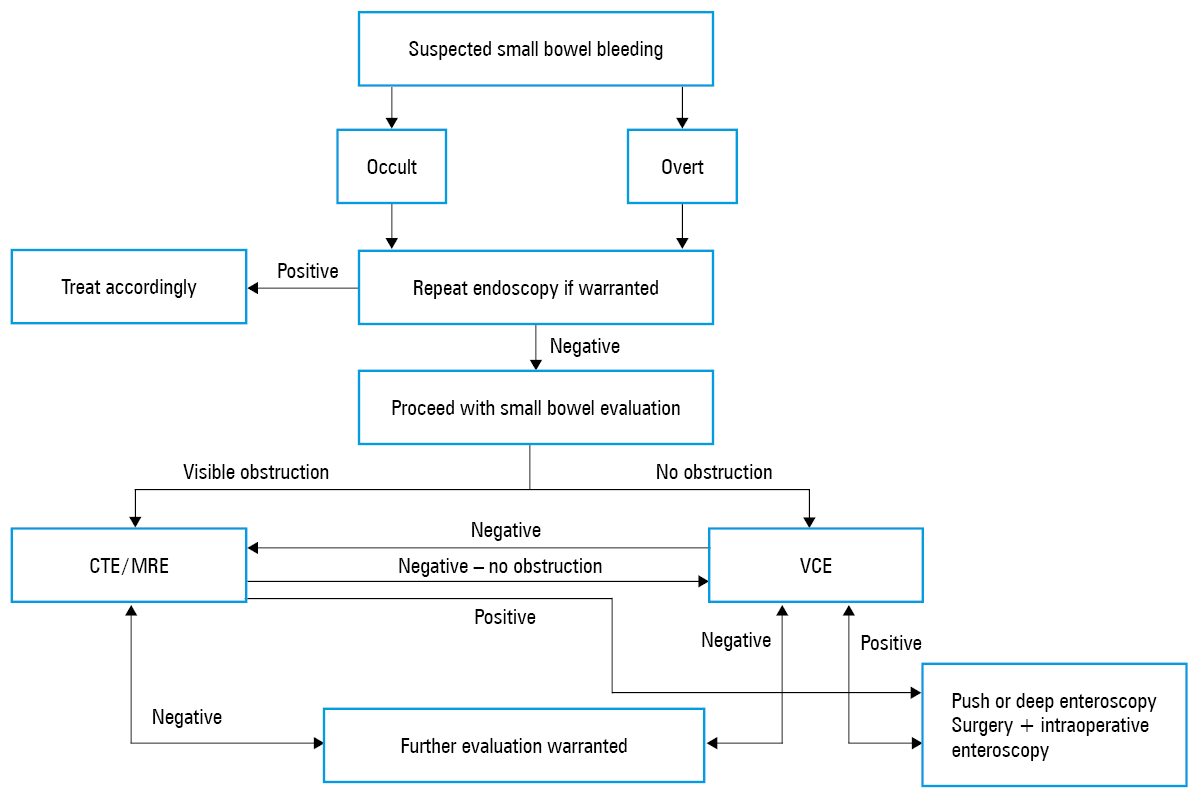
Abbreviations: CTE, computed tomography enterography; MRE, magnetic resonance enterography; VCE, video capsule endoscopy
“Second‑look” endoscopy in the diagnosis of obscure gastrointestinal bleeding
Studies reported that a high percentage of patients who were initially thought to have small bowel bleeding were subsequently found to be bleeding from a site that was missed even though it could have been identified during conventional EGD and / or colonoscopy.1,2
Accordingly, current evidence‑based guidelines recommend a “second‑look” EGD in cases of recurrent hematemesis, melena, or a previously incomplete endoscopy examination of the upper GI tract. Moreover, a “second‑look” colonoscopy is recommended in the setting of recurrent hematochezia, in the cases when prior colonoscopy was incomplete due to inadequate preparation, or if terminal ileoscopy was not performed.1,2,7
Next recommended step in the evaluation of obscure gastrointestinal bleeding
The 2007 American Gastroenterology Association guidelines recommended that patients with documented overt GI bleeding (excluding hematemesis) and negative findings on high‑quality EGD and colonoscopy undergo VCE of the small bowel as the next step in the diagnostic evaluation.
A randomized trial by Laine et al8 showed that the diagnostic yield of VCE as compared with dedicated radiological evaluation of the small bowel for suspected bleeding was 30% vs 7%, respectively. Moreover, Leung et al,9 who evaluated small bowel VCE vs angiography, showed that the diagnostic yield of VCE was higher than that of angiography in patients with overt small bowel bleeding (53.3% vs 20.0%, respectively; P = 0.016).9 Finally, in another randomized controlled trial comparing the outcomes of VCE and push enteroscopy in patients with OGIB, Segarajasingam et al10 showed that first‑approach VCE had a significant diagnostic advantage over push enteroscopy, with a significantly higher diagnostic yield (72.5% vs 48.7%, respectively; P <0.05). Similarly, the American College of Gastroenterology (ACG) and the European Society of Gastrointestinal Endoscopy recommend VCE as the next diagnostic procedure for evaluating suspected small bowel bleeding after exclusion of the upper and lower GI tracts as the sources of bleeding.1,2 They also recommend that, owing to the lower detection rate of lesions localized in the duodenum and proximal jejunum with VCE, push enteroscopy may be performed when a proximal bleeding site is suspected.
Push enteroscopy
Following negative results of EGD and colonoscopy, push enteroscopy can be performed for the evaluation of the proximal small bowel. It enables the assessment of the upper GI tract up to approximately 100 cm distal to the ligament of Treitz. Push enteroscopy allows for appropriate diagnostic and therapeutic interventions and can be performed using either a dedicated enteroscope or a pediatric colonoscope.
Video capsule endoscopy
VCE is performed using a small camera placed within a capsule that the patient ingests with a small amount of water while a belt sensor and a recording device are attached to the patient’s abdomen to transmit the images captured by the capsule. The video capsule travels through the entire small bowel until it reaches the colon and is later naturally expelled. VCE can identify active bleeding or signs of recent bleeding, angiodysplasia, mucosal inflammation (eg, erosions, ulcerations), and neoplasms. It is a diagnostic tool for evaluating obscure‑overt GI bleeding in the case when there is no suspected small bowel obstruction. If the site of small bowel bleeding is identified during VCE, targeted management should be initiated (device‑assisted deep enteroscopy, intraoperative enteroscopy, or surgery). European and American guidelines both recommend that for the evaluation of obscure‑overt GI bleeding, VCE should be performed as soon as possible after the bleeding episode, optimally within 14 days, to maximize the diagnostic yield.1,2,7 With the development of VCE more than 2 decades ago, endoscopic examination of the entire small bowel has become feasible and can guide the therapeutic intervention.
When VCE is unrevealing and the patient has ongoing bleeding, a repeat endoscopy (EGD and / or colonoscopy) should be considered, along with a repeat VCE and / or tagged red blood cell (RBC) scan, intraoperative enteroscopy, or surgery.
Device‑assisted enteroscopy
Device‑assisted enteroscopy, also referred to as deep enteroscopy, has significantly advanced in recent years and can be performed using different types of enteroscopes. The first reported device‑assisted deep enteroscopy used the double‑balloon technique (double‑balloon enteroscopy [DBE]), which was invented and reported by Yamamoto et al11 in 2001. It involved a dedicated enteroscope using 2 balloons, one attached to the distal tip of the enteroscope and the other to the distal end of a flexible overtube. Both balloons allow for anchoring of the small bowel wall and advancing the enteroscope through the small bowel. The DBE can be used anterogradely (through the mouth) or retrogradely (through the rectum). With the dedicated deep enteroscopes, diagnosis and therapeutic interventions are feasible. Although uncommon, potential adverse events associated with DBE include bowel perforation, pancreatitis, bleeding, and aspiration pneumonia.
Other device‑assisted enteroscopy techniques include single balloon enteroscopy and spiral enteroscopy. The former is similar to DBE but was reported to have a lower diagnostic yield. A novel power spiral enteroscopy is a new technique using a foot‑switch–operated motor that rotates an overtube equipped with spiral‑shaped fins positioned on the enteroscope. The rotation of the spiral fins supports continuous pleating or folding of the small intestine over the enteroscope with a goal of improving the range of maneuverability and shortening procedure times.
Radiographic techniques used in the diagnosis of obscure‑overt gastrointestinal bleeding
Several studies reported conflicting results regarding the yield of CT enterography (CTE) and VCE in evaluating obscure‑overt GI bleeding.1,2 The advantage of CTE over VCE is the improved detection of small bowel masses, especially those that are mural‑based. Therefore, CTE and VCE may be complementary examinations in the evaluation of OGIB. Accordingly, the ACG recommends CTE in patients with suspected small bowel bleeding and negative VCE results because of a higher sensitivity for the detection of mural‑based small bowel masses and the ability to guide subsequent deep enteroscopy.1 Moreover, CTE can be considered before VCE in the setting of an established inflammatory bowel disease, a history of radiation therapy, previous small bowel surgery, and / or suspected small bowel stenosis. Magnetic resonance enterography was evaluated in only a few studies and was compared with VCE in patients with OGIB. In that study, VCE was shown to have a significantly higher diagnostic yield (P = 0.0015).12
Tagged red blood cell scintigraphy
This modality involves the injection of intravenous radiolabeled RBCs prior to serial scintigraphy. Scintigraphy can detect bleeding at bleeding rates as low as 0.04 ml/min, and the radiolabeled RBCs remain in the circulation for up to 24 hours, so follow‑up serial scans can be obtained. However, the RBC scintigraphy has a reported wide range of sensitivity (30%–90%) and specificity (30%–90%), and its diagnostic yield ranges between 25% and 85%; thus, its accuracy in the evaluation of obscure‑overt GI bleeding is limited.
Meckel’s scan
This diagnostic test is performed in the nuclear medicine department. It involves intravenous administration of 99m technetium pertechnetate to detect ectopic gastric mucosa in the Meckel’s diverticulum.
Angiography
CT angiography can identify the site of bleeding when the rate of arterial bleeding is at least 0.5 ml/min. The sensitivity of angiography ranges between 30% and 50%, with higher sensitivity rates for active GI bleeding than for recurrent acute or chronic occult bleeding. This modality offers the greatest benefit if active arterial bleeding is detected. In such cases, embolization can be performed to control the bleeding lesion. Potential adverse events associated with embolization include bowel ischemia, hematoma formation, femoral artery thrombosis, hypersensitivity to contrast dye, acute kidney injury, and transient ischemic attack.
Intraoperative enteroscopy
With the advent and routine use of advanced endoscopic techniques, including VCE and device‑assisted deep enteroscopy, the diagnosis and management of overt OGIB have become more accurate. Today, intraoperative enteroscopy is largely reserved for patients with negative extensive evaluation and with ongoing overt‑obscure GI bleeding and a continuing need for blood transfusions.
- Gerson LB, Fidler JL, Cave DR, Leighton JA. ACG clinical guideline: diagnosis and management of small bowel bleeding. Am J Gastroenterol. 2015; 110: 1265. | Crossref
- Pennazio M, Spada C, Eliakim R, et al. Small‑bowel capsule endoscopy and device‑assisted enteroscopy for diagnosis and treatment of small‑bowel disorders: European Society of Gastrointestinal Endoscopy (ESGE) Clinical Guideline. Endoscopy. 2015; 47: 352. | Crossref
- Gralnek IM, Stanley AJ, Morris AJ, et al. Endoscopic diagnosis and management of nonvariceal upper gastrointestinal hemorrhage (NVUGIH): European Society of Gastrointestinal Endoscopy (ESGE) Guideline – update 2021. Endoscopy. 2021; 53: 300‑332. | Crossref
- Triantafyllou K, Gkolfakis P, Gralnek IM, et al. Diagnosis and management of acute lower gastrointestinal bleeding: European Society of Gastrointestinal Endoscopy (ESGE) Guideline. Endoscopy. 2021; 53: 850‑868. | Crossref
- Tomonori Y, Yamamoto H, Sunada K, et al. Endoscopic classification of vascular lesions of the small intestine (with videos). Gastrointest Endosc. 2008; 67: 169‑172. | Crossref
ARTICLE INFORMATION