Myocardial injury is a common finding among patients hospitalized for COVID‑19, and it is associated with a poor prognosis.1 Takotsubo syndrome (TTS) is a serious cardiac condition, indistinguishable from acute myocardial infarction at initial presentation.2 Viral infections are reportedly a less frequent cause of TTS than bacterial sepsis,3,4 and we report a case of TTS triggered by SARS‑CoV‑2 infection.
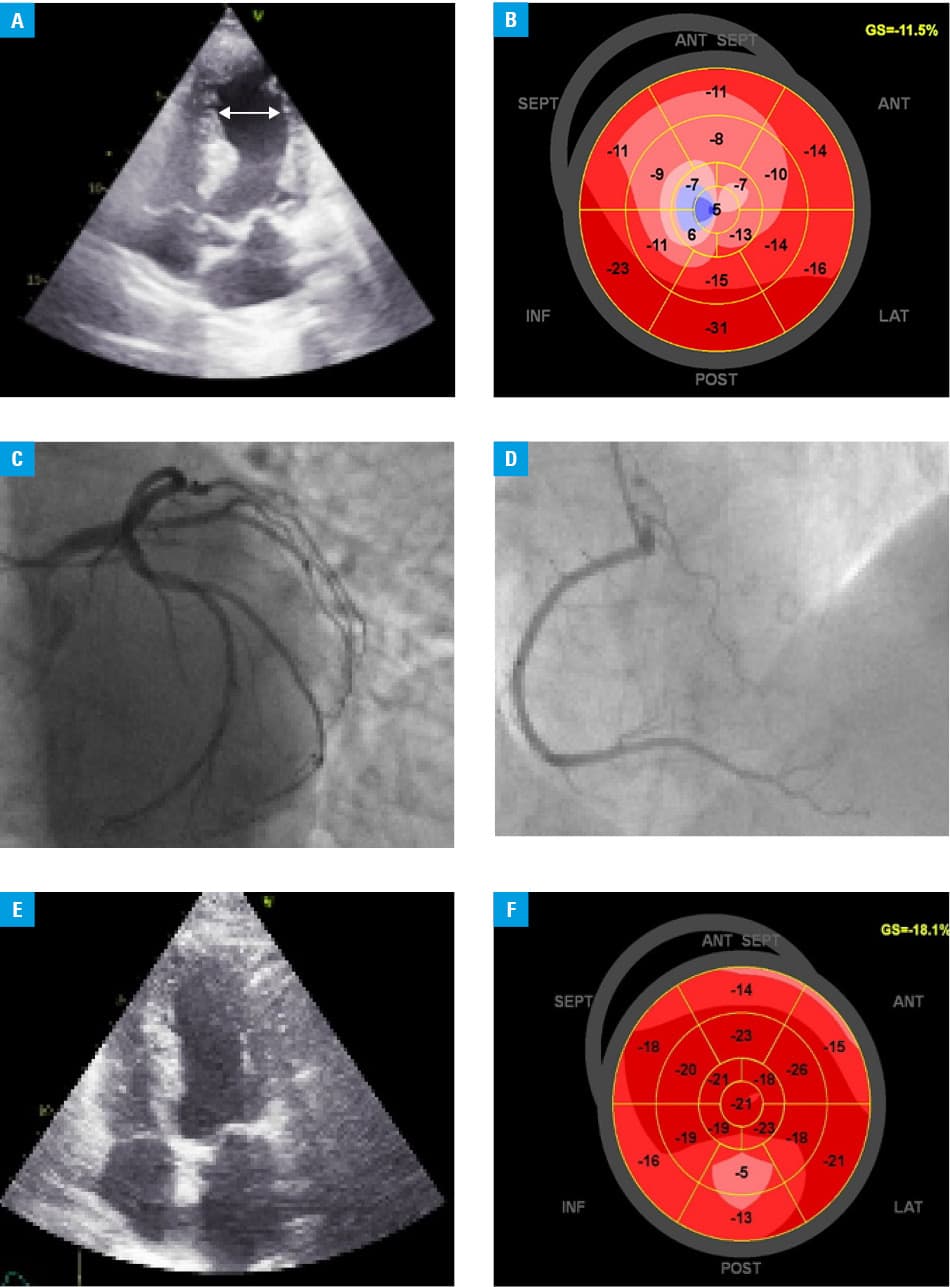
A 76‑year‑old woman with a history of arterial hypertension, asthma, and deep vein thrombosis was admitted to the isolation ward due to a mild fever, dry cough, exercise dyspnea, stomach pains, and vomiting persisting for 2 weeks. The patient had neither chest pain nor a history of coronary disease or heart failure. The PCR test from a nasopharyngeal swab sample confirmed COVID‑19, which was consistent with chest computed tomography showing multiple peripheral, small areas of ground‑glass opacities. Laboratory tests showed leukopenia (2000 cells/µl; reference range, 4000–10 000 cells/µl), significantly elevated N‑terminal pro–B‑type natriuretic peptide level (3202 pg/ml; reference range 0–125 pg/ml), normal C‑reactive protein (CRP) and D‑dimer. On the admission day, troponin T increased from 47 ng/l to 249 ng/l within a few hours (normal <14 ng/l). Electrocardiogram (ECG) revealed sinus rhythm of 80 bpm, left anterior fascicular block, and ST segment depression in V1–V5 leads. Due to those findings the patient was transferred to the Cardiology Department in a stable condition of mild shortness of breath, heart rate of 60 bpm, and blood pressure of 134/76 mm Hg. As the oxygen saturation was 95%, supplemental oxygen was not required. Both CRP (65 mg/l, normal <5 mg/l) and interleukin‑6 were elevated (131 pg/ml, nornal <7.0 pg/ml), high‑sensitivity cardiac troponin T and creatine kinase MB tests were normal in repeated measurements. The ECG showed sinus rhythm of 60 bpm with negative T waves in II, III, aVF, V1–V6 leads. Echocardiogram revealed apical dyskinesis resulting in apical ballooning and hypo‑akinesia of the mid‑ventricular segments with severely reduced left ventricular ejection fraction (LVEF) of 30% (Figure 1A and 1B). Angiography revealed only mild, nonobstructive atherosclerotic plaques in the coronary arteries (Figure 1C and 1D). During 9 days of hospitalization the patient was treated with steroids, ceftriaxone, and a therapeutic dose of enoxaparin. Control echocardiogram performed after 2 months revealed the resolution of apical ballooning and improvement of LVEF to 58% (Figure 1E and 1F), consistent with a diagnosis of COVID‑related TTS, based upon typical finding of apical ballooning in the absence of coronary disease and spontaneous functional recovery, although myocarditis remains a potential differential diagnosis.
Takotsubo syndrome occurs most commonly in women (about 90% of cases) and is usually preceded by emotional or physical triggers. It is estimated that 19.7% of COVID‑19 patients have associated cardiac complications but TTS remains a rare variety.5 It may be hypothesized that COVID‑19 produces a strong stress‑induced adrenergic discharge due to fever, inflammatory response to infection, and the need for hospitalization enhanced by hypoxia and dyspnea.
- Giustino G, Croft LB, Stefanini GG, Bragato R, et al. Characterization of myocardial injury in patients with COVID‑19. J Am Coll Cardiol. 2020; 76: 2043‑2055.
- Jaguszewski M, Osipova J, Ghadri JR, et al. A signature of circulating microRNAs differentiates takotsubo cardiomyopathy from acute myocardial infarction. Eur Heart J. 2014; 35: 999‑1006. | Crossref
- Cappelletti S, Ciallella C, Aromatario M, et al. Takotsubo cardiomyopathy and sepsis. Angiology. 2017; 68: 288‑303. | Crossref
- Meyer P, Degrauwe S, Van Delden C, et al. Typical takotsubo syndrome triggered by SARS‑CoV‑2 infection. Eur Heart J. 2020; 41: 1860. | Crossref
- Shi S, Qin M, Shen B, et al. Association of cardiac injury with mortality in hospitalized patients with COVID‑19 in Wuhan, China. JAMA Cardiol. 2020; 5: 802‑810. | Crossref
ARTICLE INFORMATION