Cardiac biomarkers on admission and in‑hospital mortality in COVID-19 patients with or without concomitant heart failure
Key words: heart failure, high-sensitivity cardiac troponin T, myocardial injury, N-terminal pro–B-type natriuretic peptide, SARS-CoV-2



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Cardiac biomarkers on admission and in‑hospital mortality in COVID-19 patients with or without concomitant heart failure
Introduction: High‑sensitivity cardiac troponin T (hs‑cTnT) and N‑terminal pro–B‑type natriuretic peptide (NT‑proBNP) are known markers of cardiac injury. However, their role in predicting the severity of COVID‑19 remains to be investigated.
Objectives: We aimed to analyze the association between hs‑cTnT and NT‑proBNP levels and in‑hospital mortality in patients with COVID‑19, with emphasis on those with concomitant chronic heart failure (CHF).
Patients and methods: A total of 1729 consecutive patients with COVID‑19 were enrolled. Demographic data, laboratory parameters, and clinical outcomes (discharge or death) were analyzed. Receiver operating characteristic (ROC) and logistic regression analyses were performed to evaluate the association between hs‑cTnT and NT‑proBNP values and the risk of death.
Results: Evaluation of hs‑cTnT was performed in 1041 patients, while NT‑proBNP was assessed in 715 individuals. CHF was present in 179 cases (10.4% of the cohort). Median values of hs‑cTnT and NT‑proBNP and in‑hospital mortality were higher in CHF patients than in those without CHF. Among patients without CHF, mortality was the highest in those with hs‑cTnT or NT‑proBNP values in the fourth quartile. In ROC analysis, hs‑cTnT equal to or above 142 ng/l and NT‑proBNP equal to or above 969 pg/ml predicted in‑hospital death. In patients without CHF, each 10‑ng/l increase in hs‑cTnT or 100‑pg/ml increase in NT‑proBNP was associated with a higher risk of death (odds ratio [OR], 1.01 and OR, 1.02, respectively; P <0.01 for both).
Conclusions: The level of hs‑cTnT or NT‑proBNP predicts in‑hospital mortality in COVID‑19 patients. Both hs‑cTnT and NT‑proBNP should be routinely measured on admission in all patients hospitalized due to COVID‑19 for early detection of individuals with an increased risk of in‑hospital death, even if they do not have concomitant heart failure.
What's new?
The study presents results based on a large database of consecutive patients with COVID‑19 treated in a single hospital according to the same standard. It shows that patients with pre‑existing heart failure and COVID‑19 had a particularly high risk of in‑hospital death. However, abnormal values of high‑sensitivity cardiac troponin T and N‑terminal pro–B‑type natriuretic peptide (NT‑proBNP) measured on admission allowed us to identify patients with a higher risk of death and prolonged hospitalization, regardless of whether they had heart failure or not. Thus, the study postulates that the markers of cardiac injury should be routinely measured on admission in all patients with COVID‑19, not only in those with a history of cardiovascular disease. The results add to the growing evidence that simple‑to‑obtain cardiac biomarkers, such as cardiac troponin and NT‑proBNP, may help in early risk stratification of patients hospitalized for SARS‑CoV‑2 infection.
Introduction
Although COVID‑19 is a viral disease in which the lungs are the primary and most severely affected organ, in some cases, it can also involve other organs, especially the heart and peripheral vessels. After the early infection stage, a severe hyperinflammation may occur, from which systemic complications are likely to result. The severity of COVID‑19 depends on many factors, the most important being age and pre‑existing comorbidities.1-4 SARS‑CoV‑2 can also affect the cardiovascular system in a variety of ways. In patients without a prior history of cardiovascular disease, it is likely that the extent of systemic inflammatory response is of vital importance. In individuals with a history of pre‑existing cardiovascular disease or comorbidities, these conditions become apparent or more complicated during COVID‑19, both as a consequence of inflammation and due to the side effects of medication or secondary hospital‑acquired infections or complications.5-7 Most patients infected with SARS‑CoV‑2 report to the hospital after the viremia phase, when they develop more severe symptoms of the disease: fever, weakness, dyspnea, and hypoxemia. This means that they are at least in the pulmonary phase of the disease, which can be confirmed by lung imaging. At this early stage of hospitalization, it is extremely important to identify the patients who are at an increased risk of death.
For many years, cardiac biomarkers are have been used in clinical practice to identify and assess the progression of cardiovascular diseases. Among these biomarkers, high‑sensitivity cardiac troponin (hs‑cTn) and N‑terminal pro–B‑type natriuretic peptide (NT‑proBNP) are the most frequently used. They are important in various cardiovascular conditions, such as chronic heart failure (CHF), ischemic heart diseases, acute coronary syndromes, or pulmonary embolism. Hs‑cTn, as a marker of cardiomyocyte necrosis, and NT‑proBNP, as a marker of cardiac biomechanical stress, seem to be useful for early stratification of patients hospitalized for COVID‑19—both are associated with damage of the heart, and therefore, their concentration during COVID‑19 indicates involvement of the cardiovascular system.5,8-10
Although several studies have shown that elevated levels of hs‑cTn or NT‑proBNP are associated with a higher risk of complications and death in patients with COVID‑19,11-14 some aspects remain to be clarified, especially with respect to individuals with concomitant heart failure. For example, it is unclear whether troponin and / or NT‑proBNP are more useful in terms of risk stratification and mortality prediction than classic inflammatory parameters, such as leukocyte count, C‑reactive protein (CRP), or interleukin 6 (IL‑6). Thus, the aim of this study was to investigate the association between high‑sensitivity troponin T (hs‑cTnT) and NT‑proBNP values on admission to the hospital and in‑hospital mortality in a large cohort of patients with COVID‑19, with particular emphasis on individuals with a prior history of CHF.
Patients and methods
We analyzed medical records of all consecutive patients who were admitted between March 6, 2020 and October 15, 2020 to the University Hospital in Kraków, Poland, which was temporarily converted into an Infectious Disease Hospital designated for the treatment of patients with COVID‑19. The patients were diagnosed with COVID‑19 according to the World Health Organization and Polish guidelines using reverse transcription–polymerase chain reaction (rhino‑oropharyngeal swab positive for SARS‑CoV‑2 RNA).15 The protocol used for COVID‑19 treatment was in accordance with recommendations of the Polish Association of Epidemiologists and Infectiologists.16,17 The patient data were obtained from the electronic Hospital Information System. Cardiovascular risk factors and diseases were identified based on the medical history and / or prior treatment, and were defined according to the current European Society of Cardiology guidelines.18 Information on the demographics, symptoms, laboratory tests (hs‑cTnT measured with the enzyme‑linked immuno‑culture assay [ELICA] using a Cobas Pro device [Roche Diagnostics GmbH, Mannheim, Germany]; NT‑proBNP measured with ELICA using a Cobas Pro device [Roche Diagnostics]; high‑sensitivity CRP (hs‑CRP) measured by nephelometry using a Siemens BN II device [Siemens Healthineers, Erlangen, Germany]; interleukin 6 (IL‑6) measured with ELICA using a Cobas Pro device [Roche Diagnostics]; D‑dimer measured by coagulometry using a Siemens Atellica COAG 360 device [Siemens Healthineers]), treatment options, and clinical outcomes (pneumonia, length of hospital stay, survival at discharge or death) was collected from all participants. Some data were presented in our previous paper, in which we also analyzed the association between cardiovascular drugs and mortality rates.19 Only cardiac and inflammatory biomarkers on admission (day 1 or 2) were considered. The diagnosis of pneumonia was confirmed using imaging studies such as chest X‑ray or high‑resolution computed tomography (CT) performed soon after admission. The data of survivors and nonsurvivors were compared, and were additionally analyzed according to the presence of previously diagnosed CHF. The study was approved by the Jagiellonian University Ethics Committee (no. 1072.6120.278.2020) and conforms to the ethical principles outlined in the Declaration of Helsinki.
Statistical analysis
We used the SAS software, version 9.2 (SAS Institute, Cary, North Carolina, United States) for database management and statistical analysis. The results were expressed as numerical values and percentages for categorical variables and as mean (SD) or median and interquartile range (IQR) for continuous variables. For the assessment of means or proportions between the study groups, we applied the t test or the χ2 test, accordingly. In the case of nonparametric data, we used the Wilcoxon signed‑rank test.
We analyzed the ability of hs‑cTnT or NT‑proBNP levels to identify participants with a higher risk of death due to COVID‑19 by constructing receiver operating characteristic (ROC) curves and calculating the area under the ROC curve (AUC) using the Mann–Whitney test. Then, we estimated the optimal cutoff points for hs‑cTnT and NT‑proBNP to determine individuals with a higher probability of death. We calculated the closest point to (0,1) using the following formula: the square root of ([1‑Sensitivity]² + [1‑Specificity]²). The test result value corresponding to the point with the shortest distance (D) was indicated as the threshold cutoff point. Independent predictors of in‑hospital death were explored in logistic regression analyses. The following variables were included into the models: age above 65 years, male sex, presence of arterial hypertension, diabetes mellitus, coronary heart disease, stroke, or atrial fibrillation, a 10‑mg/l increase in hs‑CRP, as well as 10‑ng/l and 100‑pg/ml increase in hs‑cTnT or NT‑proBNP, respectively. In all analyses, P values below 0.05 indicated statistical significance.
Results
Study population
A total of 1729 consecutive patients with COVID‑19 were hospitalized from March 6, 2020 to October 15, 2020. The study population consisted of 886 men (median [IQR] age, 62 [50–74] years) and 843 women (median [IQR] age, 64 [51–77] years). Pneumonia diagnosed using chest X‑ray or CT was present in 1075 patients (62.2%). On admission, 179 individuals had CHF (10.4% of the entire cohort). The proportion of patients receiving heart failure treatment identified on admission was as follows: β-blockers were used in 137 cases (76.5%), diuretics in 134 (74.9%), angiotensin‑converting enzyme inhibitors (ACEIs) or angiotensin receptor blockers (ARBs) in 55 (30.7%), and mineralocorticoid receptor antagonists in 53 (29.6%). During hospitalization, the following drugs were used for COVID‑19 treatment in the study population: dexamethasone in 465 patients (26.9%), remdesivir in 64 (3.7%), and tocilizumab in 5 (0.3%).
Patients with high‑sensitivity cardiac troponin T assessed on admission
The values of hs‑cTnT were available on the first or second day after admission in 1041 patients (60.2% of the entire cohort). Elevated levels of hs‑cTnT, that is, values greater than 14 ng/l (>99th percentile upper reference limit [URL]), were observed in 432 patients on admission (41.5% of all patients with known hs‑cTnT). The patients with known hs‑cTnT levels were older, mostly male, and had a higher body mass index as compared with the COVID‑19 patients who did not have this marker assessed (Table 1).
Characteristics on admission | hs‑cTnT | P valuea | NT‑proBNP | P valueb | ||
Determined (n = 1041) | Not determined (n = 688) | Determined (n = 715) | Not determined (n = 1014) | |||
Data are presented as mean (SD) or median (interquartile range) unless indicated otherwise.
a P <0.05 for differences between patients with a determined vs not determined level of hs‑cTnT on admission
b P <0.05 for differences between patients with a determined vs not determined level of NT‑proBNP on admission
c Data available in: 697 patients for BMI, 1440 patients for D‑dimer, 718 patients for IL‑6, and 1574 patients for hs‑CRP
Abbreviations: BMI, body mass index; COPD, chronic obstructive pulmonary disease; eGFR, estimated glomerular filtration rate; hs‑CRP, high‑sensitivity C‑reactive protein; hs‑cTnT, high‑sensitivity cardiac troponin T; IL‑6, interleukin 6; NT‑proBNP, N‑terminal pro–B‑type natriuretic peptide | ||||||
Age, y | 67.5 (14.1) | 52.9 (17.7) | <0.001 | 67.4 (17.6) | 57.6 (17.6) | <0.001 |
Female sex, n (%) | 473 (45.44) | 379 (53.78) | <0.001 | 307 (42.94) | 536 (52.86) | <0.001 |
BMIc, kg/m2 | 29.0 (5.4) | 27.8 (4.4) | 0.001 | 29.1 (5.3) | 28.2 (4.8) | 0.019 |
Pre‑existing conditions, n (%) | ||||||
Arterial hypertension | 708 (68.01) | 262 (38.08) | <0.001 | 487 (68.11) | 483 (47.63) | <0.001 |
Hyperlipidemia | 385 (36.98) | 88 (12.79) | <0.001 | 254 (35.52) | 219 (21.6) | <0.001 |
Diabetes mellitus | 329 (31.6) | 116 (16.86) | <0.001 | 237 (33.15) | 208 (20.51) | <0.001 |
Coronary artery disease | 242 (23.25) | 48 (6.98) | <0.001 | 168 (23.5) | 122 (12.03) | <0.001 |
Chronic heart failure | 155 (14.89) | 24 (3.49) | <0.001 | 131 (18.32) | 48 (4.73) | <0.001 |
Atrial fibrillation | 190 (18.25) | 43 (6.25) | <0.001 | 157 (21.96) | 76 (7.50) | <0.001 |
Stroke | 105 (10.09) | 34 (4.94) | <0.001 | 68 (9.51) | 71 (7.00) | 0.06 |
Asthma | 67 (6.44) | 39 (5.67) | 0.51 | 49 (6.85) | 57 (5.62) | 0.29 |
COPD | 70 (6.72) | 19 (2.76) | <0.001 | 57 (7.97) | 32 (3.16) | <0.001 |
Clinical course | ||||||
hs‑cTnT, ng/l | 10.62 (5.19–32.87) | – | – | 14.3 (6.32–48.05) | 7.75 (4.33–16.82) | <0.001 |
NT‑proBNP, pg/ml | 754 (214–2843) | 150 (75–895) | <0.001 | 594 (169–2199) | – | – |
Pneumonia, n (%) | 768 (73.78) | 307 (44.62) | <0.001 | 567 (79.3) | 508 (50.1) | <0.001 |
hs‑CRPc, mg/l | 51.5 (15–97) | 18.6 (5.3–57) | <0.001 | 57.1 (19.3–115) | 23.4 (6.16–64.7) | <0.001 |
D‑dimerc, mg/l | 0.86 (0.5–1.66) | 0.6 (0.4–1.0) | <0.001 | 0.95 (0.54–1.83) | 0.64 (0.41–1.18) | <0.001 |
IL‑6c, pg/ml | 31.4 (10.5–76.1) | 8.1 (1.5–25.1) | <0.001 | 32.59 (11.58–78.0) | 9.38 (1.5–27.59) | <0.001 |
eGFR, ml/min/1.73 m2 | 70 (56–90) | 90 (79–90) | <0.001 | 77 (54–90) | 90 (72–90) | <0.001 |
Length of hospital stay, d | 18 (13–28) | 14 (8–21) | <0.001 | 19 (13–30) | 15 (10–22) | <0.001 |
Death, n (%) | 183 (17.58) | 40 (5.81) | <0.001 | 153 (21.4) | 70 (6.9) | <0.001 |
Patients with N‑terminal pro–B‑type natriuretic peptide assessed on admission
NT‑proBNP values were measured on admission in 715 patients (41.4% of the entire cohort). An increased concentration of NT‑proBNP (ie, >125 pg/ml; laboratory cutoff point for normal value) was found in 583 patients (81.5% of all cases with known NT‑proBNP). The patients with NT‑proBNP levels determined on admission were older, had a higher body mass index and were more often male than the patients with COVID‑19 without available data on this parameter (Table 1). All comorbidities, with the exception of asthma, were more frequently observed in patients in whom hs‑cTnT or NT‑proBNP was assessed on admission (Table 1). Also, pneumonia was observed more frequently in imaging studies in this group of patients.
Patients with a history of chronic heart failure
Baseline characteristics of patients with COVID‑19 and a history of CHF are presented in Table 2. Among them, hs‑cTnT values were assessed on admission in 155 individuals (86.6% of all patients with CHF), while the values of NT‑proBNP were determined in 131 patients (73.2% of the group with CHF). The patients with concomitant CHF were significantly older than those without a prior history of CHF (Table 2). Comorbidities, except for stroke and asthma, were more common in COVID‑19 patients with a history of CHF. However, no differences were found in the frequency of pneumonia, the length of hospital stay, and hs‑CRP or IL‑6 values between the patients with or without CHF who had the hs‑TnT or NT‑proBNP levels measured on admission (Table 2).
Characteristics on admission | All patients (n = 1729) | hs‑cTnT determined (n = 1041) | NT‑proBNP determined (n = 715) | ||||||
CHF(–) | CHF(+) | P value | CHF(–) | CHF(+) | P valuea | CHF(–) | CHF(+) | P valueb | |
Data are presented as mean (SD), or median (interquartile range) unless indicated otherwise
a P <0.05 for differences between patients with and without a diagnosis of heart failure on admission, with a determined hs‑cTnT level
b P <0.05 for differences between patients with and without a diagnosis of heart failure on admission, with a determined NT‑proBNP level
c Data available in: 697 patients for BMI, 1440 patients for D‑dimer, 718 patients for IL‑6, and 1574 patients for hs‑CRP
d Pneumonia was diagnosed by chest X‑ray or computed tomography.
Abbreviations: CHF, chronic heart failure; others, see Table 1 | |||||||||
n (%) | 1550 (89.6) | 179 (10.4) | – | 886 (57.2) | 155 (86.6) | – | 584 (37.7) | 131 (73.2) | – |
Age, y | 60.0 (16.9) | 76.0 (11.4) | <0.001 | 65.96 (13.9) | 76.17 (11.7) | <0.001 | 65.4 (14.6) | 76.4 (10.9) | <0.001 |
Female sex, n (%) | 764 (49.29) | 79 (44.13) | 0.19 | 404 (45.6) | 69 (44.52) | 0.80 | 253 (43.32) | 54 (41.22) | 0.66 |
BMIc, kg/m2 | 28.5 (4.9) | 28.6 (5.8) | 0.92 | 29.1 (5.3) | 28.4 (5.8) | 0.37 | 29.2 (5.3) | 28.3 (5.3) | 0.35 |
Pre‑existing conditions, n (%) | |||||||||
Arterial hypertension | 816 (52.65) | 154 (86.03) | <0.001 | 574 (64.79) | 134 (86.45) | <0.001 | 370 (63.36) | 117 (89.31) | <0.001 |
Hyperlipidemia | 382 (24.65) | 91 (50.84) | <0.001 | 300 (33.86) | 85 (54.84) | <0.001 | 179 (30.65) | 75 (57.25) | <0.001 |
Diabetes mellitus | 368 (23.74) | 77 (43.02) | <0.001 | 263 (29.68) | 66 (42.58) | <0.01 | 175 (29.97) | 62 (47.33) | 0.001 |
Coronary artery disease | 195 (12.58) | 95 (53.07) | <0.001 | 157 (17.72) | 85 (54.84) | <0.001 | 96 (16.44) | 72 (54.96) | <0.001 |
Atrial fibrillation | 149 (9.61) | 84 (46.93) | <0.001 | 118 (13.32) | 72 (46.45) | <0.001 | 92 (15.75) | 65 (49.62) | <0.001 |
Stroke | 121 (7.81) | 18 (10.06) | 0.29 | 89 (10.05) | 16 (10.32) | 0.91 | 55 (9.42) | 13 (9.92) | 0.85 |
Asthma | 93 (6.0) | 13 (7.26) | 0.50 | 56 (6.32) | 11 (7.10) | 0.72 | 37 (6.34) | 12 (9.16) | 0.25 |
COPD | 62 (4.0) | 27 (15.08) | <0.001 | 48 (5.42) | 22 (14.18) | <0.001 | 37 (6.34) | 20 (15.27) | <0.001 |
Clinical course | |||||||||
hs‑cTnT, ng/ml | – | – | – | 9.1 (4.83–23.82) | 33.5 (11.09–96.79) | <0.001 | 11.86 (5.75–35.51) | 38.77 (12.42–132.43) | <0.001 |
NT‑proBNPc, pg/ml | – | – | – | 507 (175–1726) | 2446 (1103–5658) | <0.001 | 418 (136.5–1479.0) | 2446 (1097–5635) | <0.001 |
Pneumoniad, n (%) | 941 (60.71) | 134 (74.86) | <0.001 | 652 (73.59) | 116 (74.84) | 0.74 | 466 (79.79) | 101 (77.1) | 0.49 |
hs‑CRPc, mg/l | 35.8 (9.44–83.4) | 44.2 (14.3–90.90) | 0.15 | 52.65 (15.2–98.4) | 46.65 (14.5–93.98) | 0.21 | 59.7 (22.2–123.0) | 45.8 (14.3–93.8) | 0.01 |
D‑dimerc, mg/l | 0.73 (0.45–1.42) | 1.07 (0.58–1.93) | <0.001 | 0.82 (0.48–1.59) | 1.09 (0.62–2.02) | 0.002 | 0.91 (0.53–1.79) | 1.12 (0.68–2.07) | 0.04 |
IL‑6c, pg/ml | 21.91 (5.7–60.14) | 34.47 (15.53–70.48) | <0.001 | 31.32 (9.41–76.4) | 34.47 (14.09–70.48) | 0.15 | 32.31 (10.46–78.66) | 33.12 (14.72–69.31) | 0.26 |
eGFR, ml/min/1.73 m2 | 88 (69–90) | 56 (41–74) | <0.001 | 81 (61–90) | 56 (41–74) | <0.001 | 82 (60–90) | 55 (39–72) | <0.001 |
Length of hospital stay, d | 16 (11–24) | 17 (11–33) | 0.017 | 18 (13–27) | 17 (11–33) | 0.39 | 19 (130–30) | 20 (12–35) | 0.30 |
Death, n (%) | 165 (10.65) | 58 (32.4) | <0.001 | 132 (14.9) | 51 (32.9) | <0.001 | 106 (18.15) | 47 (35.88) | <0.001 |
The median values of hs‑cTnT and NT‑proBNP determined on admission were significantly higher in patients with CHF than in those without a prior CHF diagnosis: 33.5 vs 9.1 ng/l; P <0.001 and 2446 vs 418 pg/ml; P <0.001, respectively (Table 3).
Parameter | All patients | No history of CHF on admission | CHF on admission | P value | |
a P for differences in hs‑cTnT or NT‑proBNP levels between patients with or without CHF
b P for differences in death rate between patients with or without CHF
Abbreviations: IQR, interquartile range; others, see Table 1 | |||||
hs‑cTnT, ng/l | Patients, n (%) | 1041 (100.0) | 886 (85.1) | 155 (14.9) | – |
Median (IQR) | 10.6 (5.19–32.9) | 9.1 (4.83–23.8) | 33.5 (11.1–96.8) | <0.001a | |
Deaths, n (%) | 183 (17.6) | 132 (14.9) | 51 (32.9) | <0.001b | |
NT‑proBNP, pg/ml | Patients, n (%) | 715 (100.0) | 584 (81.7) | 131 (18.3) | – |
Median (IQR) | 594 (169.0–2199.0) | 418 (136.5–1479.0) | 2446 (1097.0–5635.0) | <0.001a | |
Deaths, n (%) | 153 (21.4) | 106 (18.1) | 47 (35.9) | <0.001b | |
In‑hospital course and mortality rates
The median length of hospital stay was 4 days longer in those with a hs‑cTnT or NT‑proBNP levels determined on admission than in those without these data (P <0.001). The patients who had the levels of hs‑cTnT or NT‑proBNP measured on admission also had higher levels of hsCRP, IL‑6, and D‑dimer. Moreover, pneumonia diagnosed by X‑ray or CT was confirmed the most frequently in this group of patients (Table 1).
The overall in‑hospital mortality rate was 12.9% (223 of 1729 patients). Among individuals with a known hs‑cTnT value on admission, 183 patients (17.6%) died during the hospital stay, whereas the number of in‑hospital deaths among patients with known NT‑proBNP values was 153 (21.4%). The death rates in both abovementioned groups were significantly higher (P <0.01) than in the patients who did not have hs‑cTnT or NT‑proBNP levels assessed on admission (Table 1).
In patients with a concomitant history of CHF, the mortality was higher than in those without CHF; in the group with known hs‑cTnT it was 32.9% vs 14.9%; P <0.001 and in the group with known NT‑proBNP it was 35.9% vs 18.1%, P <0.001, respectively. Mortality rates by quartiles of serum hs‑cTnT level in patients with COVID‑19 without previously diagnosed CHF were 2.4% in the first quartile and 43.4% in the fourth quartile; P <0.001 (Table 4), while death by quartiles of serum NT‑proBNP level in patients without CHF occurred in 2.1% of patients with values in the first quartile, and 42.5% of those with values in the fourth quartile; P <0.001 (Table 4).
Parameter | Quartile | |||||
1 (low) | 2 (medium) | 3 (high) | 4 (very high) | |||
a P <0.001 (χ2 test)
b P <0.001 (χ2 test)
Abbreviations: see Table 1 | ||||||
hs‑cTnTa | ||||||
Value, ng/l | <5.19 | ≥5.19 and <10.62 | ≥10.62 and <32.87 | ≥32.87 | ||
Death | No, n (%) | 242 (97.6) | 224 (95.3) | 181 (83.4) | 103 (56.6) | |
Yes, n (%) | 6 (2.4) | 11 (4.7) | 36 (16.6) | 79 (43.4) | ||
NT‑pro BNPb | ||||||
Value, pg/ml | <136.5 | ≥136.5 and <418 | ≥418 and <1478 | ≥1478 | ||
Death | No, n (%) | 143 (97.1) | 139 (95.2) | 112 (76.7) | 84 (57.5) | |
Yes, n (%) | 3 (2.1) | 7 (4.8) | 34 (23.3) | 62 (42.5) | ||
Receiver operating characteristic and logistic regression analyses
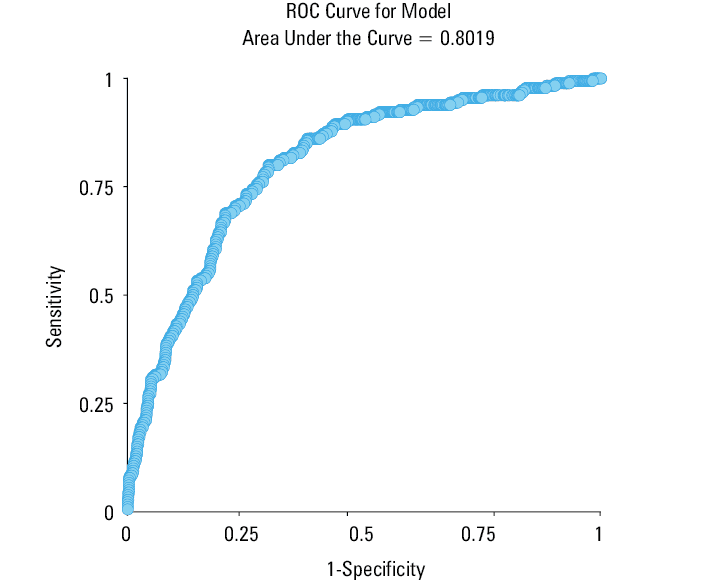
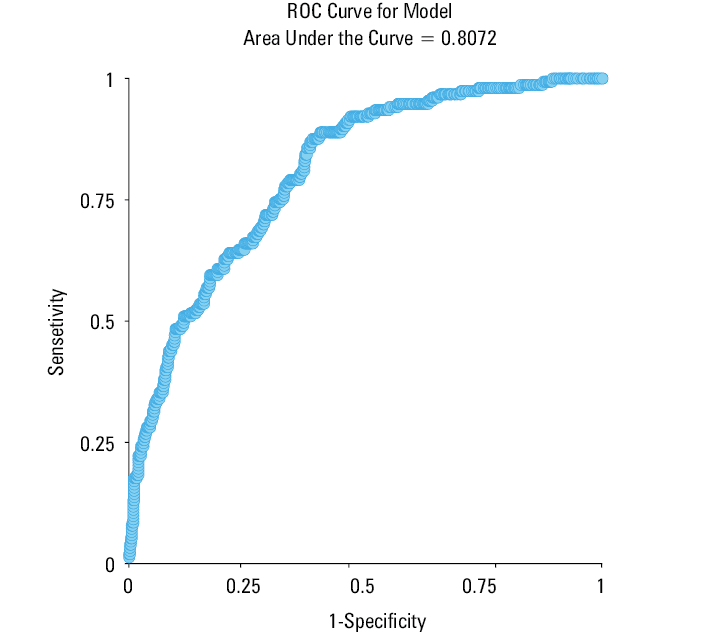
In the ROC curve analysis, hs‑cTnT values of 142 ng/l or greater measured on admission had an 80% sensitivity and a 70% specificity for predicting in‑hospital death (AUC = 0.8) (Figure 1). For NT‑proBNP, the cutoff value of 969 pg/ml had a sensitivity and specificity of 79% and 67%, respectively, for predicting in‑hospital mortality (AUC = 0.8) (Figure 2).
Logistic regression analysis showed that in COVID‑19 patients without CHF, each 10‑ng/l increase in the hs‑cTnT concentration was independently associated with a higher risk of death (odds ratio [OR], 1.01; 95% CI, 1.00–1.07; P = 0.009), based on the model of variables described in the Statistical analysis section (detailed results are presented in Supplementary material, Table S1).
Similarly, in patients without CHF, logistic regression analysis of the NT‑proBNP concentration on admission showed that for every 100‑pg/ml increase there was a greater risk of death (OR, 1.02; 95% CI, 1.01–1.03; P <0.001) (Supplementary material, Table S1).
Discussion
The study demonstrated that patients infected with SARS‑CoV‑2 who had elevated serum concentration of hs‑cTnT (>142 ng/l) and / or NT‑proBNP (>969 pg/ml) on admission had a markedly higher risk for in‑hospital death than those with lower values of these parameters. Since hs‑cTn and NT‑proBNP levels were assessed on admission in about 60% and 41% of all patients, respectively, it can be assumed that the doctors ordering these tests were guided by the assessment of the general health status of their patients upon admission. This is evidenced by the fact that most comorbidities, and also pneumonia, were observed more frequently in the patients who had the hs‑cTnT or NT‑proBNP levels measured. Additionally, the high percentage of patients with hs‑cTnT and NT‑proBNP levels evaluated on admission among individuals with CHF (87% and 73%, respectively) supports this hypothesis. Due to the fact that the frequency of myocardial injury (as defined by elevated troponin levels) among hospitalized patients with COVID‑19 increases with greater severity of the disease,20-22 it may be concluded that the frequency of testing for cardiac markers in the present study should be higher. However, in other studies, the percentage of patients in whom these markers were assessed was similar or even lower. For example, Cunningham et al23 performed a large analysis of over 48 000 patients with COVID‑19 and found that hs‑cTn and NT‑proBNP were measured on admission in 34% and 25% of individuals, respectively.
The prevalence of elevated cardiac troponin levels in individuals with COVID‑19 varies widely, ranging from 20% in cohorts of hospitalized patients to more than 40% in critically ill patients.24-26 Among our COVID‑19 cases, cardiac injury, defined by hs‑cTnT levels greater than 99th percentile URL on admission, was present in 41.5% of patients. However, considering the entire study group, regardless of the hs‑cTnT levels being determined on admission, the patients with cardiac injury accounted for 25% of the total cohort (432 out of 1729). These values are therefore similar to the results presented by other authors mentioned above.24-26
In the present study, higher NT‑proBNP values were observed in patients whose hs‑cTnT levels were measured on admission. The reverse relationship was also observed, that is, higher hs‑cTnT values were found in patients with NT‑proBNP measurements performed on admission. This means that higher values of one of the cardiac markers were accompanied by higher values of the other one. Moreover, higher values of these cardiac biomarkers were seen in more severely ill patients. This finding is consistent with recent observations that myocardial injury in COVID‑19 appears to be predominantly mediated by the severity of critical illness rather than direct injury of the myocardium from viral particles.27 Finally, in our study, the length of hospital stay was longer by 4 days in those with hs‑cTnT or NT‑proBNP levels measured on admission than in those in whom these markers were not assessed. Since the exact mechanisms leading to myocardial injury in COVID‑19 are still not well understood (whether cardiomyocyte damage dominates, as reflected by troponin leak, or whether heart overload is crucial, as reflected by natriuretic peptide increase), it seems justified to determine both biomarkers on admission to the hospital. The relationship between the concentration of cardiac troponins on admission and mortality in mild‑to‑severe and critical COVID‑19 patients was described by many authors.23,28-31 Meta‑analyses published in 2020 concluded that an increased level of high‑sensitivity troponin I (hs‑cTnI) or hs‑cTnT is strictly associated with the most severe forms of COVID‑19.32,33 Our observations are in line with these reports.
Another important observation from the present study is a significantly higher in‑hospital mortality rate among COVID‑19 patients with a history of CHF than in those without CHF. Other researchers also reported high mortality (up to 45%) in patients with CHF during hospitalization for COVID‑19.34 In our previous publication we found that, apart from older age and male sex, only diabetes mellitus and HF were independent predictors of in‑hospital death from any cause.19 In the present study, the patients with HF had higher hs‑cTnT and NT‑proBNP values on admission than the remaining patients. Undoubtedly, this result was influenced by the higher age of patients with CHF and the burden of comorbidities. Unexpectedly, we did not find differences in the frequency of pneumonia, length of hospital stay, or hs‑CRP and IL‑6 values between patients with or without CHF who had had hs‑cTnT or NT‑proBNP levels measured on admission. This fact is not easy to understand. It may be hypothesized that CHF is such a serious disease that its presence could predispose to a more frequent occurrence of viral pneumonia and a higher concentration of inflammatory markers than in individuals without CHF. Unfortunately, in our database we did not collect data on the New York Heart Association functional class of the patients with CHF, which could have also elucidated their health status and better estimate the “at entry risk.” On the other hand, it should not be forgotten that before admission to the hospital, the patients with CHF had already received the usual treatment for this disease, such as ACEIs or ARBs, mineralocorticoid receptor antagonists, β-blockers, and diuretics. As shown in our previous analysis of COVID‑19 patients, the use of these drugs during hospitalization was associated with a better prognosis, regardless of sex, age, and comorbidities.19 Nonetheless, there are also other observations about advantages and safety of ACEIs or ARBs used in the treatment of HF in COVID‑19 cases.35 A retrospective analysis recently performed in Spain showed that patients with a history of HF hospitalized for COVID‑19 who continued to receive ACEI/ARB treatment had lower rates of in‑hospital mortality and other adverse outcomes as compared with those in whom the therapy was stopped.36 Also of note, cardiac injury is not always associated with unfavorable respiratory outcomes. For instance, in a meta‑analysis published in 2021 by Bansal at al,37 cardiac injury in patients with COVID‑19 was associated with a higher risk of mortality (risk ratio [RR], 7.79), admission to the intensive care unit (RR, 4.06), mechanical ventilation (RR, 5.53), and coagulopathy (RR, 3.86), but was not associated with an increased risk of acute respiratory distress syndrome. It seems that the relationship between developing pneumonia and elevation of cardiac biomarkers during the SARS‑CoV‑2 infection needs further investigation, especially in patients with a prior history of CHF.
The importance of NT‑proBNP levels on admission in patients with CHF complicated by COVID‑19 was also explored before, although not as often as that of cardiac troponin. A single‑center study by Belarte‑Tornero et al38 involved 129 patients (43 CHF and 86 non‑CHF) with COVID‑19. All‑cause mortality was almost 2 times higher in the CHF patients than in those without CHF. A history of CHF was independently associated with 30‑day mortality (hazard ratio, 2.3); however, the patients with CHF and normal hs‑cTnT levels (<14 ng/l) had an excellent prognosis. In that study, an NT‑proBNP level greater than 2598 pg/ml on admission was associated with a higher 30‑day mortality in the patients with CHF.38 Our study included slightly more individuals with CHF (179 cases); however, the cutoff point for increased mortality in patients with COVID‑19 in the ROC curve analysis was lower, namely, 969 pg/ml. In a recently published meta‑analysis with meta‑regression, involving about 18 800 COVID‑19 cases, Zinnellu et al39 confirmed that BNP/NT‑proBNP concentrations were significantly higher in the patients with a more severe disease or nonsurvivor status than in those with low disease severity or survivor status during follow‑up.
In our hospital laboratory, the cutoff point for normal hs‑cTnT value (>99th percentile URL) was 14 ng/l, and the cutoff point for normal NT‑proBNP was 125 pg/ml. In the analyzed cohort of COVID‑19 cases without a history of CHF, even a slightly elevated level of hs‑cTnT above the reference range was associated with significantly higher mortality. As for NT‑proBNP, only an increase by about 100% above the reference range was associated with a significant increase in the number of deaths in patients without a prior history of CHF. Based on this observation, blood test results showing a slight elevation in hs‑cTnT and / or a relatively mild increase in NT‑proBNP concentrations on admission of a patient with SARS CoV‑2 infection should warrant more stringent monitoring because the risk of in‑hospital death may be greater. Other authors reported similar findings.5,11,22 In a multicenter, retrospective study of approximately 3200 patients with COVID‑19, Qin et al40 suggested that to evaluate the prognosis of patients with COVID‑19 on admission, the cutoff threshold of abnormality for hs‑cTnI, creatine kinase (CK)-myocardial band, NT‑proBNP, and CK should be lower than the currently recommended laboratory range. In their dataset, cutoff values of these cardiac markers for worse prognosis were found to be much lower (ca 50%) than the upper reference limits for the general population.40
In patients with a SARS‑CoV‑2 infection, several mechanisms could be involved in myocardial injury and the subsequent elevation of cardiac troponin and / or NT‑proBNP levels. These include acute viral infections that may cause myocarditis or pericarditis, hypoxia during the course of the disease, and endothelial dysfunction which may lead to ischemia of the heart and, in some cases, acute myocardial infarction type 2. Bacterial sepsis, cardiac adrenergic activation, and pulmonary embolism could also lead to troponin level elevation.21,41 Also, comorbidities may increase hs‑cTn values.2,42 In our study, hypertension, diabetes, coronary artery disease, atrial fibrillation, chronic obstructive pulmonary disease, and HF occurred more frequently in the group of patients who had hs‑cTnT levels measured on admission. Our results are in line with previous reports suggesting that the measurement of hs‑cTn and NT‑proBNP levels may improve risk stratification in patients with COVID‑19 in addition to the assessment of inflammatory or thrombotic markers.43-45
We must acknowledge some limitations of this study. First, it was limited by its retrospective design, inducing possible bias in data collection and result interpretation (the retrospective nature of the study did not allow us to draw conclusions about the cause‑effect relationship). Moreover, our results were obtained based on cases treated during the first 2 waves of the pandemic, with a similar protocol of COVID‑19 in‑hospital treatment. Therefore, the generalizability of our findings to asymptomatic or symptomatic COVID‑19 patients who were not hospitalized may be limited. However, we presented a large, comprehensive dataset of consecutive patients and checked the data carefully. Second, hs‑cTn and NT‑proBNP levels were not systematically monitored during the hospital stay. Although the patients were treated in a single hospital, the assessment of cardiac troponin and NT‑proBNP levels on admission was not obligatory. Third, data on concomitant diseases, including a history of HF, were obtained based on the available medical records and an interview with the patient or their relatives. Finally, echocardiography was performed on admission in a small subset of the study patients (<3%), which made it impossible to perform a reliable analysis of the heart function in relation to hs‑cTn or NT‑proBNP concentrations.
In conclusion, hs‑cTnT or NT‑proBNP predicted in‑hospital mortality in all patients with COVID‑19 included in our study. The patients with a history of CHF with concomitant COVID‑19 who had elevated cardiac troponin or NT‑proBNP levels at the time of admission to the hospital had the worst prognosis. Elevated values of hs‑cTnT and NT‑proBNP also enabled us to identify the patients with a higher risk of prolonged hospitalization time. For this reason, both cardiac troponin and NT‑proBNP should be routinely measured on admission in all patients with COVID‑19, not only in those with a history of cardiovascular disease. The results of the study support the growing evidence that simple‑to‑obtain cardiac biomarkers may help in early risk stratification of patients hospitalized for SARS‑CoV‑2 infection.
- Richardson S, Hirsch JS, Narasimhan M, et al. Presenting characteristics, comorbidities, and outcomes among 5700 patients hospitalized with COVID‑19 in the New York City area. JAMA. 2020; 323: 2052‑2059.
- Inciardi RM, Adamo M, Lupi L, et al. Characteristics and outcomes of patients hospitalized for COVID‑19 and cardiac disease in Northern Italy. Eur Heart J. 2020; 41: 1821‑1829. | Crossref
- Zhou F, Yu T, Du R, et al. Clinical course and risk factors for mortality of adult inpatients with COVID‑19 in Wuhan, China: a retrospective cohort study. Lancet. 2020; 395: 1054‑1062. | Crossref
- Grasselli G, Zangrillo A, Zanella A, et al. Baseline characteristics and outcomes of 1591 patients infected with SARS‑CoV‑2 admitted to ICUs of the Lombardy Region, Italy. JAMA. 2020; 323: 1574‑1581.
- Khan S, Rasool ST, Ahmed SI. Role of cardiac biomarkers in COVID‑19: what recent investigations tell us? Curr Probl Cardiol. 2021; 46: 100842. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION