Benefits and limitations of statin use in primary cardiovascular prevention: recent advances
Key words: cardiovascular disease, elderly, primary prevention, statin



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Benefits and limitations of statin use in primary cardiovascular prevention: recent advances
The status of low‑density lipoprotein (LDL) cholesterol is strong as an essential cause of atherosclerotic vascular disease (ASCVD) and primary target of lipid lowering. Drugs affecting primarily LDL cholesterol through an increase of LDL receptor expression are the backbone of current therapy, and generic statins are generally safe, effective, and inexpensive drugs serving this purpose. Statins are indicated for practically all patients in secondary prevention, whereas treatment in primary prevention (healthy individuals) is based on a calculated 10‑year risk of ASCVD. At “borderline” (from 5% to <7.5%) and “intermediate” (from 7.5% to <20%) risk various biomarkers (eg, coronary artery calcium) are available for accurate assessment of the individual risk. The calculation of a lifetime risk instead of the 10‑year risk can be especially useful in younger people. More information about the benefits and risks of statins in primary prevention in older people (>70 years of age) will be provided by ongoing randomized and controlled trials (STAREE and PREVENTABLE). In this narrative review, I shall present recent advances in the use of statins in younger and older healthy people, and discuss their benefits and potential risks. I also raise a question whether with the current evidence base, most people in affluent societies would benefit from taking statins.
Background
The status of low‑density lipoprotein (LDL) cholesterol as an essential cause of atherosclerotic vascular disease (ASCVD) and primary target of lipid lowering has only strengthened during the 21st century.1 Although other atherosclerotic lipoproteins contribute as well,2 drugs affecting primarily LDL cholesterol through an increase in the number of LDL receptors are the backbone of current therapy. Despite newer, effective drugs for LDL lowering, such as Proprotein Convertase Subtilisin / Kexin Type 9 (PCSK9), monoclonal antibodies and inhibitors (eg, inclisiran), and bempedoic acid, statins (inhibitors of HMG‑CoA‑reductase, the rate‑limiting step of cholesterol synthesis) remain the primary therapeutic agents due to their safety and low cost as generic drugs. Apart from lowering LDL cholesterol, they also reduce triglyceride levels and increase high‑density lipoprotein (HDL) cholesterol levels. As statins inhibit cholesterol synthesis, their combination with ezetimibe (inhibitor of cholesterol absorption) results in effective LDL cholesterol lowering with lower statin doses. Statins can also be combined with a fibrate or omega‑3 therapy (eg, icosapent ethyl) in combined dyslipidemia. For contemporary use of various hypolipidemic drugs in the treatment of dyslipidemia the reader is referred to recent reviews.3,4
Statins have been in clinical use for a long time, since 1987. They are by far one of the great achievements, and are listed among the most studied drugs in preventive medicine. Considering applicability of trial data to everyday patients, it is also important that half of the middle‑aged population in primary prevention would be eligible for at least one of the statin randomized controlled trials (RCTs).5 In general, an effective statin will halve the relative risk of an ASCVD event, the absolute benefit naturally depending on absolute risk of ASCVD. Furthermore, the actual risk of adverse effects is generally minor both in primary and secondary prevention,6-8 and reported effects in real life are often unlikely to be evoked by the statins. However, due to a wide use by millions of patients, even rare adverse effects may affect a large number of people. This is an important reason why some aspects of statin administration are continuously debated.
While only the most dedicated denialists question the use of statin therapy in secondary prevention, the discussion regarding primary prevention, that is, the use of statins in healthy people for preventive purposes, is wide‑ranging. In primary prevention, benefits obviously accumulate slower than in secondary prevention, and therefore the risk of adverse effects requires careful consideration based on absolute ASCVD risk and the optimal benefit / risk ratio.
In this narrative review, I shall present recent advances in the use of statins in younger and older healthy people, and discuss their benefits and potential risks. I also raise a question whether—with the current evidence base—most people in affluent societies would not benefit from using statins.
Current decision‑making in primary prevention: the role of biomarkers
In primary prevention aimed at people without clinical ASCVD or diabetes, risk assessment and treatment decisions are based on absolute risk of ASCVD, and there are several validated methods to assess a 10‑year risk. In the United States, pooled cohort equations or the Framingham General CVD Risk Profile are usually recommended for this purpose.9,10 The European SCORE (Systematic Coronary Risk Evaluation) and updated SCORE2, based on numerous European cohorts, are recommended by the European Society of Cardiology and the European Atherosclerosis Society.11,12 The scores are primarily based on age, sex, and a variable set of traditional ASCVD risk factors.
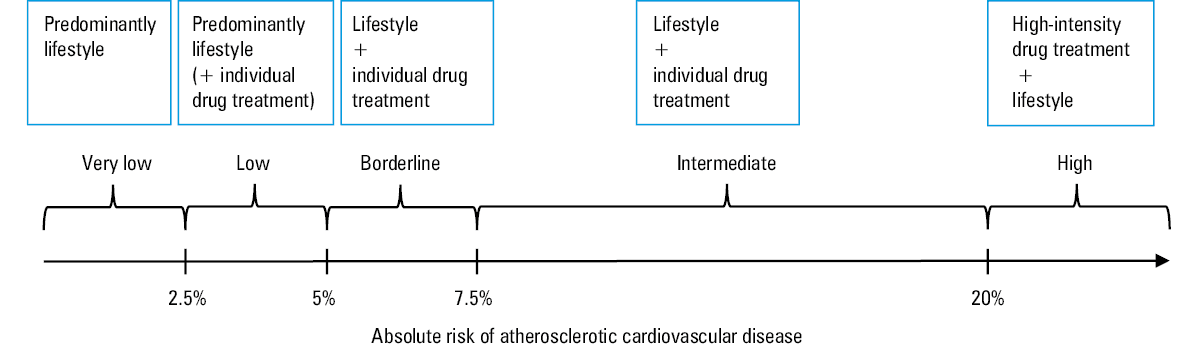
Accurate prediction of future events is always challenging and all scores may result in under- or overestimation at individual levels. The decisions are usually simple at extreme ends: predominantly lifestyle advice for very low (<2.5%) or low risk (from 2.5% to <5%), and lifestyle advice plus drug treatment for individuals at very high risk (>20%). New methods to specify the risk more accurately are needed in people with “borderline” (from 5% to <7.5%) and “intermediate” (from 7.5% to <20%) risk (Figure 1). As usual risk scores cover a 10‑year period, which is a short time for the development of a chronic disease such as ASCVD, more precision may also be needed for younger people currently at low risk. Possible risk‑enhancing factors are shown in Table 1. Detailed description of these factors and their cutoff points is outside the scope of this review but a few comments are listed here.
Factor | |
Abbreviations: ASCVD, atherosclerotic cardiovascular disease; LDL, low‑density lipoprotein | |
Genetic factors: family history of premature ASCVD, polygenic risk scores | |
Lifetime risk of ASCVD | |
High LDL cholesterol (>4 mmol/l) | |
Metabolic syndrome | |
Chronic kidney disease | |
Chronic inflammatory disease such as rheumatic arthritis, HIV | |
Premature menopause, history of pre‑eclampsia | |
High‑risk ethnicity, high‑risk social status | |
Lipid markers other than cholesterol | Primary hypertriglyceridemia |
Elevated lipoprotein(a) | |
Elevated apolipoprotein B | |
Elevated plasma ceramides | |
Elevated high‑sensitivity C‑reactive protein | |
N‑terminal pro–B‑type natriuretic peptide, high‑sensitivity cardiac troponin T | |
Low ankle‑brachial index | |
Carotid artery atherosclerosis | |
Coronary artery calcium score | |
Calculation of a lifetime risk (eg, with https://tools.acc.org/ldl/ascvd_risk_estimator/index.html#!/calulate/estimator/) may be useful for younger people and for clinician‑patient discussions about treatment benefits over the life course in primary prevention.13 In the United States, imaging coronary artery calcium (CAC) with cardiac computed tomography and scoring the result is presently considered the best additional test to aid the decision‑making for statin therapy.10 CAC is useful in younger and middle‑aged people but not so much in individuals older than 75 years.10 A practical suggestion for primary prevention has been recently presented14: CAC = 0: delay statins for 10 years; CAC = 1–99: delay statins for 5 years; CAC above 100: statin (plus non‑statin).
Biomarkers to improve the risk assessment in primary prevention include more traditional factors, such as triglycerides and lipoprotein(a) [Lp(a)], whose concentrations may provide additional clues regarding the risk. The role of triglycerides can be assessed simply by calculating non‑HDL cholesterol or apolipoprotein B to include the impact of all atherogenic lipoproteins. Very high inherited Lp(a) strongly predicts ASCVD,15 and while statins do not affect Lp(a), both PCSK9 monoclonal antibodies and inhibitors and newer drugs do.16 Chronic inflammation can be assessed with high‑sensitivity C‑reactive protein (hs‑CRP), and in the JUPITER trial a combination of elevated LDL cholesterol and CRP posed a high risk in primary prevention.17
In a large study combining the risk chart information with N‑terminal pro–B‑type natriuretic peptide (NT‑proBNP), high‑sensitivity cardiac troponin T, and hs‑CRP improved the prediction of cardiovascular disease (CVD) in older adults.18
Polygenic risk stratification has been considered a helpful way of detecting especially younger people at risk of CVD.19 However, its use is not yet generally established.20
Measurement of plasma ceramides is a promising way to assess CVD risk independently of traditional risk factors, and ceramide‑based variables have been investigated in several studies, although mainly in secondary prevention to assess a residual risk.21 Their use in primary prevention is not yet established but it is interesting that ceramides are lower among statin users, and strongly predict all‑cause mortality among octogenarian men.22
A decision to start statin treatment is based on these general principles, and what is the evidence of benefit in various risk categories. Moreover, the risk of adverse events and their seriousness, as well as the cost of treatment must be taken into account.
Current status of statins in primary prevention overall: new studies
Evidence from large‑scale RCTs shows that statin therapy efficiently reduces the risk of major ASCVD (ie, coronary death or myocardial infarction, stroke, and coronary revascularization), by about 25% for 1 mmol/l reduction in LDL cholesterol during each year of continuing the therapy.6 Also, total mortality has been reduced by 10%.
The relative risk reduction of events is independent of patient characteristics (eg, primary or secondary prevention), but absolute risk reduction depends on absolute risk (larger in secondary than in primary prevention). Accordingly, statin treatment offers benefits also in primary prevention of ASCVD, but due to a lower absolute risk in primary prevention trials at baseline and relatively short treatment periods (up to 5 years), these trials have usually been underpowered to show effects on total mortality. Furthermore, the effects of statin treatment on all‑cause mortality hinge on the proportion of ASCVD as a cause of death, and also improved treatments decrease ASCVD‑related mortality.
In an extended follow‑up, statin treatment has, however, been associated with reduced total mortality also in primary prevention. In the WOSCOPS (West of Scotland Coronary Prevention Study) all‑cause mortality was by 18% (P = 0.004) lower in the pravastatin groups than in the control placebo group over a 20‑year follow‑up.23 In WOSCOPS, mean LDL cholesterol was 4.9 mmol/l, and on‑trial LDL cholesterol was around 3.4 mmol/l, which is clearly higher than recommended in current guidelines. Consequently, the use of pravastatin 40 mg in this 1990s study of high‑risk men was suboptimal according to the current guidelines. In general, it is very important that statin treatment was shown to reduce ASCVD risk during each year it was continued. Consequently, absolute benefits would increase with a prolonged therapy, and these benefits also persist long‑term,6 as shown in the WOSCOPS follow‑up.23 Results of short‑term RCTs confirm the strong associations between LDL cholesterol and ASCVD events observed in Mendelian randomization studies.24 Moreover, ASCVD outcomes noted in trials usually do not account for recurrent events, so the total benefit is probably greater.
As there used to be fewer women in RCTs, their benefits of especially high‑intensity statins in primary prevention are less clear. This situation has gradually improved, and recently a large register study in the Netherlands, comparing 17 008 statin users and 30 793 nonusers without CVD, suggested that the protective effect of primary prevention with statins was actually stronger in women than men for both all‑cause and CVD mortality.25 Moreover, the study showed that fewer women eligible for statin therapy received statins as compared with men, and when they did, they more often received a low‑intensity statin.
When a large proportion of a population is treated, it is imperative to assess also the economic impact and cost‑effectiveness of the statin therapy. The demonstrated benefits and general safety (see below) of statin treatment, and the advent of generic pricing have broadened the statin eligibility. The cost‑effectiveness of broadening preventive statin eligibility in primary prevention of CVD was evaluated using a computer simulation model in adults aged 40 years or older. The model was built from the Scottish health sector perspective and used a cohort survey and register data.26 The main outcome measure was the lifetime incremental cost‑effectiveness ratio evaluated as cost (GBP 2020) per quality‑adjusted life year gained. The results showed that generic pricing rendered preventive statin therapy cost‑effective or even cost‑saving for many adults.
Current status of statins in primary prevention in older people: new and ongoing studies
Treatment of older adults, that is, those over 75 to 80 years, with lipid‑lowering drugs has been disturbed by the repeated and often falsely interpreted observational studies showing that older people with low plasma cholesterol levels have worse prognosis.27 However, this may be due to a reverse causality, for example, low‑grade inflammation, subclinical disease and frailty lower cholesterol levels and also increase mortality risk. This is supported by Mendelian randomization studies indicating that high LDL cholesterol level maintains its role as a risk factor even in the oldest‑old,28 and the “low cholesterol‑higher mortality” association is not observed when LDL cholesterol concentration is reduced medically, that is, with statins.29 Consequently, “exogenous” (therapeutic) cholesterol lowering must be differentiated from cholesterol lowering due to internal, “endogenous” mechanisms.
The problems of older and especially oldest‑old people are further complicated by difficulties in recognizing people potentially benefiting from statin therapy. RCT findings in younger patients and subgroups of patients aged 75 years or older as well as the results of observational studies support secondary prevention of ASCVD also in the oldest patients, but trial evidence in primary prevention is less clear.6,30 The absolute risk is high due to advanced age (reflecting long‑term predisposition to risk factors) but there are no RCTs specifically involving people older than 80 years at baseline. Consequently, the guidelines have been reluctant to support a routine statin therapy for primary prevention in adults older than 75 years, and emphasized shared decision- making and heterogeneity of the older adult population, spanning from the robust to the most frail. On the other hand, available data do not imply specific harms in older patients (see below), and therefore also judicious primary prevention is possible.
Furthermore, there are observational studies that suggest that statin treatment is useful at least in people over 75 years in primary prevention.29,31,32 In a systematic review and meta‑analysis of observational studies, statin therapy in older people (≥65 years) without CVD was associated with by 14%, 20%, and 15% lower risk of all‑cause mortality, CVD death, and stroke, respectively.33 This beneficial association with the risk of all‑cause mortality was significant also at higher ages (>75 years), in both men and women, but only in people with diabetes.
Ideally, the treatment of hypercholesterolemia should be started far earlier than at the age of 75–80 years, and there is no need to discontinue statin treatment due to the age alone.34 However, persons older than 75 years are biologically a very heterogeneous group with frequent frailty, comorbid conditions, and multiple concomitant drugs. All these, as well as personal preferences, must be taken into account in treatment decisions, both when continuing a treatment started earlier in life and considering implementation of statins de novo in old age. The following points should be addressed: life expectancy (it takes 1–2 years of treatment before benefits are seen), risk of vascular events, capacity of a statin to reduce this risk also in old age, competing causes of deaths, and risk of genuine adverse effects, for example, due to drug interactions. In general, statins seem safe also for older adults, even those with frailty.35 As all prevention drugs, statin treatment can be discontinued when palliative treatment is started.
Ongoing trials in older people
RCTs in individuals older than 75 years should provide more information about primary prevention in old age, and 2 megatrials are currently ongoing about benefits and risks of statin treatment among older adults.
STAREE (Statins in Reducing Events in the Elderly)36 is the first placebo‑controlled RCT of statin therapy specifically in a cohort of adults aged 70 years and over. STAREE is a community‑based trial across Australia and it will last for an average of 5 years. At baseline, all participants (n = 18 000) are independent and free‑living in the community. The primary end point is either the time from randomization to death or development of dementia (as measured by cognitive function tests), or development of disability (as measured by the KATZ ADL 33 test), or to a major fatal or nonfatal CVD event. The points in Table 2 will be addressed in STAREE.
Can statins prevent the first heart attack or stroke in older adults? |
Can statins prevent cognitive decline (dementia)? |
Can statins improve healthy life expectancy? |
Do statins impact day‑to‑day physical functioning? |
Comparison of adverse reactions between statin and placebo |
Risk of developing diabetes during statin treatment |
Is statin therapy cost‑effective in healthy older adults? |
Another ongoing trial in older adults is PREVENTABLE (Pragmatic Evaluation of Events and Benefits of Lipid‑lowering in Older Adults), a study funded by the US National Institute on Aging.37,38 It is an RCT comparing 40 mg atorvastatin with placebo among community‑dwelling older (≥75 years, n = 20 000) adults without clinically evident cardiovascular disease, significant disability, or dementia at baseline. The participants will be followed for an estimated median of 3.8 years at 100 United States sites. PREVENTABLE will specifically compare the incidence of new dementia and chronic disability in these 2 groups.
Together, STAREE and PREVENTABLE are anticipated to fill in the knowledge gaps regarding the benefits and risks of statin treatment in oldest patients in primary prevention; the outcomes of STAREE shall be available in 2023, and of PREVENTABLE in 2027.
Current urrent considerations of adverse effects
As presented above, statin treatment and its cost‑effectiveness in primary prevention are mainly affected by 3 aspects: benefits, adverse effects, and costs. The benefits are established (although they surface slower than in secondary prevention), and the cost is no more an issue after introduction of generic pricing. Therefore, potential adverse effects are the main players for cost‑effectiveness. Among healthy older participants enrolled in statin trials, perceived adverse effects and their related impact were the key factors contributing to permanent study drug discontinuation. Consequently, it is essential that all adverse effects experienced by the patient, whether in the end truly caused by the drug, are taken seriously.
Adverse effects of statins observed in RCTs have been mainly related to the muscles, liver, and glucose metabolism. In addition, there have been miscellaneous concerns (mostly from observational studies) about potential effects on cognition, neurological functions, pancreas (pancreatitis), kidney function, intracerebral hemorrhage, and eyes (cataract). As statins are often used in patients with polypharmacy, it is important to recognize potential drug interactions.
Muscles
Statin therapy can cause myopathy (defined as muscle pain or weakness with a large increase in creatine kinase levels), but this is rare and most muscle‑related symptoms are not myopathies. As a myopathy can be serious, patients are warned about the possibility of muscle pain or weakness when prescribed statins, and because of those warnings, some may then report such symptoms. Consequently, observational studies involving the routine use of statins, which necessarily cannot involve blinded control, may well misattribute symptoms to the statins. A marked increase in muscle enzymes (creatine kinase) and substantial muscle effects are rare, but in a worst case scenario can lead to rhabdomyolysis as demonstrated during treatment with highly potent cerivastatin.39 With currently used statin medication, the incidence of rhabdomyolysis is assessed to be 1–3 cases per 100 000 patient‑years.40
In registry‑based studies, various muscle symptoms related to statin use are reported among 7%–29% of statin users, and various muscle complaints are the most important cause of statin discontinuation. However, in several placebo‑controlled trials, the reported muscle symptoms were similar in statin and placebo groups.6 For example, in a large Heart Protection Study similar proportions of participants reported muscle‑related symptoms after about 5 years (32.9% simvastatin vs 33.2% placebo).41 Accordingly, a substantial share of symptoms in everyday practice may actually be due to the nocebo or “drucebo” effect14,42 (see below).
Consequently, while the symptoms must always be taken seriously, statin treatment should not be discontinued before other potential causes are excluded, these including specific exercise, hypothyreosis, vitamin D deficiency, and drug interactions. However, in about 5% of cases muscle symptoms may truly be due to statins. Genetic disposition (SLCO1B1 polymorphism),43 specific effects on mitochondria, or ubiquinone metabolism may contribute. A very rare cause of myopathy can be due to an immunological mechanism (anti‑HMG‑CoA‑reductase antibodies).44
True statin intolerance may be treated by changing to another statin, lowering its dose, switching to every other day or once a week dosing, combination with ezetimibe (whereupon statin dose can be reduced).14 Also combining with ubiquinone can be tried.45 With these procedures it is nevertheless vital that optimal lipid lowering is maintained. Naturally, switching to a PCSK9 inhibitor is possible but cost may be an issue.
Liver
The possible increase in liver transaminases has been recognized from the very beginning, and its incidence is 0.5%–2.0% among statin users. However, its clinical significance is unknown, and elevated liver enzymes are not as such a contraindication for statin treatment.6 Statins are not considered to show liver toxicity and a true cause and effect relationship with statins in very rare cases of hepatic failure has not been established. Consequently, other causes of liver diseases in a statin user must always be excluded.
Glucose metabolism and type 2 diabetes
Statin treatment slightly increases the risk of new‑onset type 2 diabetes. A meta‑analysis of 13 trials including over 90 000 patients demonstrated that statin increased the risk of diabetes by 9% vs placebo.46 The risk is higher with a high‑intensity statin and among older people. On the other hand, diabetes risk is higher among those statin users who are already at a risk of developing diabetes. The clinical significance of statin‑induced diabetes is unclear, as statins improve prognosis among patients who develop diabetes during statin treatment as well as among those with previous diabetes.6,47 The risk of diabetes emphasizes the important role of a healthy diet in statin users.
Neurological and cognitive symptoms
Observational studies have suggested rare cases of statin treatment‑associated neuropathy but this has not been observed in RCTs.48 There have been concerns about cognitive changes but observational studies have rather suggested that statins may protect from dementia.49 Moreover, RCTs confirmed that statin treatment reduced the number of ischemic stroke events,6 which are a risk factor for dementia. Still, the general opinion is that statin treatment does not affect cognition and cannot be used for dementia prevention.6 More light on this matter will be shed by the ongoing PREVENTABLE RCT with a primary end point of new dementia (see above).37,38
Nonvascular disease and cancer
It is especially important for primary prevention that early concerns about statins increasing the risk of nonvascular disease have been repeatedly refuted.6 In contrast, statins may even have beneficial effect in some cancers but this is not established.50
Hemorrhagic stroke
While statin treatment reduces the risk of ischemic stroke, there has been much controversy about their relationship with intracerebral hemorrhage.6,51 In any case, the risk is probably minor, although caution may be indicated with lobar intracerebral hemorrhage related to cerebral amyloid angiopathy.
Frailty
As statin may be associated with muscle‑related effects, there have been concerns that vulnerable individuals with frailty, often associated with sarcopenia, would be at special risk. In a meta‑analysis of 6 cohort studies where frailty was assessed, statin treatment was associated with lower mortality at least in secondary prevention, whereas no studies concerning primary prevention were identified.35
Interactions
Co‑administration of statins with several other medications (eg, cyclosporine, clarithromycin, protease inhibitors) may cause drug‑drug interactions and requires careful attention when prescribing. Also some herbal agents and foods that interact through common enzymatic pathways with statins can cause adverse effects.4,52
Miscellaneous concerns
While some observational studies have raised concerns about the risk of pancreatitis during statin treatment, incident cases were actually fewer in statin‑treated patients in RCTs.53 There have been inconsistent results on a link between cataract and statin treatment from observational studies, not verified in RCTs.6 In general, reverse causality and nocebo effects (see below) must always be taken into account when assessing the results from observational studies.
Nocebo effect
Nocebo is a counterpart of placebo, a patient‑centered negative response with physiological effects and symptoms. An individual may anticipate adverse effects that become self‑fulfilling and are not due to pharmacological effects.14 This bias is likely to be exacerbated by medical or nonmedical sources that emphasize possible adverse effects.
The role of nocebo in adverse effects experienced during statin treatment is supported by several findings. For example, the most frequent adverse effect of statins, namely muscle complaints, have been equally prevalent in statin and placebo groups, and discontinuation rates have been usually similar. Also n = 1 studies support a drucebo effect,42 as adverse effects have not been necessarily different between statin and placebo groups.54,55 However, it must be emphasized that statins do have also “real” adverse effects, and symptoms must be taken seriously lest patient adherence is lost.
Pleiotropic effects and are there new indications for statins?
Inhibition of HMG‑CoA reductase affects also other pathways apart from that leading to cholesterol synthesis. Statins are known to have various anti‑inflammatory and immunomodulating properties, which might be beneficial in other clinical conditions than ASCVD. These properties were named “pleiotropic” effects, although differentiating them from lipid effects is not straightforward. A systematic review analyzed 58 publications that in general supported the beneficial pleiotropic effects of statin use in contrast‑induced nephropathy, head injury, Alzheimer’s and Parkinson’s diseases, nuclear cataract, prostate cancer, infection management, and spinal cord injury.56 RCTs are nevertheless required to confirm these observations.
Future directions of primary prevention: statins for (almost) everyone?
As presented above, sophisticated methods to assess risk in healthy people are and will be available. But a provocative question may be raised: what is their relevance and is their use cost‑effective? In 2003, Wald and Law presented their concept of a “polypill”, that is a combination of low‑dose preventive drugs for CVD. According to their calculations, a polypill for all people over 55 years of age in Westernized populations would prevent more than 80% of cardiovascular events.57 This kind of “medicalization” has naturally met with resistance but gradually evidence base for this approach has grown. Polypill promotes better adherence,58 a serious problem in primary prevention, and according to meta‑analyses of RCTs, a polypill regimen decreases the incidence of fatal and nonfatal cardiovascular events particularly in low‑risk and primary prevention populations.59
A statin is one, and maybe the most important component of a polypill, and the efficacy, very low cost and excellent safety record of statins make them attractive for an umbrella therapy also in primary prevention. Actually, a decision analysis provocatively suggested that the preferred strategy is to treat all people with atherosclerotic cardiovascular risk above 2.5%.60,61 According to a modelling study of a 30‑year risk in people aged 30 to 59 years and not eligible for statin treatment under most guidelines, intensive lipid‑lowering should begin in individuals between 40 and 59 years of age and with non‑HDL cholesterol levels exceeding 160 mg/dl (4.15 mmol/l corresponding to LDL cholesterol of 3.35 mmol/l).62 The question of primary prevention and statins should shift from “whether” to “when”63: lipid‑lowering treatment in people at risk should begin before advanced vascular lesions develop. Even younger people need to consider the primary prevention concerning all ASCVD risk factors.64 This approach of making earlier treatment decisions would also relieve us from pondering statin initiation in older people: when a statin has been prescribed earlier, old age alone is not a reason to stop it.34 Naturally, it takes a while till we are in that situation, and in the meantime implementing statins for primary prevention, especially in older people, will be better informed once the results of ongoing STAREE and PREVENTABLE trials are available.
- Mach F, Baigent C, Catapano AL, et al. 2019 ESC/EAS Guidelines for the management of dyslipidaemias: lipid modification to reduce cardiovascular risk. Eur Heart J. 2020; 41: 111‑188.
- Borén J, Taskinen MR, Björnson E, Packard CJ. Metabolism of triglyceride‑rich lipoproteins in health and dyslipidaemia. Nat Rev Cardiol. 2022 Mar 22. [Epub ahead of print]. | Crossref
- Ferraro RA, Leucker T, Martin SS, et al. Contemporary management of dyslipidemia. Drugs. 2022; 82: 559‑576. | Crossref
- Hassen LJ, Scarfone SR, Milks MW. Lipid‑targeted atherosclerotic risk reduction in older adults: a review. Geriatrics. 2022; 7: 38. | Crossref
- Pavlovic J, Greenland P, Deckers JW, et al. Comparison of ACC/AHA and ESC guideline recommendations following trial evidence for statin use in primary prevention of cardiovascular disease: results from the population‑based Rotterdam Study. JAMA Cardiol. 2016; 1: 708‑713. | Crossref
ARTICLE INFORMATION