Solitary multiple myeloma as a very rare cause of hypophosphatemia, micturition, and defecation disorders



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Solitary multiple myeloma as a very rare cause of hypophosphatemia, micturition, and defecation disorders
A 53‑year‑old man with no history of chronic diseases was admitted to the hospital due to lumbar pain. Magnetic resonance imaging showed a vertebral tumor‑like mass at the L5/S1 level (Figure 1A–1D). Basic laboratory results were normal. An open biopsy of the mass was performed. Pain exacerbation and leg muscle weakness appeared, and urination and defecation problems developed. Radiotherapy was introduced to reduce the neurological problems. The total radiotherapy dose was 20 Gy divided into 4 Gy fractions administered on 5 consecutive days (Figure 1E).
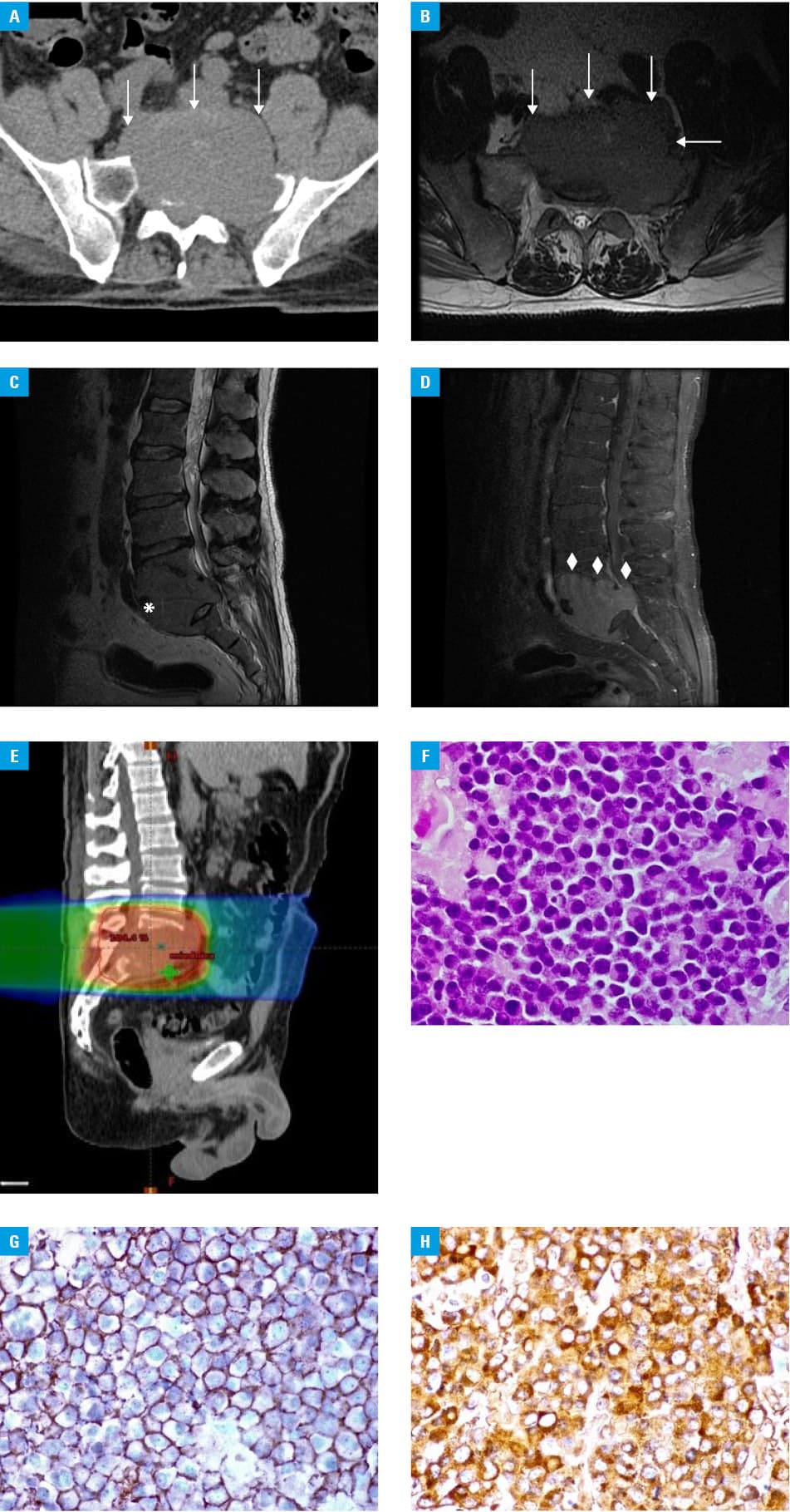
Histopathological examination showed the infiltration of plasma cells with various degrees of morphological maturity. Immunophenotyping revealed CD138+, λ+ > κ+ (Figure 1F–1H). Plasma cell tumor was diagnosed based on the following results: CD20–, CD3–, cyclin D1–, CK Pan–, CD38+, CD56+ and Ki‑67 of approximately 65%.
Additional tests revealed an increased total serum calcium concentration of 6.02 mmol/l (normal range, 4.3–5.1 mmol/l), decreased serum albumin of 2.5 g/dl (normal range, 3.5–5.2 g/dl), elevated white blood count (WBC) of 18 150/mm3 (normal range, 4800–10 000/mm3), increased neutrophil count, normocytic and normochromic anemia with hemoglobin of 12.1 g/dl (normal range, 13.0–16.5 g/dl), and elevated erythrocyte sedimentation rate of 50 mm/h (normal range <15 mm/h).
Bone marrow cell immunophenotyping revealed no clonal plasma cells. Serum and urine proteinogram showed monoclonal proteins in the γ globulin fraction. Monoclonal immunoglobulin (IgG) λ protein was found with serum and urine immunofixation. The concentration of κ free light chains (FLCs) in the serum was 13.24 mg/l (normal range, 3.3–19.4 mg/l) and the concentration of λ FLCs was 66.86 mg/l (normal range, 5.71–26.3 mg/l). The κ/λ ratio was 0.198 (normal range, 0.26–1.65). The urine concentration of κ FLCs was 26 mg/l (normal range, 0.78–13.48 mg/l) and that of λ FLCs was 8.41 mg/l (normal range, 2.22–5.9 mg/l). The κ/λ ratio in the urine was 3.082 (normal range, 2.04–10.37). Ig concentrations were as follows: IgA 64 mg/dl (normal range, 70–400 mg/dl), IgG 2302 mg/dl (normal range, 700–1600 mg/dl), and IgM 75 mg/dl (normal range, 40–230 mg/dl). Based on the above results, extramedullary IgG λ myeloma was diagnosed.
Chemotherapy was introduced according to the VTD (bortezomib, thalidomide, dexamethasone) regimen. The chemotherapy decreased the serum phosphate level to 1.48 mg/dl (normal range, 2.7–4.5 mg/dl). The tubular reabsorption of phosphate of 97% (normal range >86%) and the ratio of the tubular maximum reabsorption of phosphate of 1.65 mg/dl (normal range, 3.0–5.0 mg/dl) did not confirm the tubular phosphate loss.1 Seemingly, hypophosphatemia was caused by a shunt from the extracellular to intracellular space. Excessive phosphate transport in the cancer patient resulted from intensive nutrition with a low‑phosphate diet (anabolic phase), and steroid therapy.2 However, in the case of a myeloma patient in whom hypophosphatemia is detected, the possibility of a pseudohypophosphatemia “phenomenon” (resulting from the interference of myeloma paraproteins with some biochemical phosphate markers) should always be considered, as such pseudohypophosphatemia does not require treatment.2 A decreased serum 25‑hydroxyvitamin D concentration of 5.96 ng/ml (normal range, 20–30 ng/ml) was observed. The patient was treated with phosphate‑rich diet, intravenous phosphate supplementation, and oral cholecalciferol.
Very good partial response was achieved with the remission induction regimen (VTD) and salvage radiotherapy. Neurological symptom alleviation and WBC reduction were observed.3 Multiple myeloma is a rare malignant neoplasm of the hematopoietic system. The isolated form described above accounts for 2%–5% of all plasma cell neoplasms. It is most commonly located in the vertebral bodies. The patient was prepared for hematopoietic cell autotransplantation.4
Regrettably, the diagnosis was delayed in this patient, because the health care system was facing problems related to patient care during the COVID‑19 pandemic.5
- Stompór T, Zabłocki M, Pankrac K. Renal involvement in multiple myeloma. Pol Arch Med Wewn. 2012; 122: 443‑438. | Crossref
- Jeffs P, Mangual‑García M, González‑Bóssolo A, Rivera‑Santana N. Transient hypophosphatemia: a dangerous event in multiple myeloma. Case Rep Endocrinol. 2021; 2 021: 3609346. | Crossref
- Schütz NP, Ochoa P, Duarte P, et al. Real world outcomes with bortezomib thalidomide dexamethasone and cyclophosphamide bortezomib dexamethasone induction treatment for transplant eligible multiple myeloma patients in a Latin American country. A retrospective cohort study from Grupo Argentino de Mieloma Múltiple. Hematol Oncol. 2020; 38: 363‑371. | Crossref
- Czyż J, Jurczyszyn A, Szudy‑Szczyrek A, et al. Autologous stem cell transplantation in the treatment of multiple myeloma with 17p deletion. Pol Arch Intern Med. 2020; 130: 106‑111. | Crossref
- Weller D. Cancer diagnosis and treatment in the COVID‑19 era. Eur J Cancer Care (Engl). 2020; 29: e13265. | Crossref
ARTICLE INFORMATION