A 52‑year‑old woman was admitted to the General Surgery Department for further workup of a left adrenal gland tumor. The patient complained of pain and discomfort in the epigastric region, dysphagia, fatigue, and weight loss over the course of several months.
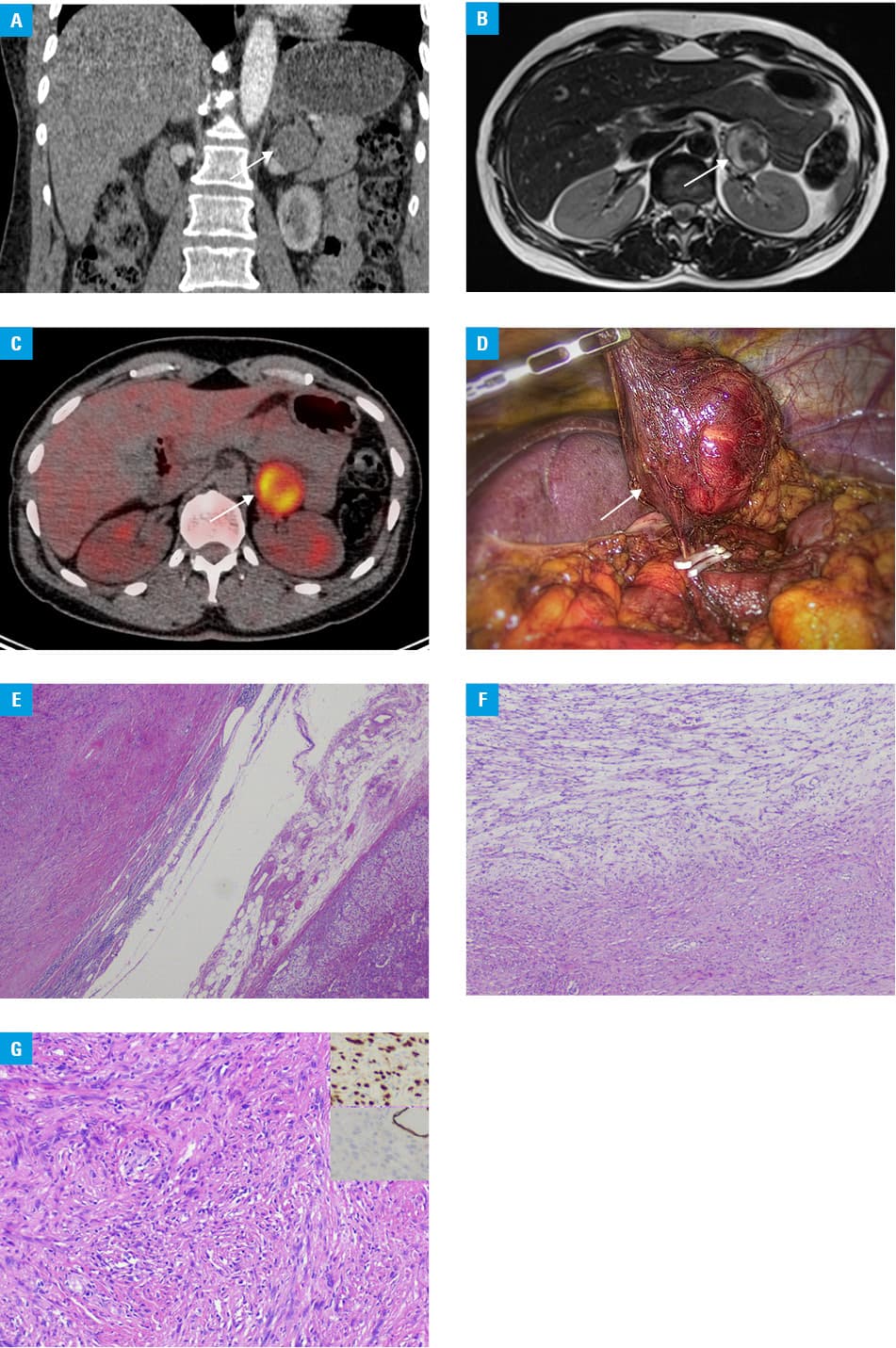
Past medical history revealed that 8 years before the current admission the patient had been diagnosed with and treated for skin melanoma. The primary neoplastic skin lesion, located on her left foot, had been resected, and since the procedure the patient has continued with regular oncological follow‑up visits. A recent computed tomography scan showed a 33 × 36 × 35 mm nodular lesion in the left adrenal gland, with the density of 32 Hounsfield units, which is not typical for adenoma (Figure 1A). Magnetic resonance imaging (Figure 1B) revealed a noncharacteristic tumor (litho‑cystic and lipid‑poor), without restricted diffusion. Subsequently, positron emission tomography was performed and showed intense uptake within the left adrenal mass (40 × 34 mm) with a standardized uptake value of 10.2, which strongly indicates malignancy (Figure 1C). Additional biochemical hormonal assessment, in accordance with the guidelines of the Polish Endocrine Society,1 revealed normal activity of adrenal hormones. Due to the results of the imaging studies, the patient’s medical history, and our previous experience,2 we decided to proceed with the surgical treatment. In February 2022, a left‑sided laparoscopic adrenalectomy was performed (Figure 1D). The histopathology report described a tumor (45 × 42 × 23 mm) adjacent to the adrenal gland, with features of Schwannoma with degenerative changes (“Ancient” Schwannoma) (immunophenotype: S100+, SOX10+, HMB45–, desmin–, SMA–, CK AE1) (Figure 1E–1G).
Adrenal Schwannoma (AS) is a very rare tumor of the peripheral nerve sheath arising from Schwann cells. The term “ancient” is used to describe schwannomas showing degenerative changes and diffuse hypocellular ischemic areas.3 Despite advances in diagnostics, AS cannot reliably be differentiated from malignant lesions through imaging and, so far, histopathologic examination remains the only way to make an unequivocal diagnosis.4 In this particular case, previous medical history of melanoma led to the decision to pursue surgery; however, AS should also be added to the list of possible differential diagnoses of nonsecreting adrenal tumors suspected for malignancy.
- Bednarczuk T, Bolanowski M, Sworczak K, et al. Adrenal incidentaloma in adults ‑ management recommendations by the Polish Society of Endocrinology. Endokrynol Pol. 2016; 67: 234‑258. | Crossref
- Lewandowska‑Graban K, Zdrojewska M, Jendrzejewski J, et al. A case report of melanoma metastasis to adrenal gland. Pol Arch Intern Med. 2019; 129: 636‑637. | Crossref
- Mohiuddin Y, Gilliland MGF. Adrenal Schwannoma: a rare type of adrenal incidentaloma. Arch Pathol Lab Med. 2013; 137: 1009‑1014. | Crossref
- Incampo G, Di Filippo L, Grossrubatscher EM, et al. Adrenal schwannoma: why should endocrinologists be aware of this uncommon tumour? Endocrine. 2022; 75: 684‑697. | Crossref
ARTICLE INFORMATION