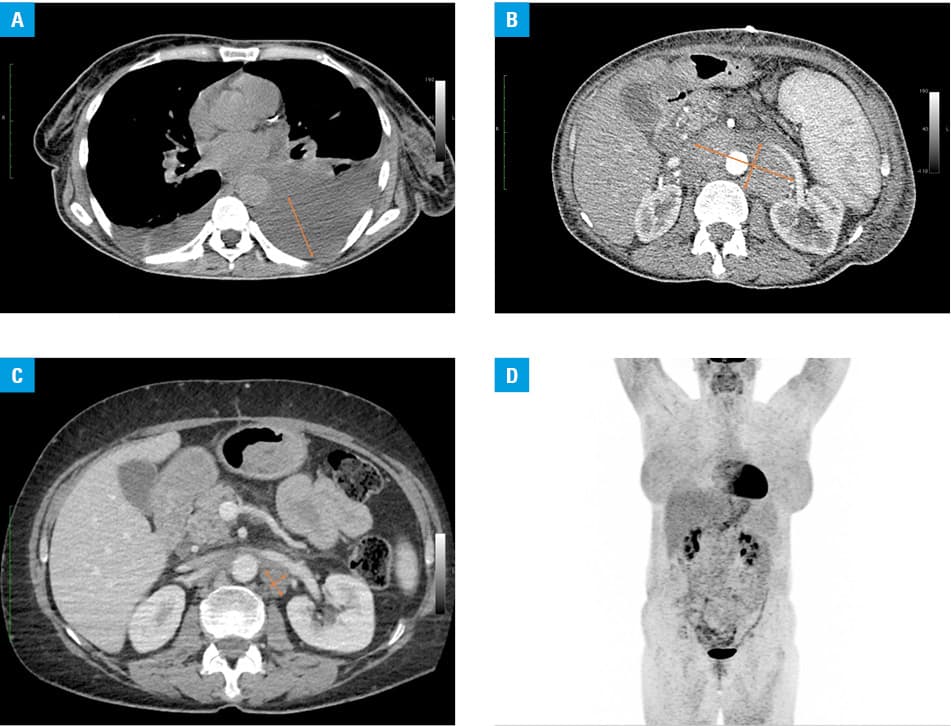
A 58‑year‑old woman, without comorbidities, was admitted to the hospital due to weight loss (10 kg in 2 months), dyspnea, and dry cough. Imaging studies (Figure 1A) revealed left hydrothorax, ascites, generalized lymphadenopathy (supraclavicular and mediastinal, with the largest retroperitoneal mass measuring 111 × 50 × 160 mm), and splenomegaly (160 mm) (Figure 1B). Biopsy of the retroperitoneal mass revealed classical Hodgkin lymphoma (HL), mixed cellularity subtype, with an international prognostic score of 2 (age, albumin). The diagnosis did not raise any doubts and the results of pathological evaluation of the lymph node were unequivocal. The pretreatment polymerase chain reaction (PCR) test for SARS‑CoV‑2 infection was positive. Dexamethasone at a dose of 8 mg/day was started, together with remdesivir for 5 days and 1 unit of convalescent plasma. Left pleural cavity drainage was required 4 times. The patient’s general condition gradually improved, but she remained PCR‑positive for SARS‑CoV‑2; therefore, chemotherapy for HL was postponed for a long time. After 5 months of supportive monotherapy with dexamethasone (8 mg daily for the first 2 weeks, later reduced to 4 mg daily in accordance with the local standards for SARS‑CoV‑2 infection management), and with persistent positive test results for SARS‑CoV‑2, the patient was referred to our department for a decision regarding further treatment. She was in a good condition, with no abnormalities in physical examination. Computed tomography (CT) showed an almost complete regression of the lymph node size in both the mediastinum and abdominal cavity, with a residual retroperitoneal node of 20 × 16 mm in size (Figure 1C). Positron emission tomography–CT (PET/CT) showed no active metabolic lesions, although prolonged steroid therapy may have decreased the fluorodeoxyglucose tracer accumulation (Figure 1D). Due to the lack of evidence of active HL, the patient was discharged with a plan of a stringent observation. After 14 months of follow‑up, she has remained free of symptoms, in complete response (CR), and SARS‑CoV‑2–negative.
Our case is the second reported HL remission likely induced by SARS‑CoV‑2 infection.1 One case of follicular lymphoma (FL) was also reported.2 The 2 other patients were of similar age, mildly symptomatic (infection stage 1), and required only supportive treatment. In the HL patient, no corticosteroid or immunochemotherapy was administered, and general resolution of lymphadenopathy as well as limitation of the coexisting Epstein–Barr virus infection were achieved during the 4‑month follow‑up. In the FL case, after the end of treatment (bendamustine plus rituximab), partial response was achieved, at which time SARS‑CoV‑2 infection was detected. PET/CT was performed at 2 and 4 months; the first one showed progression, the next, surprisingly, CR.
The reason why selected patients achieve remission after COVID‑19 is unclear. The infection might impair the interaction between tumor cells and their microenvironment,3 or SARS‑CoV‑2 might activate an immune response, including an increased production of proinflammatory cytokines,4 which is also partially directed against the tumor cells. The resulting changes in the tumor microenvironment, including a shift in macrophages, might create unfavorable conditions for tumor cells.5 In our case, the prolonged administration of dexamethasone was unlikely to have induced a prolonged CR, since steroids are not very active against HL tumor cells.
- Challenor S, Tucker D. SARS‑CoV‑2‑induced remission of Hodgkin lymphoma. Br J Haematol. 2021; 192: 415. | Crossref
- Sollini M, Gelardi F, Carlo‑Stella C, et al. Complete remission of follicular lymphoma after SARS‑CoV‑2 infection: from the “flare phenomenon” to the “abscopal effect”. Eur J Nucl Medi Mol Imaging. 2021; 48: 2652‑2654. | Crossref
- Montanari F, Diefenbach CS. Hodgkin lymphoma: targeting the tumor microenvironment as a therapeutic strategy. Clin Adv Hematol Oncol. 2015; 13: 518‑524.
- Wang C, Zhou X, Wang M, et al. The impact of SARS‑CoV‑2 on the human immune system and microbiome. Infectious Microbes & Diseases. 2020; 3: 14‑21.
- Jayasingam SD, Citartan M, Thang TH, et al. Evaluating the polarization of tumor‑associated macrophages into M1 and M2 phenotypes in human cancer tissue: technicalities and challenges in routine clinical practice. Front Oncol. 2019; 9: 1512. | Crossref
ARTICLE INFORMATION