Irregular treatment leading to pituitary and scalp involvement in metastatic breast cancer



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Irregular treatment leading to pituitary and scalp involvement in metastatic breast cancer
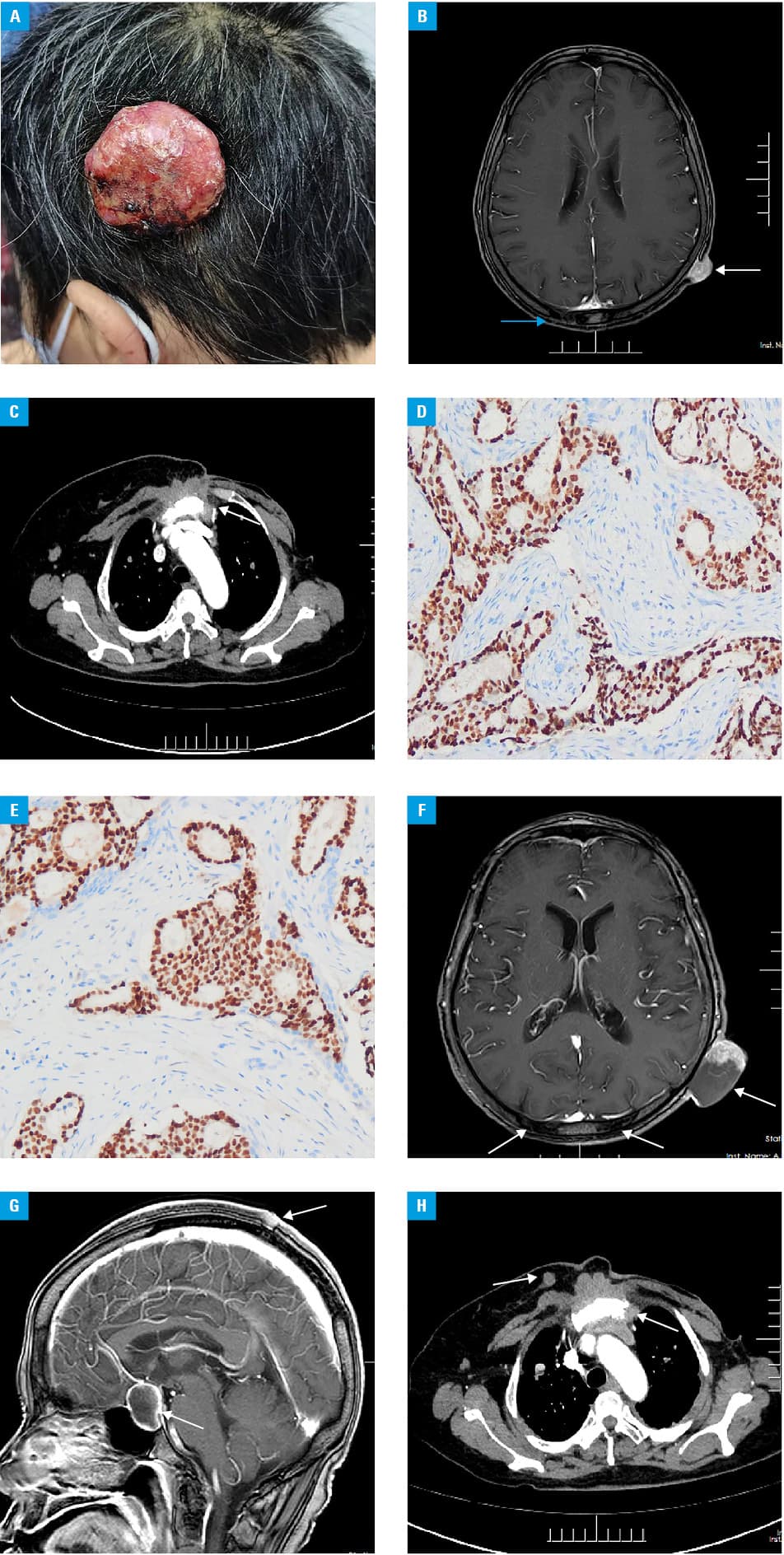
A 65‑year‑old woman presented with a painful scalp mass and severe visual impairment in the left eye that had persisted for approximately 2 weeks (Figure 1A). She had a complex history of left breast cancer that was first diagnosed in 2003, and was primarily treated with a modified radical mastectomy combined with axillary lymph node dissection. The final diagnosis was invasive breast cancer, luminal B subtype, stage I (T1N0M0); however, the patient declined adjuvant chemotherapy at that time; instead, she self‑administered traditional Chinese medicine. In 2020, contrast‑enhanced magnetic resonance imaging of the head revealed a lesion on the left scalp with strong enhancement and an abnormal skull signal (Figure 1B). Computed tomography of the chest and abdomen showed masses in the lungs and bone destruction involving the sternum (surrounded by a soft‑tissue mass) (Figure 1C), left scapula, right clavicle, bilateral ribs, cervicothoracic lumbosacral vertebral bodies and accessories, bilateral ilium, left acetabulum, and right femur. A biopsy of the scalp lesion revealed breast cancer positive for estrogen receptor (100%), progesterone receptor (70%), and human epidermal growth factor receptor 2 (1+) (Figure 1D and 1E). Considering the high level of the molecular receptor expression and her poor financial status, the patient was prescribed letrozole for endocrine therapy, zoledronic acid for antibone metastasis therapy, and capecitabine for approximately 1 year. Subsequent imaging studies showed an increase in the number and size of the metastatic foci. Additional masses were present, including a sellar mass with strong, ring‑shaped enhancement, a mass in the right breast (Figure 1F-1H), and masses on the right side of the axilla and neck. These findings supported the diagnosis of secondary breast cancer with widespread metastases. The patient and her family refused further treatment except for capecitabine. The patient died after a follow‑up period of 6 months.
The incidence of pituitary and scalp masses resulting from widespread metastatic disease is low. However, such lesions may appear as the only metastasis or the first manifestation of the primary tumor.1,2 To the best of our knowledge, this is the first reported case of metastatic breast cancer simultaneously involving the pituitary and the scalp.
Breast cancer is the most common primary tumor among patients with pituitary metastases.3 The clinical symptoms include diabetes insipidus, hypopituitarism, visual field defects, and headache. Therefore, these lesions are difficult to distinguish from benign tumors based on symptoms and imaging features alone. There are no systematic reviews on the primary lesions most commonly associated with scalp metastases, only case reports and small case series are available in the literature. Scalp metastases of breast cancer may appear as single or multiple inflammatory or nodular lesions, telangiectasias, or skin lesions of irregular shape that are flesh or reddish in color, which makes them hard to distinguish from other skin carcinomas. Scalp metastases can become ulcerated or infected. The diagnosis relies on histopathology. Imaging studies, especially positron emission tomography–computed tomography, can visualize the degree of systemic involvement.
Since pituitary and scalp metastases indicate a late‑stage primary tumor, it is not possible to change the bad prognosis associated with the dissemination stage. However, systemic treatments, including chemotherapy alone or in combination with targeted or endocrine therapy, are necessary to extend the overall survival. To alleviate local symptoms and improve the patient’s quality of life, local surgical resection and palliative antihemorrhagic radiotherapy can be performed for single lesions, especially in the case of bleeding ulcers. However, pituitary and scalp metastases of breast cancer are associated with a poor prognosis—even if treatments were administered, the median survival time was 1 to 2 years.4 Our patient was first diagnosed with breast cancer 19 years prior to the index admission, and had the mass surgically removed. However, no systemic chemotherapy or radiotherapy was administered, and fatal widespread metastases occurred. Therefore, standard treatment with regular follow‑up is important for patients with breast cancer to prevent such consequences and improve the prognosis.
- Habu M, Tokimura H, Hirano H, et al. Pituitary metastases: current practice in Japan. J Neurosurg. 2015; 123: 998‑1007. | Crossref
- Lemieux J, Desbiens C, Hogue JC. Breast cancer scalp metastasis as first metastatic site after scalp cooling: two cases of occurrence after 7- and 9‑year follow‑up. Breast Cancer Res Treat. 2011; 128: 563‑566. | Crossref
- Fredrika S, Margareta N, Daniel SO, et al. Pituitary metastases: a nationwide study on current characteristics with special reference to breast cancer. J Clin Endocrinol Metab. 2019; 104: 3379‑3388. | Crossref
- Tan AR. Cutaneous manifestations of breast cancer. Semin Oncol. 2016; 43: 331‑334. | Crossref
ARTICLE INFORMATION