Effectiveness of chronic obstructive pulmonary disease (COPD) treatment with a combination of tiotropium / olodaterol in Polish standard clinical practice as measured by the improvement of the Clinical COPD Questionnaire score: an observational study
Key words: chronic obstructive pulmonary disease, Clinical COPD Questionnaire, observational study, olodaterol, tiotropium



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Effectiveness of chronic obstructive pulmonary disease (COPD) treatment with a combination of tiotropium / olodaterol in Polish standard clinical practice as measured by the improvement of the Clinical COPD Questionnaire score: an observational study
Introduction: Health‑related quality of life in patients with chronic obstructive pulmonary disease (COPD) can be measured by the Clinical COPD Questionnaire (CCQ). In this study, the CCQ was used to assess the therapeutic success of a fixed‑dose tiotropium / olodaterol combination treatment in Polish COPD patients.
Objectives: We aimed to evaluate the changes in the CCQ score in Polish patients with COPD after 6 weeks of treatment with tiotropium / olodaterol and to assess the predictors of response to this treatment.
Patients and methods: Data of the Polish subgroup of the NIS‑CCQ observational study (NCT03663569) were extracted. COPD patients who had received a new tiotropium / olodaterol prescription were included. The primary end point was therapeutic success predefined as a 0.4‑point reduction in the CCQ score after 6 weeks of tiotropium / olodaterol treatment. Post‑hoc logistic regression analysis was performed to identify the predictors of response to the treatment.
Results: After 6 weeks of treatment, 72.4% of patients achieved therapeutic success. The therapy was successful in 83.4% of treatment‑naïve patients, as compared with 62.6% and 73.3% of those previously treated with long‑acting muscarinic antagonists or long‑acting β2 agonists in monotherapy and in combination with inhaled corticosteroids, respectively. Therapeutic success was achieved by at least 50% of patients regardless of the COPD severity and exacerbation history but it was more frequent in patients with more severe disease. The airflow limitation severity grades 2 to 4, modified Medical Research Council Dyspnea Scale classes 2 to 4, exacerbations within the last year before the study, and treatment‑naïve status predicted a better response to tiotropium / olodaterol.
Conclusions: Tiotropium / olodaterol treatment improved clinical control in Polish COPD patients. Therapeutic success was the most pronounced in individuals with more severe COPD and in the treatment‑naïve group but occurred also in those with moderate disease and in previously treated participants.
What's new?
This is the first real‑world study to analyze the use of a fixed‑dose combination of tiotropium / olodaterol in Polish patients with chronic obstructive pulmonary disease (COPD). The results demonstrate that a 6‑week treatment with tiotropium / olodaterol improved clinical control in COPD patients assessed with the Clinical COPD Questionnaire. Therapeutic success associated with the tiotropium / olodaterol treatment was the most pronounced in treatment‑naïve patients (not previously treated with long‑acting muscarinic antagonists, long‑acting β2 agonists [LABA], or inhaled corticosteroids [ICSs]), and in those with more severe COPD. Nonetheless, this therapy also proved to be beneficial in most patients with less advanced disease without any exacerbation and in those previously treated with mono- or dual ICS/LABA therapy. The duration of COPD did not affect the chance of benefiting from tiotropium / olodaterol; therefore, our results suggest that this treatment may be used in a broad group of patients with COPD.
Introduction
Chronic obstructive pulmonary disease (COPD) is a respiratory disorder causing irreversible and progressive airflow limitation.1,2 As a result, the disease significantly decreases the health status and, consequently, patients’ health‑related quality of life (HRQoL).3
HRQoL of patients with COPD can be assessed with patient‑reported outcome questionnaires evaluating the degree to which a patient’s health status affects the self‑determined quality of life (QoL).4 The Clinical COPD Questionnaire (CCQ) is an easy‑to‑use and effective QoL questionnaire strongly correlated with the St George’s Respiratory Questionnaire.5 Moreover, it is a convenient and practical tool used in clinical populations, with good reliability, validity, and responsiveness to interventions.5
The Global Initiative for Chronic Obstructive Lung Disease (GOLD) recommends the use of long‑acting muscarinic antagonists (LAMA) or long‑acting β2 agonists (LABA) as the main methods of symptom management.6 However, dual bronchodilator therapy consisting of LAMA and LABA in fixed‑dose combinations (FDCs) is more effective. It has been shown that, in comparison with monotherapy, LAMA/LABA are more efficient in reducing dyspnea and improving the lung function, lung hyperinflation, exercise tolerance, exacerbation frequency, and QoL of patients with COPD.7-10
Data on the effectiveness and safety of LAMA/LABA treatment from randomized controlled trials (RCTs) are largely consistent with those reported in real‑world studies, and reinforce the position of LAMA/LABA in pharmacological management of COPD.11 In 2019, Valipour et al12 published the results of the OTIVACTO study providing evidence of improvement in self‑reported physical functioning following tiotropium / olodaterol treatment in COPD patients from Central and Eastern European countries. In 2021, the first real‑world analysis covering a population of Polish patients was published, namely, the NIS‑CCQ study13 (Study on the Control of Chronic Obstructive Pulmonary Disease [COPD] in Patients Taking the Combination of tiotropium and olodaterol using the Respimat Inhaler; NCT03663569). It included 4819 patients, 526 of whom were Polish citizens.
The aims of the present analysis of the NIS‑CCQ study comprised the evaluation the changes in HRQoL of Polish patients with COPD after approximately 6 weeks of treatment with tiotropium / olodaterol in standard clinical practice, and post‑hoc assessment of the predictors of response to this treatment. To our knowledge, this is the first analysis of real‑life data from Polish COPD patients treated with a LAMA/LABA combination. In comparison with the COPD populations of other European Union countries, the Polish population is exposed to higher levels of air pollutants,14 a well‑known risk factor for COPD development, which strengthens the rationale to perform a detailed analysis of this population of COPD patients.
Patients and methods
Study design
The presented data are derived from a post‑hoc analysis of the Polish subgroup of patients included in the NIS‑CCQ study.13
The NIS‑CCQ was an open‑label, single‑arm, noninterventional, self‑controlled study involving patients of both sexes, aged 40 years or older, who were diagnosed by the attending physician (pulmonologist or general practitioner) with COPD requiring a combination treatment with LAMA and LABA (FDC of tiotropium bromide and olodaterol delivered in a Respimat inhaler). The patients were categorized into groups B, C or D according to the GOLD classification (the 2018 version).15
The study was performed according to the Declaration of Helsinki, International Conference on Harmonization: Harmonized Tripartite Guideline for Good Clinical Practice, and local regulations. According to the decision of the Ethics Committee of Silesian Medical University in Katowice, Poland, the study did not require ethical approval (Decision Letter from October 7, 2018). All the patients included in the study signed an informed consent before enrollment.
The exclusion criteria were as follows: (1) treatment with a LAMA/LABA combination (as individual drugs or in a combination product) within the last 6 weeks before commencement of the study (ie, none of the included patients were treated with a LAMA/LABA combination prior to the study); (2) need to continue the treatment with LABA / inhaled corticosteroids (ICS) (the decision on LABA/ICS continuation was left to the discretion of the attending physician; the patients requiring such a treatment were not enrolled in the study); (3) pregnancy or lactation; (4) current participation in another clinical trial or noninterventional study involving a drug or a medical device.
End points
The primary end point of the study was the achievement of therapeutic success, defined as a reduction in the total CCQ score from Visit 1 (baseline visit) to Visit 2 (final visit, approximately 6 weeks after initiation of the treatment) by 0.4 points.
The secondary end points included changes in the total CCQ score, the scores for individual CCQ domains (symptoms, mental state, and functional status), and a patient’s general condition (evaluated according to the Physician’s Global Evaluation [PGE] score) between Visit 1 and Visit 2. In addition, patients’ satisfaction with the tiotropium / olodaterol treatment and with handling of the Respimat device, as well as their willingness to continue the treatment were assessed at Visit 2. At Visit 1, the patients received extensive training in Respimat inhaler handling and usage. The inhalation skills with the inhaler were checked at Visit 2 according to the GOLD recommendations.
Safety was monitored from Visit 1 following the signing of the informed consent until the end of the study. Data on the safety of tiotropium / olodaterol included adverse drug reactions and serious adverse events.
Assessments
A summary of data collected from the patients and the assessments performed is illustrated in Figure 1.
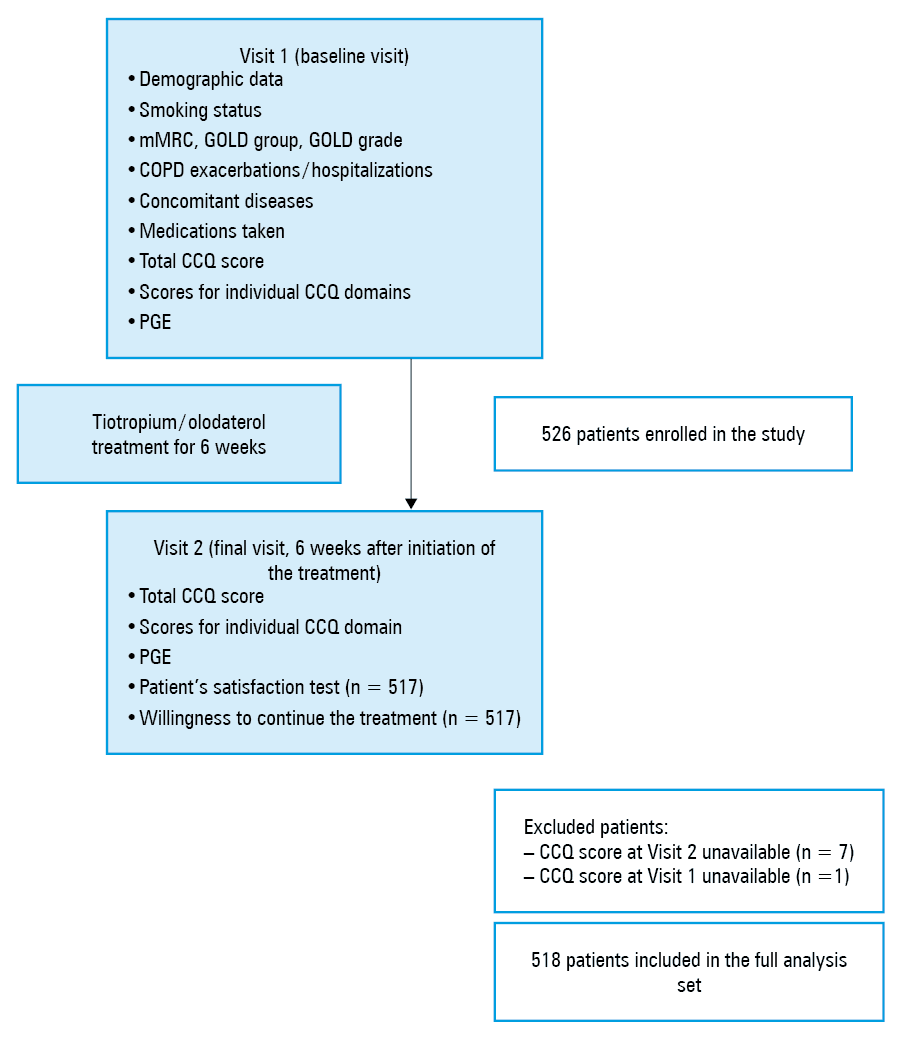
Abbreviations: CCQ, Clinical COPD Questionnaire; COPD, chronic obstructive pulmonary disease; GOLD, Global Initiative for Obstructive Lung Disease Criteria; mMRC, Modified Medical Research Council Dyspnea Scale; PGE, Physician’s Global Evaluation.
The patients completed the CCQ at Visit 1 and Visit 2. The questionnaire consists of 10 questions and covers 3 domains (symptoms, mental state, functional status). The total CCQ score is the sum of the scores assigned by a patient in response to all 10 questions divided by 10. A higher score indicates a worse condition. Each of the 10 questions is scored on a 7‑point scale, from 0 (never / not limited at all) to 6 (almost all the time / totally limited or unable to do). A reduction of the total score by 0.4 points is considered a minimal clinically significant difference (MCID).16 The percentage of patients achieving this reduction was assessed.
Scores for individual CCQ domains are calculated as follows: for the “sypmtoms” domain, the sum of the scores assigned to answers to questions 1, 2, 5, and 6 divided by 4; for the “mental state” domain, the sum of the scores assigned to answers to questions 3 and 4 divided by 2; and for the “functional status” domain, the sum of the scores assigned to answers to questions 7, 8, 9, and 10 divided by 4. An absolute reduction in the score for individual CCQ domains between Visit 1 and Visit 2 was considered a therapeutic success. The reduction was calculated by subtracting the score obtained at Visit 1 from the score obtained at Visit 2. The results lower than 0 were interpreted as therapeutic success.
For the assessment of patient general condition by a physician, the PGE was used. The patient’s state was evaluated on an 8‑point scale (1–2: poor; 3–4: satisfactory; 5–6: good; 7–8: excellent).
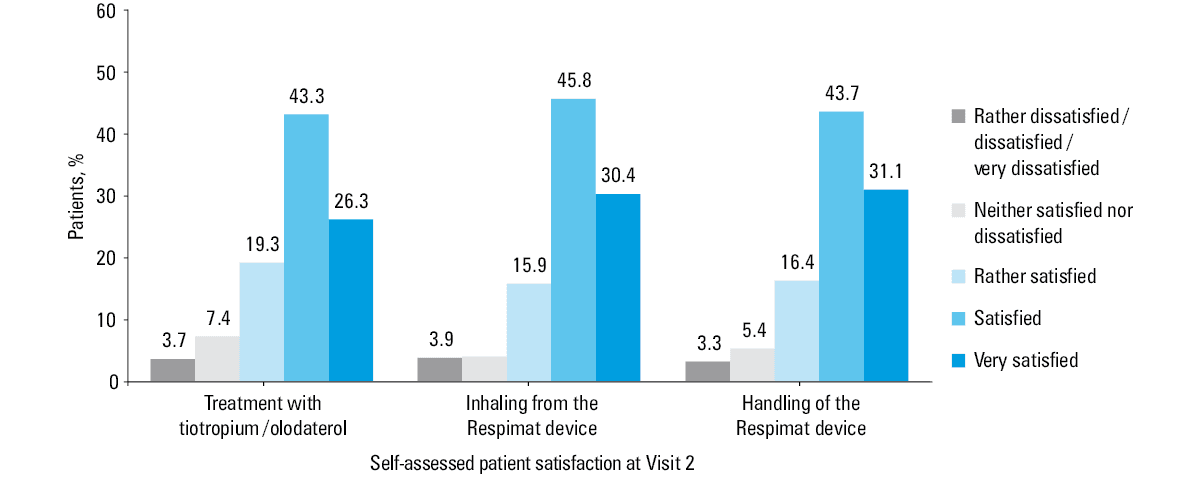
Patient satisfaction with the tiotropium / olodaterol treatment and with handling of the Respimat device was self‑measured on a 7‑point scale using a survey with the following answers: “very dissatisfied” (1), “dissatisfied” (2), “rather dissatisfied” (3), “neither satisfied nor dissatisfied” (4), “rather satisfied” (5), “satisfied” (6) and “very satisfied” (7).
Statistical analysis
Descriptive statistics are presented as frequencies and percentages for categorical variables and medians with interquartile ranges (IQRs) for continuous variables. Statistical significance of differences between percentages of patients achieving therapeutic success was evaluated by the Fisher exact test. Analyses of factors influencing the therapeutic success were performed using uni- and multivariable logistic regression. Results are presented as odds ratios with respective 95% CIs. Calculations were performed using R 4.0.2 statistical software (R Foundation for Statistical Computing, Vienna, Austria)17 and a P value of less than 0.05 was considered significant. In Supplementary material, Table S1, presenting proportions of the patients achieving therapeutic success measured by the CCQ reduction, 2 age groups were distinguished, in line with the age groups analyzed in the NIS‑CCQ study.13 Supplementary material, Table S2 presents the improvement in the PGE score and distinguishes 4 age groups, allowing for a more detailed analysis.
Results
Baseline characteristics of the study group
The study group comprised 526 patients, with a mean (SD) age of 67 (9.1) years. The majority of patients (64.1%) were men. Almost half of the patients (47.7%) were current smokers, and the other half were ex‑smokers (49.2%). According to the 2018 GOLD classification, more than half of the patients were categorized as GOLD B (51.9%), followed by GOLD D (40.5%), and GOLD C (7.6%). Comorbidities were reported in 57.4% of the patients, and the most frequent one was cardiovascular disease, which occurred in 40.5% of the patients. None of the 43 patients with respiratory diseases other than COPD were diagnosed with concomitant asthma. At baseline, the most numerous group were treatment‑naïve patients, that is, not previously treated with either LAMA, LABA, or ICS (44.1%), followed by patients using LAMA or LABA in monotherapy (36.3%). The remaining participants were treated with ICS or with combinations of LAMA or LABA and ICS. Baseline characteristics of the patients are presented in Table 1.
Parameter | Value | |
Data are presented as number (percentage) of patients unless indicated otherwise.
Abbreviations: ICS, inhaled corticosteroids; IQR, interquartile range; LABA, long‑acting β2 agonists; LAMA, long‑acting muscarinic antagonists; others, see Figure 1 | ||
Age, y, mean (SD) | 67 (9.1) | |
Sex | Female | 189 (35.9) |
Male | 337 (64.1) | |
Smoking status | Smoker | 251 (47.7) |
Ex‑smoker | 259 (49.2) | |
Never smoker | 16 (3.1) | |
Time from COPD diagnosis, y, median (IQR) | 5 (2.0–10.0) | |
mMRC classification | Grade 0 | 4 (0.8) |
Grade 1 | 36 (6.8) | |
Grade 2 | 295 (56.1) | |
Grade 3 | 176 (33.5) | |
Grade 4 | 15 (2.9) | |
GOLD group | B | 273 (51.9) |
C | 40 (7.6) | |
D | 213 (40.5) | |
Airflow limitation severity (GOLD grade) | 1 (mild) | 38 (7.2) |
2 (moderate) | 316 (60.1) | |
3 (severe) | 140 (26.6) | |
4 (very severe) | 26 (4.9) | |
Missing | 6 (1.1) | |
Exacerbations within the last 12 months before the initial visit | 0 | 152 (28.9) |
1 | 183 (34.8) | |
2 | 144 (27.4) | |
3 | 34 (6.5) | |
4 | 8 (1.5) | |
5 | 1 (0.2) | |
6 | 2 (0.4) | |
8 | 2 (0.4) | |
Nonsevere (not requiring hospitalization) COPD exacerbations within the last 12 months | 0 | 220 (41.8) |
1 | 147 (27.9) | |
2 | 128 (24.3) | |
3 | 23 (4.4) | |
4 | 4 (0.8) | |
5 | 1 (0.2) | |
6 | 1 (0.2) | |
8 | 2 (0.4) | |
Hospitalizations due to exacerbations within the last 12 months before the initial visit | 0 | 413 (78.5) |
1 | 103 (19.6) | |
2 | 10 (1.9) | |
Concomitant diseases | Any type | 302 (57.4) |
Cardiovascular | 213 (40.5) | |
Metabolic / endocrinological | 83 (15.8) | |
Gastrointestinal / hepatobiliary | 35 (6.7) | |
Neurological | 18 (3.4) | |
Allergic | 14 (2.7) | |
Respiratory (except COPD) | 43 (8.2) | |
Psychiatric | 2 (0.4) | |
Renal / urogenital | 24 (4.6) | |
Other | 50 (9.5) | |
ICS treatment at baseline | Yes | 104 (19.8) |
No | 422 (80.2) | |
COPD treatment at baseline | ICS | 15 (2.8) |
LAMA | 52 (9.8) | |
LAMA + ICS | 5 (0.9) | |
LABA | 139 (26.4) | |
LABA + ICS | 84 (16.0) | |
No treatment with either LAMA or LABA or ICS at baseline | 232 (44.1) | |
Treatment success assessed using the Clinical COPD Questionnaire
Treatment success was achieved in 375 patients (72.4%). The treatment success analyses for individual CCQ domains demonstrated that in 365 patients (70.5%) the therapy was successful with respect to the symptoms, in 340 (65.6%) with respect to the functional state, and in 336 (64.9%) with respect to the mental state (Figure 2). The median (IQR) change of the total CCQ score between Visit 1 and Visit 2 was 0.7 (0.3–1.4) points. Median (IQR) reductions in the scores for individual CCQ domains between Visit 1 and Visit 2 were: 0.75 (0.25–1.5) points, 0.75 (0.25–1.25) points, and 0.5 (0.00–1.5) points, for symptoms, functional state, and mental state, respectively.
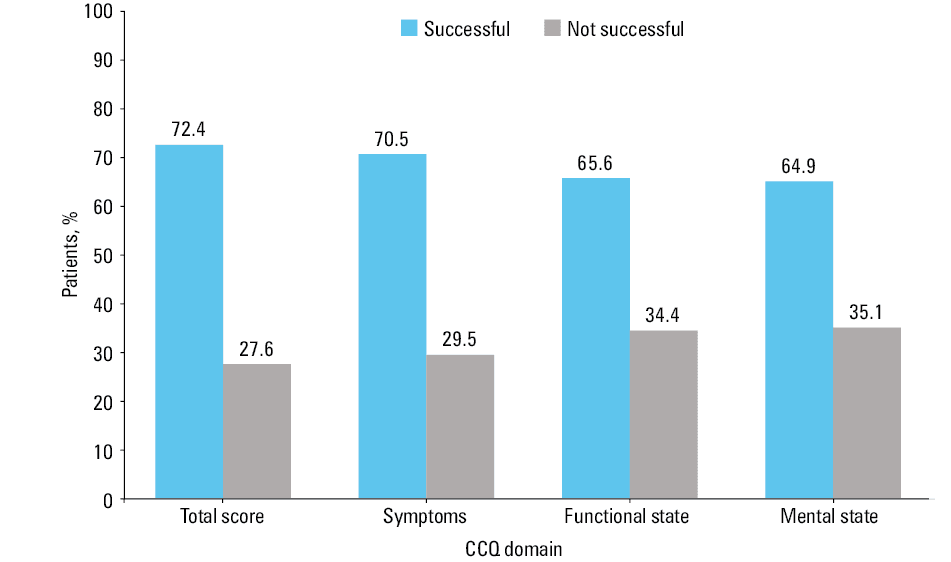
Abbreviations: see Figure 1
The proportion of patients achieving therapeutic success was the highest in the treatment‑naïve group (83.4% of the patients not previously treated with either LAMA, LABA, or ICS) as compared with 73.3% of the patients previously treated with ICS, 62.6% of the patients treated with LAMA or LABA monotherapy, and 64.4% of those treated with LAMA and ICS or LABA and ICS (P <0.001). The therapeutic success was achieved regardless of the degree of COPD severity, as assessed by: (1) the GOLD group: therapeutic success achieved by 82.9% of the patients assigned to a GOLD group D, 67.4% of those assigned to group B, and 50.0% of those assigned to group C (P <0.001); (2) spirometric grades of airflow limitation: success achieved by 76.0% of individuals with very severe (GOLD 4), 77.5% of those with severe (GOLD 3), 72.2% of those with moderate (GOLD 2), and 47.7% of those with mild (GOLD 1) airflow limitation (P = 0.003); (3) modified Medical Research Council Dyspnea Scale (mMRC) grade: success achieved by 74.3% of patients with grades 2 to 4 and 50.0% of those with grade 0 or 1 (P <0.001). The therapy was successful in 80.0% of patients who were hospitalized or experienced more than 2 COPD exacerbations within 12 months before inclusion in the study, in 70.6% of patients with a single exacerbation, and in 64.9% of those without any exacerbation (P = 0.007) (Supplementary material, Table S1).
Uni- and multivariable regression analyses of therapeutic success measured by the CCQ score change showed that the severity of airflow limitation (GOLD grades 2–4), mMRC classes 2 and 3 to 4, as well as exacerbations or hospitalizations within the last 12 months before inclusion in the study predicted a better response to the tiotropium/olodaterol treatment (Figure 3). Generally, the patients with more severe airflow limitation (GOLD grades 3 and 4) had a greater chance of achieving therapeutic success. Notably, the duration of COPD and smoking status did not predict the treatment success.
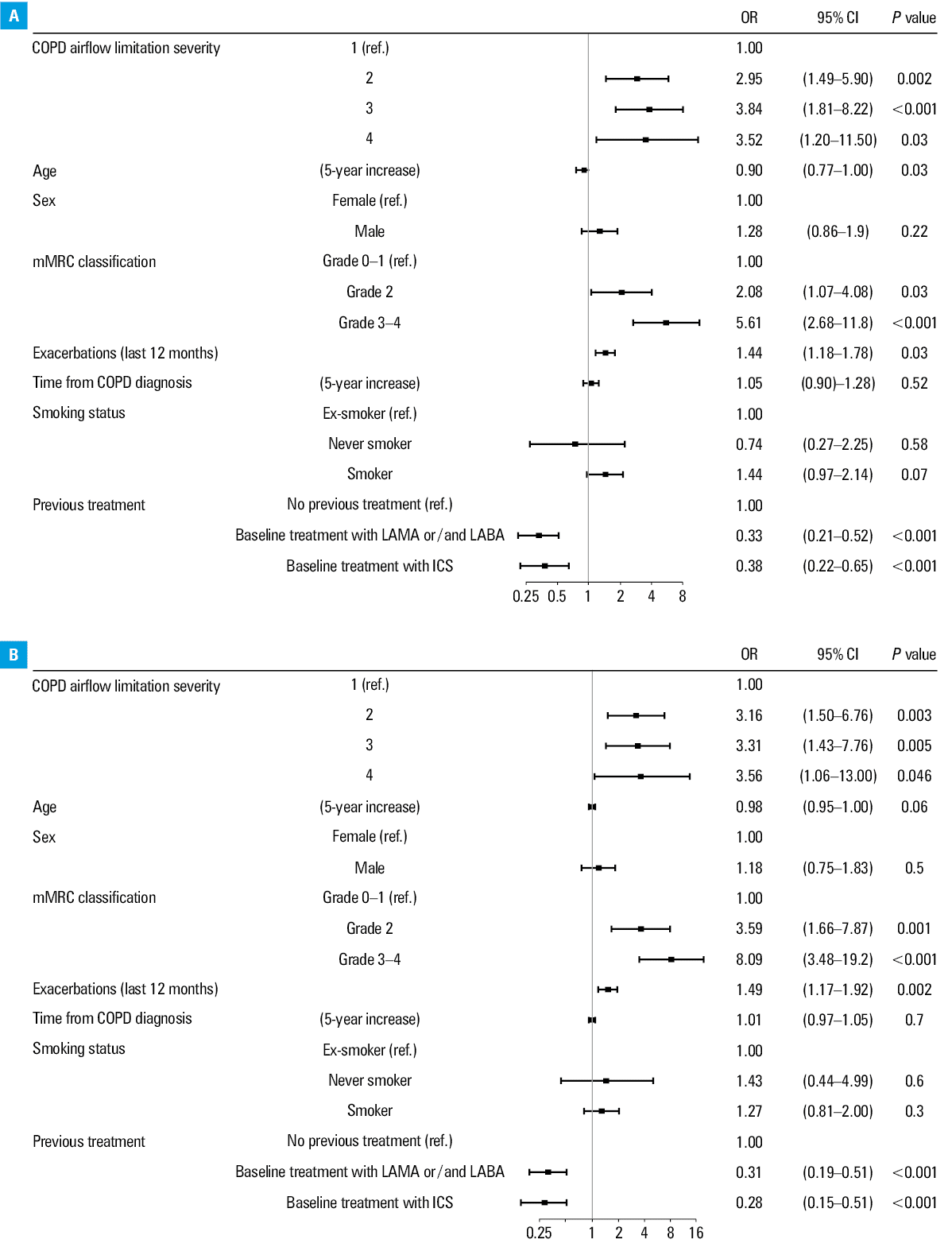
Abbreviations: OR, odds ratio; others, see Figure 1 and Table 1
Univariable and multivariable regression analyses of the impact of previous treatment on therapeutic success showed that the patients treated with ICS before enrollment (both using ICS monotherapy and dual therapy with LABA/ICS or LAMA/ICS) as well as those treated with LAMA or LABA monotherapy, had a significantly lower chance of success than the treatment‑naïve participants. In addition, the regression analysis showed a significant, even though relatively small influence of older age on lowering the chance of achieving the therapeutic success (P = 0.03).
Physician’s Global Evaluation of patients’ general condition and self‑assessment of patients’ satisfaction
The results of PGE demonstrated that after 6 weeks of treatment with tiotropium / olodaterol, the percentage of patients in excellent and good condition increased from 44% to 81.6% (Figure 4).
As in the case of the CCQ, the PGE results indicated that the therapy was more successful in patients at more severe stages of the disease (Supplementary material, Table S2). Among the patients whose PGE score improved by at least 1 point, the patients with mMRC grades 2 to 4 accounted for 93.9% of the group (vs 6.1% with grade 0 or 1, P = 0.044), those categorized into GOLD group B accounted for 46.6%, and those categorized into group D constituted 47.2% (vs 6.1% with group C, P <0.001). The patients who experienced more than 2 exacerbations or a hospitalization within 12 months before entry into the study accounted for 41.9% of the individuals with a PGE improvement by at least 1 point (vs 34.6% of patients with 1 exacerbation and 23.5% of patients without any exacerbation; P <0.001). With respect to age, people younger than 60 years were the most numerous subgroup among the patients with a PGE improvement (31.1% vs 25.1% of those aged 60–70 years, 19.6% of those aged 70–80 years, and 23.7% of those above 80 years of age); however, these differences were not significant.
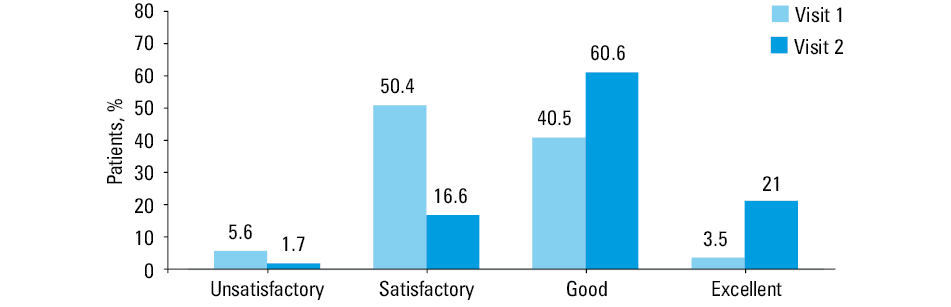
Regarding the self‑assessment of patient satisfaction, at Visit 2, most patients (69.6%) considered themselves very satisfied or satisfied with the tiotropium / olodaterol treatment. The cumulative percentage of the patients who were rather dissatisfied, dissatisfied, and very dissatisfied was 3.7%. Comparable results were obtained with respect to satisfaction with inhaling from and handling of the Respimat device (Figure 5). Moreover, almost all patients (94.4%) expressed their willingness to continue the treatment. Data on the patient satisfaction were missing in 9 cases.
Safety
During the study, 15 adverse drug reactions were reported in 8 patients (1.5%). No serious adverse events were reported. Details are given in Supplementary material, Table S3.
Discussion
This post‑hoc analysis of the NIS‑CCQ study13 aimed to evaluate the changes in clinical control of COPD after 6 weeks of treatment with tiotropium / olodaterol in the Polish population, with the use of the CCQ. Therapeutic success was achieved in 72.4% of the patients. Furthermore, improvement was observed in every domain of the CCQ, reflecting fewer symptoms and a better functional and mental state of the COPD patients.
Beneficial effects of the LAMA/LABA treatment in patients with COPD were previously demonstrated in a systematic review presenting highly consistent results of 24 randomized clinical studies and 8 real‑world studies.11 The use of LAMA/LABA reduced the exacerbation rates and dyspnea, and improved the lung function and HRQoL in comparison with LAMA or LABA monotherapy, LABA/ICS dual therapy, or triple therapy with LAMA, LABA, and ICS. Importantly, real‑world studies confirmed the high efficacy of the LAMA/LABA combination in COPD patients demonstrated in RCTs.11 Thus, our data from the Polish population further uphold the position of dual bronchodilator therapy with LAMA and LABA in the pharmacological management of COPD.
The recently published NIS‑CCQ study13 analyzed data of 4700 COPD patients from Bulgaria, Czech Republic, Hungary, Israel, Lithuania, Poland, Romania, Russia, Slovenia, Switzerland, and Ukraine. For the purpose of the present study, data of the Polish subgroup were extracted, and post‑hoc analyses were performed, which enabled us to provide a more detailed insight into factors that potentially affect patient response to the tiotropium / olodaterol treatment. The general outcomes of both analyses are similar—the majority of patients achieved therapeutic success measured by the CCQ score reduction, and the highest proportion of patients achieving the therapeutic success were either those with the most severe COPD or those not previously treated with LAMA and / or LABA and / or ICS. Nevertheless, differences can be seen between the percentage of patients achieving treatment success: in the NIS‑CCQ study, the percentage was 81.4%, whereas in the Polish subgroup it was 72.4%. Subsequently, smaller proportions of patients who achieved therapeutic success were also observed when the participants were stratified based on the GOLD group, GOLD spirometric grade, or the number of COPD exacerbations and hospitalizations. These interesting outcomes are probably due to the differences between characteristics of the populations. The proportion of patients with the most severe dyspnea (mMRC grade 4), severe and very severe airflow limitation (GOLD 3 and 4), and hospitalizations in the Polish subgroup was considerably lower than in the general NIS‑CCQ population (mMRC 4: 2.9% vs 6.7%; GOLD 4: 4.9% vs 6.9%; GOLD 3: 26.6% vs 33.6%; hospitalizations: 21.5% vs 32.6%). Since the post‑hoc logistic regression analysis of the Polish subgroup revealed that all the abovementioned variables predicted a better response to the tiotropium / olodaterol treatment, it is not surprising that the overall proportion of patients achieving therapeutic success was lower in this subgroup. Moreover, the percentage of treatment‑naïve patients was also smaller in the Polish subpopulation (44.1% vs 56.8%), further explaining the lower overall therapeutic success in this study.
The current GOLD report recommends dual bronchodilation with the LAMA/LABA combination as an initial treatment for GOLD group D patients with a high symptom burden (eg, a COPD Assessment Test [CAT] score >20) or for those whose disease is not adequately controlled by monotherapy at the follow‑up visit.6 The results of our study suggest that the LAMA/LABA combination is beneficial also in other analyzed GOLD groups. This observation is not unique, since the results of other real‑world studies demonstrate that considerable numbers of COPD patients with GOLD group B and even group A benefit from the LAMA/LABA combination therapy.9,12,18 These findings from real‑world studies confirm the broader use of the LAMA/LABA combination, which is already in the clinical practice of many physicians.
We observed that the therapeutic success of tiotropium / olodaterol differed in patient subgroups defined on the basis of medications taken before switching to the LAMA/LABA combination. The highest rate of therapeutic success was observed in the group of treatment‑naïve patients (83.4% of these patients achieved a reduction of the total CCQ score by 0.4 points). The regression analysis also showed that the patients treated with ICS (in mono- or dual therapy with LABA or LAMA) or LAMA or LABA monotherapy before enrollment in the study had a significantly lower chance of success than the treatment‑naïve individuals. These data are in line with the results of other studies demonstrating beneficial effects of tiotropium / olodaterol in the maintenance‑naïve patients with COPD.12,18-20 A pooled analysis of 4 RCTs revealed that initiation of treatment with tiotropium / olodaterol in the patients naïve to LAMA, LABA, and ICS resulted in greater improvements in their lung function, dyspnea severity, and health status in comparison with tiotropium monotherapy.21 Similar results were also published on different LAMA/LABA combinations, including umeclidinium / vilanterol and glycopyrronium / indacaterol, as compared with LAMA monotherapy in maintenance‑naïve patients.22-24 In our study, the therapeutic success of tiotropium / olodaterol, however less pronounced, was also observed in the COPD patients previously treated with ICS, LAMA, or LABA in monotherapy or those treated with LAMA or LABA and ICS in dual therapy. Switching from baseline LAMA or LABA monotherapy or LABA/ICS to the combination of LAMA/LABA (glycopyrronium / indacaterol) was reported to significantly reduce the risk of clinically important deterioration and improve the total CAT score to the greatest degree.25,26 Moreover, data from RCTs on patients with infrequent exacerbations also demonstrate that the change of treatment from the LABA/ICS to the LAMA/LABA combination improves symptom severity and lung function.27,28 Algorithms and guidelines on the withdrawal of inhaled ICS in COPD patients were developed, and can facilitate the decision process concerning the ICS discontinuation.29,30 Together, all these data suggest that the FDC of tiotropium / olodaterol may be beneficial to the majority of patients with COPD irrespective of prior therapy, and could probably be used as first‑line therapy in treatment‑naïve patients.
Our results show that the effectiveness of the tiotropium / olodaterol therapy was higher in the patients with more severe dyspnea (assessed with mMRC). However, even in the patients with mild breathlessness, the treatment led to therapeutic success in 50% of cases. Individuals with less prominent COPD symptoms are classified into groups A and C according to the GOLD criteria. Patients with the GOLD group A were not included in this study. However, there was a small subgroup of group C patients (40 individuals), and half of them achieved therapeutic success. Although the small size of this group did not allow for making conclusive statements, this result indicates the need for further exploration of the potential benefits of the tiotropium / olodaterol treatment in less symptomatic COPD patients. A similar observation was made in the OTIVACTO study, 12 where even the GOLD group A COPD patients benefited from the tiotropium / olodaterol treatment.
Our data showed that patients with a history of exacerbations (especially frequent exacerbation phenotype) had a greater probability of achieving therapeutic success with the tiotropium / olodaterol treatment. However, 64% of the patients without any exacerbation and 70% of the patients with only a single exacerbation also benefited from such treatment. Therefore, tiotropium / olodaterol may be considered a therapeutic possibility irrespective of the exacerbation burden. Interestingly, this study showed that the duration of COPD did not affect the chance of benefiting from the use of tiotropium / olodaterol, which further implies that this drug combination acts therapeutically at every stage of the disease, and even from its onset. Altogether, the LAMA/LABA combination should be considered a treatment option in COPD patients irrespective of the disease duration and exacerbation rate.
Our results showed that therapeutic success of the tiotropium / olodaterol treatment was also reflected by an improvement in the PGE score. At Visit 1, most patients were in a satisfactory or unsatisfactory condition, whereas after 6 weeks of treatment with LAMA/LABA, the majority were categorized as being in a good or excellent condition. The improvement in the PGE score at Visit 2 was accompanied by a high level of patient satisfaction with the treatment. At Visit 2, around 80% of the patients evaluated themselves as very satisfied, satisfied, or rather satisfied with the tiotropium / olodaterol treatment, and with inhaling from and handling of the Respimat device. The high level of satisfaction of patients resulted in their willingness to continue the treatment after the study. Other real‑world studies demonstrated comparable results regarding a parallel improvement in patients’ self‑assessed satisfaction and PGE scores in COPD populations treated with tiotropium / olodaterol.23,31 Previous studies also reported a high level of patient satisfaction with the Respimat device, its reliability and ease of use.32-35
This study has certain strengths and limitations. The strong point is that it is the first real‑world study to analyze the use of tiotropium / olodaterol in an FDC in the Polish COPD population. The lack of previous studies encompassing the Polish population was the main reason for our post‑hoc analysis of data from the Polish subgroup of the NIS‑CCQ study.13 The rationale for the detailed analysis of the Polish population also results from the fact that Poland is a country with a very high level of air pollution, strongly exceeding the limits for particulate matter (PM 2.5 and 10) and benzo[a]pyrene. Therefore, the Polish population is especially exposed to the environmental risks of COPD development.14 This unfavorable situation is associated with the high prevalence of COPD in Poland, which exceeds 20% in some regions of the country.36 Interestingly, the low level of satisfaction with air quality (reflecting the level of air pollution) was demonstrated to be associated with COPD in a questionnaire‑based study of a Chinese population.37 It confirms not only the negative role of air pollutants in COPD but also the applicability of patient questionnaires as a reliable tool for data collection. Thus, the use of the CCQ in our study to assess the clinical control of COPD should also be considered a strong point. Moreover, the CCQ reflects the patient status better than the CAT and is preferred by COPD patients.38
The limitations of the study are mainly associated with its noninterventional, observational design, which has some weaknesses, such as the lack of a control group. Additionally, the follow‑up period in this study was short. Although a 6‑week follow‑up reduces the risk of recall bias, it is not long enough to collect data on the disease exacerbation or other long‑term events related to the treatment. It would be therefore of great value to conduct other real‑world studies with longer follow‑up periods (eg, 6 months), allowing for a long observation of tiotropium / olodaterol treatment effects. Another limitation of the study was a relatively small size of the study group, especially with respect to the number of patients previously treated with ICS (102 vs 187 for LAMA- or LABA‑treated and 229 for treatment‑naïve patients). The possible explanation of this situation is recruitment bias or physicians’ unwillingness to change the treatment from the ICS / bronchodilator therapy to the LAMA/LABA combination therapy.
Overall, the studies based on questionnaires measuring patient satisfaction are subjective, which may be considered a limitation. Nonetheless, these subjective assessments provide an insight into patients’ self‑perceived health state and present valuable real‑world data.
In conclusion, the results of this post‑hoc analysis of the NIS‑CCQ study demonstrate that the 6‑week treatment with tiotropium / olodaterol in an FDC improved the clinical control of the disease in COPD patients assessed with the CCQ. Furthermore, the improvement was observed in terms of the general condition of patients evaluated by the PGE, and was accompanied by a high level of patient satisfaction with the treatment. The therapeutic success of the tiotropium / olodaterol treatment was the most pronounced in the patients with more severe COPD and the treatment‑naïve individuals. Importantly, this therapy also proved beneficial in most patients with less advanced disease, without any exacerbation, and in those previously treated with mono- or dual ICS/LABA therapy. Due to the fact that the duration of COPD did not affect the chance of benefiting from tiotropium / olodaterol, our results suggest that this drug combination may be used in a broad group of patients with COPD.
- World Health Organization. Global Burden of Disease Website. http://www.who.int/topics/global_burden_of_disease. Accessed June 2021.
- Hogg JC, Chu F, Utokaparch S, et al. The nature of small‑airway obstruction in chronic obstructive pulmonary disease. N Engl J Med. 2004; 350: 2645‑2653. | Crossref
- Janson C, Marks G, Buist S, et al. The impact of COPD on health status: findings from the BOLD study. Eur Resp J. 2013; 42: 1472‑1483. | Crossref
- Curtis JR, Patrick DL. The assessment of health status among patients with COPD. Eur Respir J Suppl. 2003; 41: 36s‑45s. | Crossref
- van der Molen T, Willemse BW, Schokker S, et al. Development, validity and responsiveness of the Clinical COPD Questionnaire. Health Qual Life Outcomes. 2003; 28: 13. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION