Bland‑White‑Garland syndrome (BWGS), also known as anomalous left coronary artery (LCA) from pulmonary artery (ALCAPA), is considered a very rare condition that comprises 0.25% to 0.5% of all congenital heart defects.1 ALCAPA results in decreased oxygen levels, coronary steal phenomenon, and myocardial ischemia. Symptoms and prognosis depend on the degree of ischemia correlating with the development of collateral circulation to LCA.1 The absence of an adequate collateral supply can lead to myocardial infarction, left ventricle dilation, congestive heart failure, mitral regurgitation, arrhythmia, and sudden cardiac death (SCD).2 Unfortunately, the majority of patients affected by BWGS (90%) die within the first year of life, unless they are operated on. In adults who survived, SCD is the most common cause of death, and it might be the first clinical manifestation. Ventricular fibrillation most often occurs due to myocardial ischemia and degeneration of scar‑related reentrant ventricular tachycardia.2
A 35‑year‑old man, a professional soldier, previously asymptomatic, was admitted to our hospital to diagnose reduced exercise tolerance following SARS‑CoV‑2 infection. Outpatient echocardiography revealed hypokinesia of the basal segment of the lateral wall and akinesia of the apical segments of the anterior wall, with an ejection fraction of approximately 45%. Furthermore, Holter electrocardiogram monitoring detected frequent premature ventricular contractions. Coronary angiography showed a giant and very tortuous right coronary artery (RCA), with a retrograde inflow to the LCA up to the left main (Figure 1A and 1B). The ostium of LCA from the aorta was not visualized. We extended diagnostic evaluation with computed tomography angiography and magnetic resonance imaging (MRI), which confirmed LCA originating from the pulmonary trunk and filling with RCA collaterals (Figure 1C).
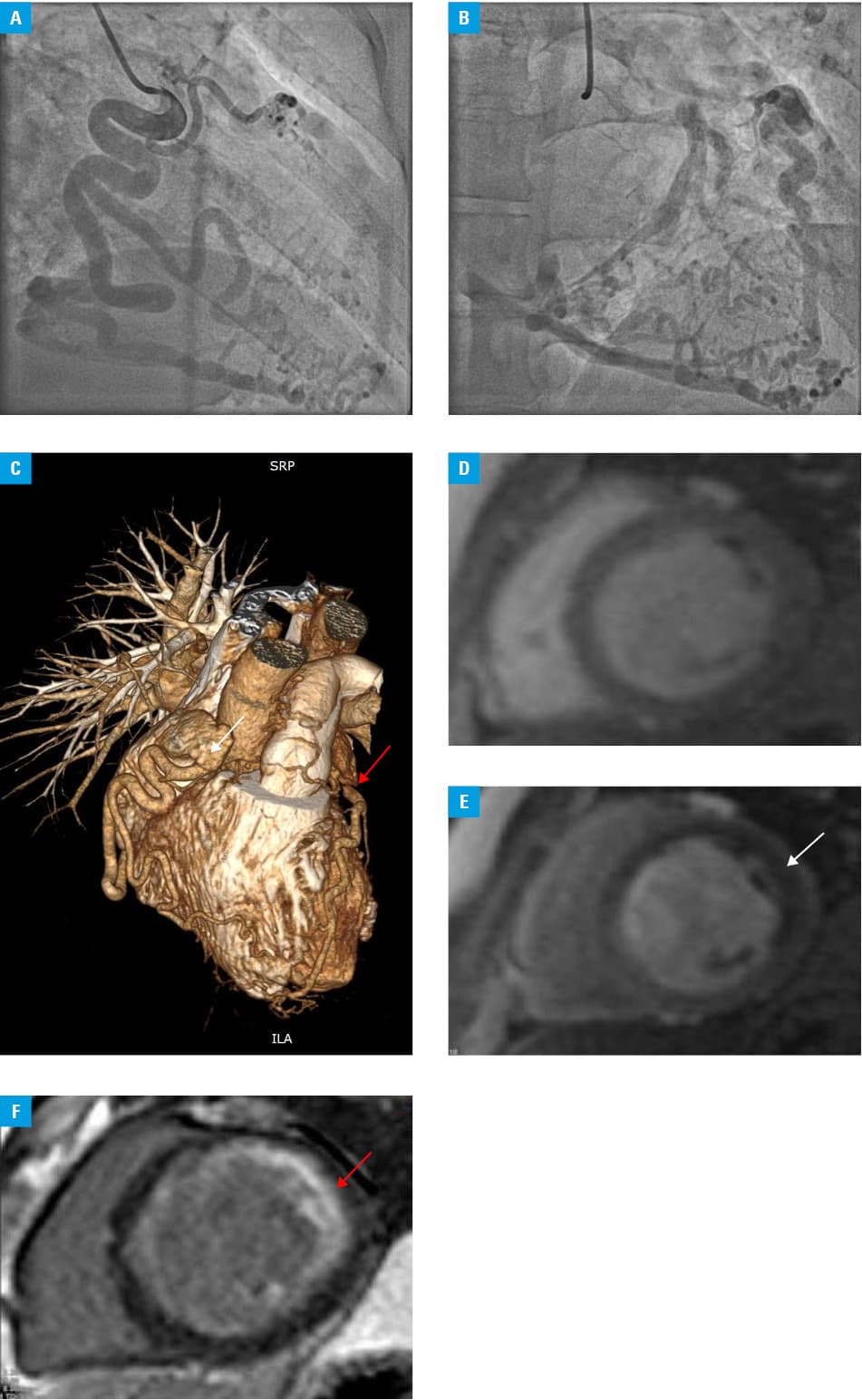
Positive stress perfusion MRI showed regadenoson‑induced myocardial ischemia of the basal segments of the intraventricular septum and anterolateral wall (Figure 1D-1E). Moreover, MRI revealed a myocardial infarct scar involving 75% of thickness of the apical wall segments and 25% to 50% of the non‑apical anterior and lateral wall segments (Figure 1F).
Following the discussion of the therapeutic options, the patient did not agree to the invasive approach and opted for the conservative treatment.
Unique to our case is the diagnosis of BWGS only in adulthood, despite intense physical exertion associated with the soldier profession. The American Heart Association guidelines suggest surgery even for asymptomatic patients with ALCAPA.3 There are several surgical approaches, among which LCA reimplantation and Takeuchi operation are the most common.4 The choice of surgical management depends on the patient’s anomalous coronary anatomy and additional cardiac problems. Nevertheless, the conservative management should also be considered in asymptomatic patients with high operational risk.5 Current literature does not unanimously confirm that the surgical approach eliminates the risk of recurring ventricular arrhythmia in patients after SCD. This subject needs further research, as only a few case reports with short follow‑ups have been published.
- Pfannschmidt J, Ruskowski H, de Vivie ER. Bland‑White‑Garland syndrome. Clinical aspects, diagnosis, therapy [in German]. Klin Padiatr. 1992; 204: 328‑334. | Crossref
- Boutsikou M, Shore D, Li W, et al. Anomalous left coronary artery from the pulmonary artery (ALCAPA) diagnosed in adulthood: varied clinical presentation, therapeutic approach and outcome. Int J Cardiol. 2018; 261: 49‑53. | Crossref
- Stout KK, Daniels CJ, Aboulhosn JA, et al. 2018 AHA/ACC guideline for the management of adults with congenital heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation. 2018; 139: e637‑e697. | Crossref
- Cramer JW, Cinquegrani M, Cohen SB. Takeuchi repair of anomalous left coronary artery from the pulmonary artery. J Cardiovasc Comput Tomogr. 2015; 9: 457‑458. | Crossref
- Vizzuso A, Righi R, Zerbini M, et al. An unusual presentation of anomalous left coronary artery from the pulmonary artery (ALCAPA) syndrome in a 70‑year‑old man: a case report. J Med Case Rep. 2018; 12: 308. | Crossref
ARTICLE INFORMATION